Liver chirrosis
Reading File
Finding Sources
Searching PubMed
"liver cirrhosis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, authoritative content from Goldman-Cecil Medicine and Robbins Pathology. I can now write a thorough answer.
Liver Cirrhosis
Definition
Cirrhosis is the diffuse transformation of the liver into regenerative parenchymal nodules surrounded by fibrous bands. It represents the end stage of any chronic liver disease and is characterized by disruption of the normal hepatic architecture, vascular distortion, and progressive loss of functional liver mass.
- Robbins & Kumar Basic Pathology, p. 598
- Goldman-Cecil Medicine, p. 1614
Etiology / Causes
Major causes (globally):
- Alcoholic liver disease
- Non-alcoholic fatty liver disease (NAFLD/MASLD)
- Chronic hepatitis B
- Chronic hepatitis C (less common now due to effective antivirals)
Less common causes (<2% each):
- Cholestatic/autoimmune: Primary biliary cirrhosis, primary sclerosing cholangitis, autoimmune hepatitis
- Metabolic: Hemochromatosis, Wilson disease, alpha-1 antitrypsin deficiency, glycogen storage diseases, porphyria
- Mechanical obstruction: Biliary atresia, cystic fibrosis
- Vascular: Budd-Chiari syndrome, veno-occlusive disease, right-sided heart failure
- Drugs and toxins
- Cryptogenic cirrhosis: no identifiable cause
Goldman-Cecil Medicine, p. 1615 (Table 139-1)
Pathogenesis
1. Hepatic Stellate Cell Activation
The central mechanism is activation of hepatic stellate cells (Ito cells / perisinusoidal cells), which reside in the space of Disse between hepatocytes and sinusoidal endothelial cells.
- At rest: stellate cells are quiescent and store retinoids (vitamin A)
- In response to injury: they lose vitamin A, proliferate, develop rough ER, and secrete extracellular matrix (collagen types I and III, sulfated proteoglycans, glycoproteins)
- They transform into contractile myofibroblasts
2. Sinusoidal Capillarization
Normal hepatic sinusoids lack a basement membrane and have fenestrated endothelium (100-200 nm), permitting large molecules (up to 250,000 Da) to pass freely. Collagen deposition in the space of Disse leads to defenestration of sinusoidal endothelial cells ("capillarization"), reducing exchange between plasma and hepatocytes and narrowing sinusoidal diameter further.
3. Fibrosis and Nodule Formation
Progressive collagen deposition links portal tracts to each other (or to central veins), trapping regenerating hepatocyte clusters into nodules. The balance between fibrosis progression and regression (which can occur after disease cure or remission) dictates clinical outcome.
Goldman-Cecil Medicine, p. 1614-1615
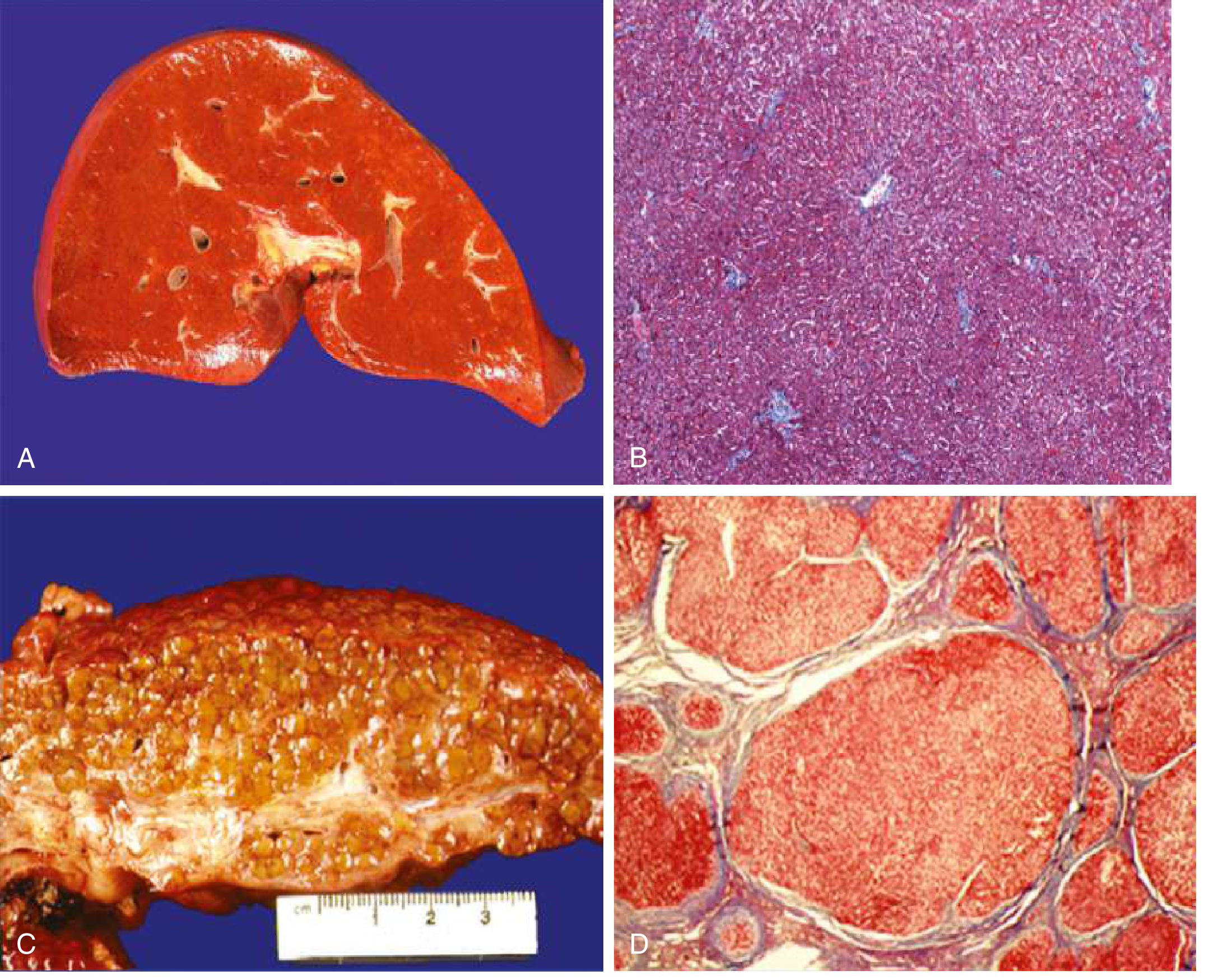
Morphology
- Gross: Liver surface shows bulging, irregularly sized regenerative nodules. Color may be tawny-orange (alcoholic) or dark (viral/other)
- Micro: Rounded parenchymal nodules surrounded by fibrous septa (Masson trichrome stain highlights collagen in blue); ductular reactions (stemcell-derived ductlike structures) prominent
- Micronodular cirrhosis: nodules <3 mm, typically alcoholic
- Macronodular cirrhosis: nodules >3 mm, typically viral hepatitis
- Regression features: thinner, denser-compacted scars that fragment over time
Robbins & Kumar, p. 598-599
Clinical Staging
Cirrhosis is classified into two prognostically distinct stages:
| Stage | Definition | Key mechanism |
|---|---|---|
| Compensated | No decompensating event; often asymptomatic | Fibrosis/nodules without functional failure |
| Decompensated | Ascites, variceal hemorrhage, encephalopathy, or jaundice | Portal hypertension + liver insufficiency |
About 40% of patients are asymptomatic until advanced disease. Early symptoms are nonspecific: anorexia, weight loss, weakness.
Pathophysiology of Complications
Portal Hypertension
Results from two mechanisms:
- Increased sinusoidal resistance - fixed component (fibrosis/nodule compression) + functional component (active vasoconstriction from intrahepatic NO deficiency and enhanced vasoconstrictors)
- Increased portal venous inflow - splanchnic arteriolar vasodilation driven by NO and other vasodilators produced in response to portal hypertension
Early: spleen enlarges and sequesters platelets (hypersplenism). Later: collateral vessels develop (portosystemic shunts).
Esophagogastric Varices
- Develop in ~40% of advanced cirrhosis
- Most clinically important consequence of portal hypertension
- Risk of massive, potentially fatal hematemesis (especially with coagulopathy)
Ascites
- ~85% of ascites cases are due to cirrhotic portal hypertension
- Fluid is a transudate: protein <3 g/dL, serum-to-ascites albumin gradient (SAAG) ≥1.1 g/dL
Hepatic Encephalopathy
- Occurs at ~2-3% per year in cirrhotic patients
- Spectrum: subclinical → grade 1 (sleep inversion, forgetfulness) → grade 2 (confusion, disorientation) → grade 3 (lethargy, profound disorientation) → grade 4 (coma)
- Hallmark sign: asterixis (flapping tremor)
- Characteristic breath: fetor hepaticus (sweet-smelling)
- Pathogenesis: combined effect of portal hypertension (shunting of gut toxins, especially ammonia) + liver insufficiency
Spontaneous Bacterial Peritonitis (SBP)
- ~1/3 of cirrhotics admitted to hospital develop bacterial infection
- Presenting features: fever, jaundice, abdominal pain, rebound tenderness - but up to 1/3 are initially asymptomatic
- Can also present as encephalopathy, acute kidney injury, or shock
Hepatorenal Syndrome (HRS)
- Prerenal kidney injury from maximal peripheral vasodilation + intense renal artery vasoconstriction + hormonal sodium/water retention
- HRS-AKI (formerly Type 1): rapidly progressive, creatinine rise within 2 weeks - poor prognosis
- HRS-non-AKI (formerly Type 2): slower, associated with diuretic-refractory ascites
Pulmonary Complications
- Hepatopulmonary syndrome: intrapulmonary vascular shunting - presents with exertional dyspnea
- Portopulmonary hypertension: elevated pulmonary arterial pressure
Hyperestrogenemia (males)
Impaired estrogen catabolism leads to:
- Palmar erythema
- Spider angiomas (skin)
- Gynecomastia, testicular atrophy
Prognostic Scoring
Child-Pugh Score
Incorporates: bilirubin, albumin, PT/INR, ascites, encephalopathy
- Classes A/B/C - used for surgical risk and prognosis
MELD Score
MELD = [0.957 × ln(creatinine) + 0.378 × ln(bilirubin) + 1.12 × ln(INR) + 0.643] × 10
MELD-Na: If MELD ≥12, adjusted with serum sodium:
MELD-Na = MELD(0) + 1.32 × (137 - Na) - [0.033 × MELD(i) × (137 - Na)]
MELD-Na is the primary tool for organ allocation on liver transplant waitlists.
Goldman-Cecil Medicine, p. 1615 (Table 139-2)
Management Overview
| Problem | Treatment |
|---|---|
| Underlying cause | Antivirals (HBV/HCV), alcohol abstinence, weight loss (NAFLD) |
| Portal hypertension (prophylaxis) | Non-selective beta-blockers (propranolol, nadolol, carvedilol) |
| Varices - primary/secondary prophylaxis | Beta-blockers ± endoscopic band ligation |
| Acute variceal bleeding | IV octreotide/terlipressin, urgent endoscopy (band ligation), TIPS if refractory |
| Ascites | Salt restriction, spironolactone ± furosemide; paracentesis for refractory |
| SBP | Cefotaxime/ceftriaxone; prophylaxis with norfloxacin in high-risk patients |
| Hepatic encephalopathy | Lactulose (first-line), rifaximin (second-line/maintenance); identify precipitants |
| HRS-AKI | Albumin + vasoconstrictors (terlipressin preferred; norepinephrine); treat precipitants |
| End-stage disease | Liver transplantation (only definitive treatment) |
Recent evidence note: A 2025 meta-analysis (PMID 40597728) on timing of endoscopy in acute variceal bleeding confirms early endoscopy (within 12 hours) is beneficial in cirrhotic patients - aligning with current guidelines.
Key Points to Remember
- Cirrhosis is not a specific diagnosis - it is a morphologic endpoint of many diseases with variable prognosis
- Regression is possible - fibrosis can remodel if the underlying cause is removed (e.g., cured hepatitis C, alcohol abstinence)
- The two pillars of morbidity are portal hypertension and liver insufficiency
- Compensated cirrhosis may be clinically silent for years; decompensation markedly worsens prognosis (1-year mortality ~20-57%)
- HCC surveillance (ultrasound every 6 months ± AFP) is indicated in all cirrhotic patients
Sources: Robbins & Kumar Basic Pathology, p. 597-600; Goldman-Cecil Medicine, pp. 1614-1619
This is a shared conversation. Sign in to Orris to start your own chat.