Morphological appearance of embolism
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
That last image was a placeholder icon. I have all the content I need. Here is the comprehensive answer:
Morphological Appearance of Embolism
An embolus is a detached intravascular solid, liquid, or gaseous mass carried by blood from its point of origin to a distant site, where it causes partial or complete vascular occlusion. The vast majority are dislodged thrombi (thromboembolism). Other types include fat, air/gas, amniotic fluid, cholesterol, tumor fragments, and bone marrow.
1. Pulmonary Thromboembolism
Gross morphology:
- Most (>95%) arise from DVT of the deep leg veins proximal to the popliteal fossa
- The embolus is a dark red-brown, coiled, serpentine mass conforming to the shape of the vein of origin
- It lodges in a pulmonary artery branch where the lumen narrows; a large embolus can straddle the bifurcation of the right and left pulmonary arteries - this is called a "saddle embolus"
- On cut section it appears as a coiled or elongated thrombus, distinguishable from post-mortem clot by its laminated (lines of Zahn), dry, granular, and adherent appearance
Gross image - Saddle embolus in pulmonary arteries (Robbins & Kumar):

Gross photograph showing a dark red-brown thromboembolus lodged at the pulmonary artery bifurcation. The surrounding lung parenchyma is visible.
Histological morphology:
- The embolus consists of fibrin mesh enmeshing red cells, platelet aggregates, and leukocytes
- Organized (older) emboli show ingrowth of fibroblasts and endothelial cells from the vessel wall
- Complete organization incorporates the embolus into the vascular wall; incomplete organization may leave a delicate bridging fibrous web across the vessel lumen
Downstream effects:
- 60%-80% of small emboli are clinically silent and organize
- Medium-sized emboli cause pulmonary hemorrhage (but not infarction, due to dual blood supply from bronchial arteries) - unless bronchial circulation is compromised (left heart failure)
- Small end-arteriolar emboli often produce infarction with hemorrhage
- Emboli obstructing >60% of pulmonary circulation cause cor pulmonale or sudden death
2. Systemic Thromboembolism
- 80% arise from intracardiac mural thrombi (two-thirds from left ventricular infarcts, one-fourth from dilated left atria in atrial fibrillation)
- Remainder from aortic aneurysms, ulcerated atherosclerotic plaques, or valvular vegetations
- Common sites: lower extremities (75%), brain (10%), intestines, kidneys, spleen
- Gross appearance is identical to thromboemboli elsewhere: dark red-brown, friable, and adherent to the vessel wall at the point of arrest
3. Fat Embolism
Cause: Fractures of long bones or soft tissue crush injuries rupture vascular sinusoids, releasing fat globules and marrow elements into the circulation.
Histological morphology:
- Microscopic fat globules (empty "ghost" vacuoles in paraffin sections, since lipid is dissolved by processing solvents) within pulmonary and cerebral microvasculature
- Associated hematopoietic bone marrow elements (megakaryocytes, erythroid precursors) often accompany the fat globules
- The embolus may have an early organizing thrombus attached to it
- Special stains required: Oil Red O or Sudan stains on frozen sections (fat is dissolved in routine paraffin processing) confirm fat globules
- Platelet aggregates and red cell aggregates surround fat microemboli in the microvasculature
Histological image - Bone marrow/fat embolus in pulmonary vessel:
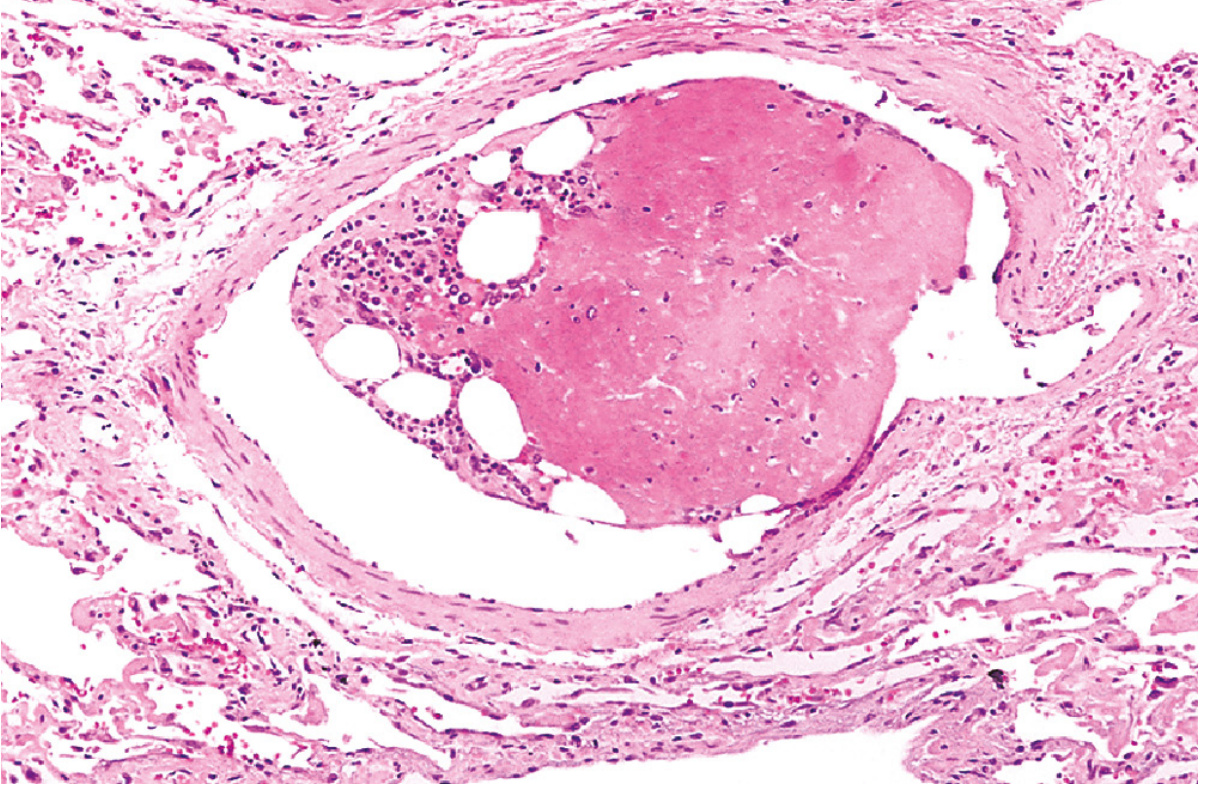
H&E section: The embolus occupies a pulmonary vessel lumen. Hematopoietic cells are visible on the left, cleared vacuoles represent dissolved marrow fat, and the relatively uniform pink area on the right is early organizing thrombus.
4. Air/Gas Embolism
Cause: Entry of air into the vasculature (neurosurgery, obstetric procedures, chest trauma, mechanical ventilation) or rapid decompression (decompression sickness/"the bends")
Morphological appearance:
- Gas bubbles coalesce to form frothy masses that obstruct vascular flow
- In pulmonary vessels: foamy appearance to blood; edema, hemorrhage, and focal atelectasis or emphysema in surrounding lung
- In decompression sickness: gas bubbles in skeletal muscles, joints, and bones cause ischemic necrosis - caisson disease results in multiple foci of avascular necrosis at the femoral heads, tibia, and humeri
- Bubbles in the CNS vasculature produce ischemic lesions
-
100 mL of air is needed for significant pulmonary effect; 300-500 mL over seconds can be fatal
5. Amniotic Fluid Embolism
Cause: Tear in placental membranes or rupture of uterine veins during labor allows amniotic fluid/fetal tissue into maternal circulation.
Classic histological findings (autopsy):
- Pulmonary microvasculature packed with squamous cells shed from fetal skin - appear as laminated, whorled eosinophilic structures
- Lanugo hair (fine fetal hair)
- Fat globules from vernix caseosa
- Mucin from fetal respiratory or gastrointestinal tract
- Associated pulmonary edema and diffuse alveolar damage
Histological image - Amniotic fluid embolism:
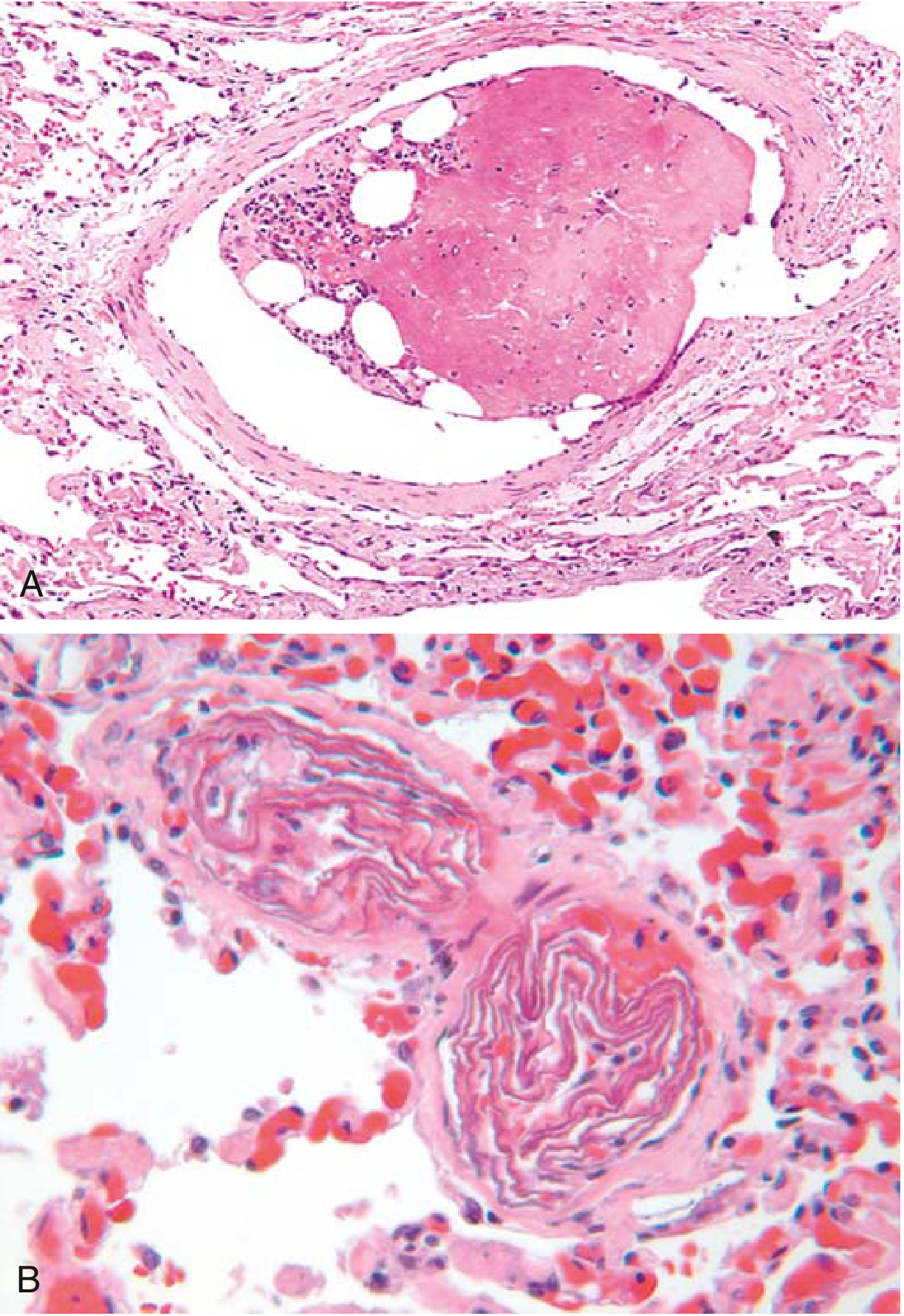
Panel A: A fat/bone marrow embolus filling a pulmonary arteriole (clear vacuoles = fat, pink cells = hematopoietic marrow elements). Panel B: Small pulmonary arterioles packed with laminated whorls of fetal squamous cells - the hallmark of amniotic fluid embolism. Surrounding lung shows edema.
Summary Table
| Type | Gross Appearance | Histological Features | Special Stains |
|---|---|---|---|
| Thromboembolism | Dark red-brown, laminated, coiled mass; saddle embolus at bifurcation | Fibrin, RBCs, platelets, leukocytes; organizing fibrosis | None specific |
| Fat embolism | Not visible grossly | Empty vacuoles (fat dissolved), marrow elements, platelet aggregates | Oil Red O / Sudan on frozen sections |
| Air embolism | Frothy blood in vessels | No specific histology; foam in vessels, lung edema/hemorrhage | None |
| Amniotic fluid embolism | Not visible grossly | Squamous cells, lanugo hair, vernix fat, mucin in pulmonary microvessels | PAS for mucin |
| Systemic thromboembolism | Same as pulmonary TE; lodges in end arteries | Same as above; infarction in supplied territory | None specific |
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease, pp. 130-132 | Robbins & Kumar Basic Pathology, pp. 93-96
This is a shared conversation. Sign in to Orris to start your own chat.