I now have all the information needed for a thorough, well-illustrated answer. Here is the complete overview:
Patent Ductus Arteriosus (PDA)
Anatomy & Embryology
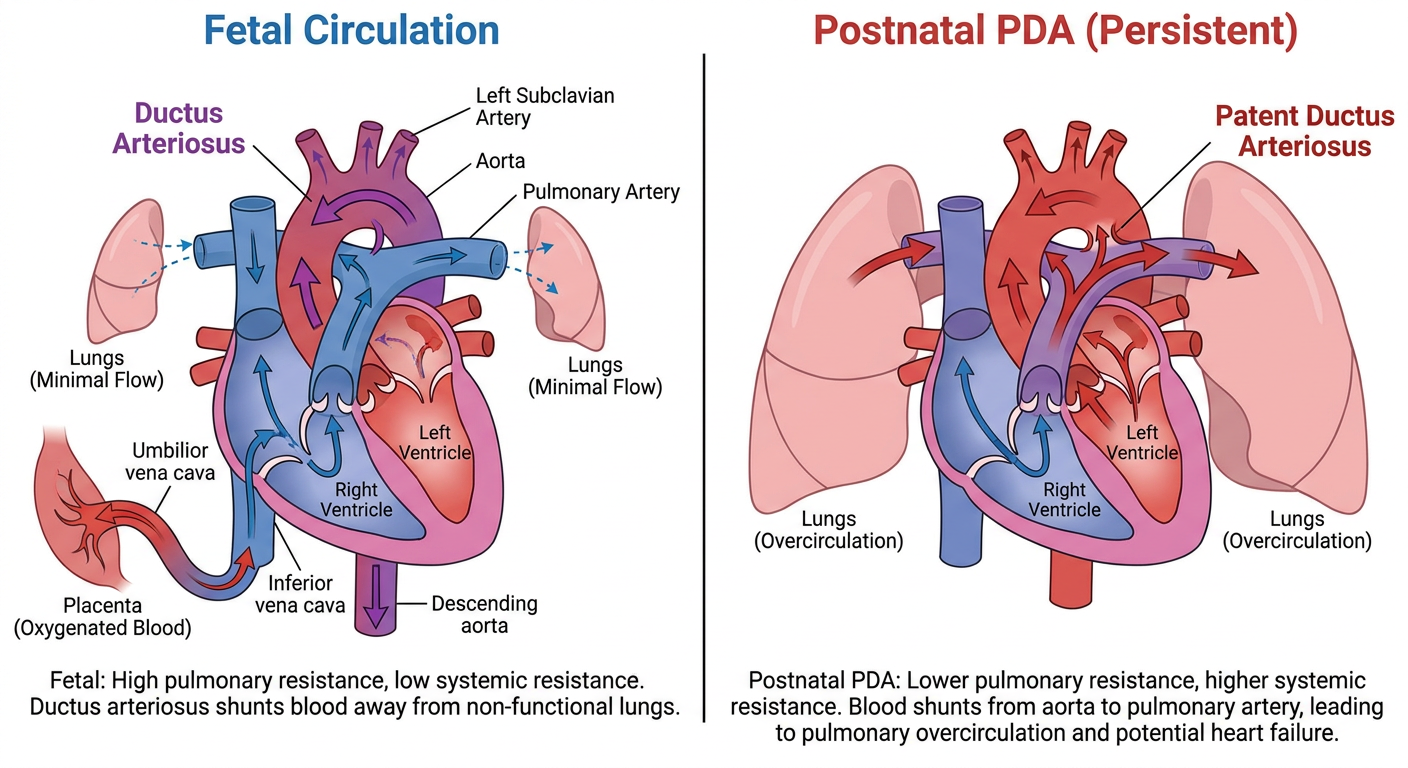
The ductus arteriosus is derived from the sixth aortic arch and connects the main (or left) pulmonary artery to the upper descending thoracic aorta, just distal to the left subclavian artery. In fetal life, ductal flow accounts for approximately 60% of combined ventricular output and is directed exclusively from the pulmonary artery to the aorta (right-to-left), bypassing the fluid-filled, non-functional lungs.
Normal closure occurs in two phases:
- Functional closure: within 10-15 hours of birth, driven primarily by rising arterial oxygen tension causing smooth muscle contraction; also aided by histamines, catecholamines, bradykinin, and acetylcholine.
- Anatomic closure: fibrosis over the first few months leaves behind the ligamentum arteriosum.
The molecular mechanism maintaining fetal ductal patency involves locally produced prostaglandin E2 (PGE2) and prostaglandin I2 (PGI2), which cause active relaxation of ductal smooth muscle. At birth, increased pulmonary blood flow metabolizes these prostaglandins and removal of the placenta eliminates a major source of them, precipitating closure. Failure of TGF-β induction after birth has also been proposed as a mechanism of persistent patency. - The Developing Human, Clinically Oriented Embryology
Epidemiology
| Factor | Detail |
|---|
| Incidence | ~1 in 2,000 live births |
| Sex ratio | Females > Males (2:1) |
| Prematurity | PDA found in 75% of infants at 28-30 weeks gestation |
| Extremely preterm (<28 wks, <1750 g) | Nearly 100% have PDA in the first 24 hours |
| Isolated defect | ~90% of cases |
| Contribution to all CHD | ~7% |
Risk factors for persistence:
-
Prematurity / respiratory distress syndrome (surfactant deficiency)
-
Maternal rubella infection in early pregnancy
-
Hypoxia (high altitude, congenital heart disease)
-
Chromosomal anomalies
-
Associated lesions: coarctation of the aorta, transposition of the great arteries (TGA), pulmonary stenosis/atresia (these create large pressure differentials that physically prevent ductal constriction)
-
Schwartz's Principles of Surgery, 11th Ed. | The Developing Human, Clinically Oriented Embryology
Pathophysiology
After birth, the pulmonary vascular resistance drops over 8-10 weeks. A PDA now produces a left-to-right shunt (aorta → pulmonary artery), reversing the fetal direction. The magnitude of shunting depends on:
- Ductal diameter and length
- Ratio of pulmonary to systemic vascular resistance
Hemodynamic consequences:
- Increased pulmonary blood flow → left atrial and left ventricular volume overload
- Elevated pulmonary artery pressure → right ventricular strain
- Low aortic diastolic pressure → risk of coronary and systemic hypoperfusion
- Tachycardia, tachypnea, ventricular hypertrophy via sympathetic activation
Eisenmenger syndrome (late, ~5% of isolated PDAs):
If untreated, progressive pulmonary hypertension leads to shunt reversal (right-to-left), producing differential cyanosis - the lower body is cyanosed (receives desaturated blood from pulmonary artery via ductus into the descending aorta) while the upper body remains pink.
Clinical Features by PDA Size
| Size | Shunt | Left heart | Pulmonary hypertension | Symptoms |
|---|
| Small | Systolic + diastolic, no dilation | Normal | None | Asymptomatic; risk of infective endarteritis ~0.45%/year after 2nd decade |
| Moderate/Large (restrictive) | Left-to-right throughout cycle | Left atrial/ventricular dilation | Variable | Dyspnea, palpitations, exercise intolerance by 2nd-3rd decade |
| Large (non-restrictive) | Massive L→R shunt | Severe dilation | Severe; may lead to Eisenmenger | Heart failure, cyanosis |
-
Untreated mortality: ~30% overall; two-thirds of patients die by age 60 if large ductus untreated. By the 4th decade, mortality rises to 3-4% per year.
-
Goldman-Cecil Medicine | Schwartz's Principles of Surgery
Clinical Signs & Diagnosis
Classic sign: "Machinery murmur" - a harsh, continuous (systolic + diastolic) murmur heard best at the left infraclavicular area / second intercostal space. Small PDAs may have only a systolic murmur.
Examination:
- Wide/bounding pulse pressure (due to diastolic runoff into pulmonary circulation)
- Hyperdynamic precordium
- No cyanosis in uncomplicated PDA (unless Eisenmenger develops)
Investigations:
| Test | Findings |
|---|
| ECG | Left ventricular strain, left atrial enlargement; right ventricular hypertrophy if pulmonary hypertension |
| CXR | Increased pulmonary vascularity, cardiomegaly |
| Echocardiography | Gold standard - demonstrates patency, estimates shunt size, assesses chamber dilation |
| Cardiac catheterization | Only needed if pulmonary hypertension suspected |
- Schwartz's Principles of Surgery, 11th Ed.
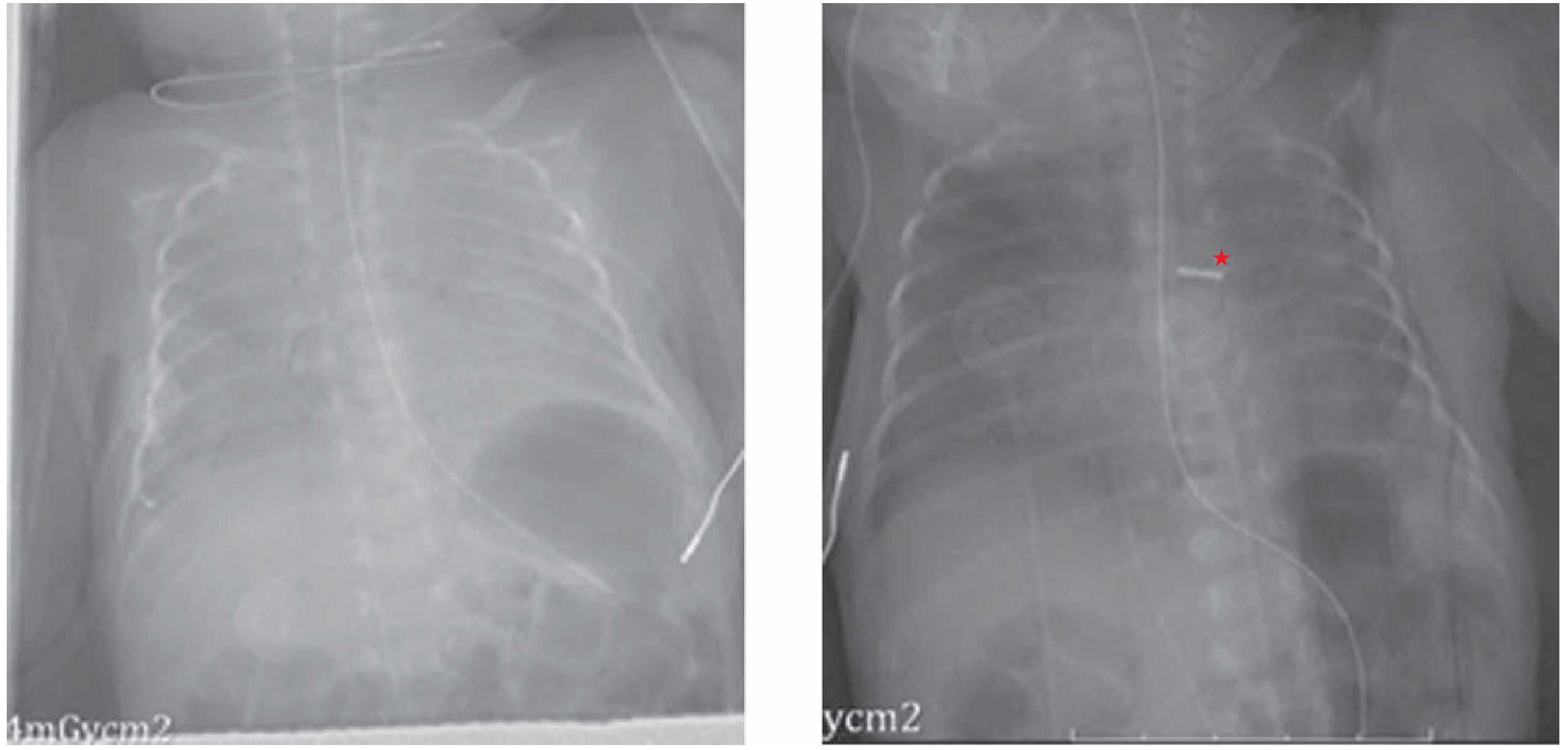
CXR before and after PDA ligation - note dramatic clearing of the lung fields after surgical clip placement (red star):
Treatment
The presence of a persistent PDA is sufficient indication for closure due to the increased mortality and risk of endocarditis. Closure is generally contraindicated in Eisenmenger syndrome (fixed pulmonary hypertension) as it may worsen outcomes.
1. Pharmacological (Premature Infants Only)
- Indomethacin or ibuprofen (COX inhibitors - block prostaglandin synthesis)
- Term infants are generally unresponsive to these agents (pharmacological therapy is therefore not useful in term neonates)
- Contraindications: necrotizing enterocolitis, renal insufficiency, bleeding disorders
2. Catheter-Based (Transcatheter) Closure
Now the preferred approach for most older infants, children, and adults with small-to-moderate PDAs:
- Rashkind double-umbrella device
- Gianturco coils (coil embolization)
- Occlutech/Amplatzer ductal occluder devices
Complications: thromboembolism, incomplete occlusion, vascular injury, device embolization, endocarditis. May not be feasible in very premature infants due to small vessel size.
- Generally preferred for older patients (>5 years) and smaller ducts (<3 mm).
3. Surgical Closure
Two approaches:
-
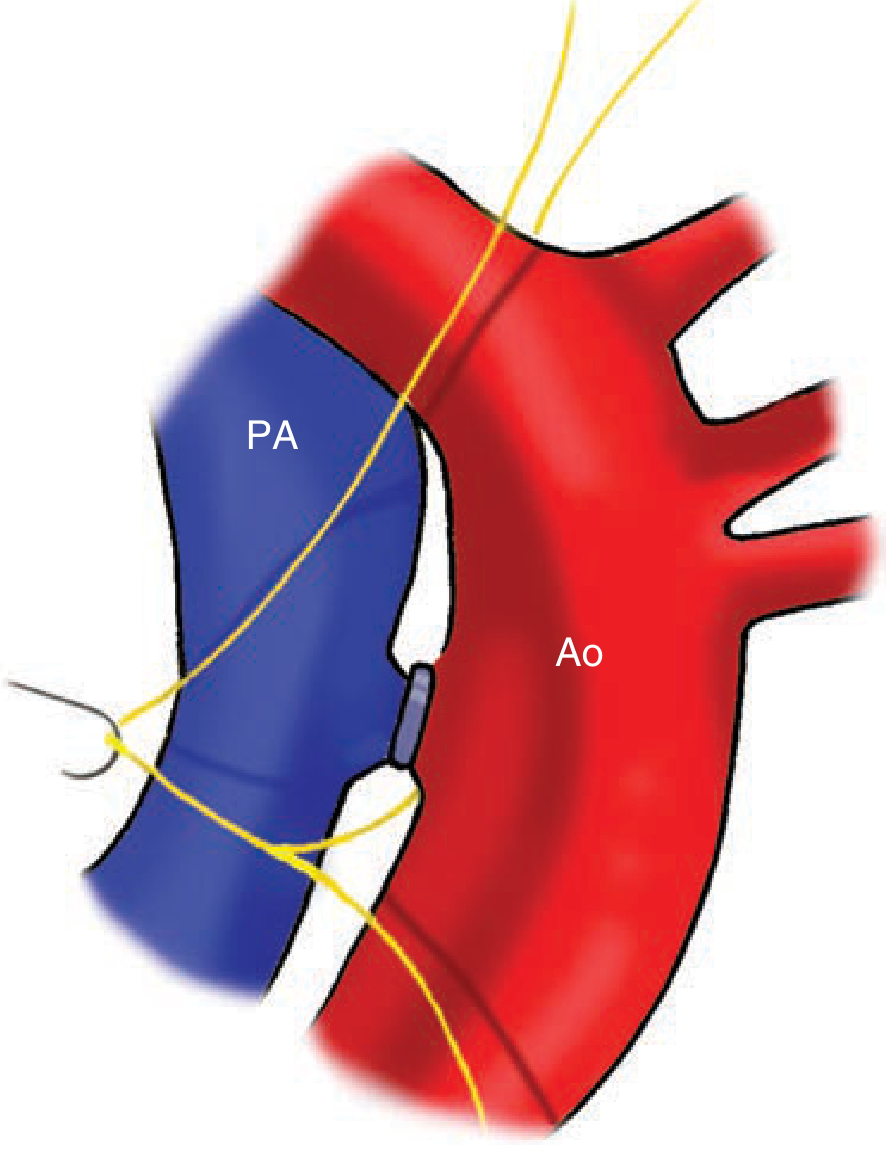
Open (posterior lateral thoracotomy): 3rd or 4th intercostal space, left side. Lung retracted anteriorly. PDA is ligated with a surgical clip or permanent suture. Care must be taken to protect the recurrent laryngeal nerve, which wraps around the PDA.
- For a short, broad ductus: division between vascular clamps with oversewing of both ends.
- CPB may rarely be needed for a very large ductus.
-
Video-Assisted Thoracoscopic Surgery (VATS): Metal clips placed thoracoscopically. Offers few advantages over open approach.
-
Median sternotomy: reserved for PDA combined with other lesions requiring repair.
-
Preferred for preterm newborns and young children where catheter access is limited.
Key Points Summary
| Feature | Detail |
|---|
| Embryology | 6th aortic arch; fails to close → no ligamentum arteriosum |
| Mechanism of patency | PGE2/PGI2 maintain dilation; hypoxia, prematurity impair closure |
| Shunt direction | L→R (aorta to pulmonary artery) post-natally |
| Classic murmur | Continuous "machinery" murmur |
| Key risk | Infective endarteritis (small PDA), heart failure, Eisenmenger (large PDA) |
| Drug treatment | Indomethacin/ibuprofen (premature only) |
| Surgical landmark | Recurrent laryngeal nerve wraps around PDA |
| Closed fetal remnant | Ligamentum arteriosum |
Sources: Schwartz's Principles of Surgery, 11th Ed. | Goldman-Cecil Medicine | Robbins & Kumar Basic Pathology | The Developing Human, Clinically Oriented Embryology