post tb sequale chest x-ray findings
Reading File
Finding Sources
Finding Sources
Searching the Web
post TB sequelae chest X-ray findings radiology
Finding Sources
Finding Sources
Reading Web Page
https://epos.myesr.org/poster/esr/ecr2019/C-3051/findings%20…
Finding Sources
Finding Sources
Finding Sources
Reading Web Page
https://pubs.rsna.org/doi/abs/10.1148/radiographics.21.4.g01…
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information from Grainger & Allison's Diagnostic Radiology and the ECR 2019 pictorial review. Here is the complete answer:
Post-TB Sequelae: Chest X-Ray Findings
Post-TB sequelae are the radiological changes that persist after bacteriological cure and treatment completion. They result from complications of both primary and post-primary (reactivation/reinfection) tuberculosis. These changes can mimic active disease and must be distinguished carefully. They are broadly categorized into parenchymal, airway, pleural/chest wall, vascular, and mediastinal changes.
1. Parenchymal Changes
Fibro-calcific Changes (most common)
- The hallmark of healed post-primary TB
- Irregular, dense opacities with or without calcification, typically in the upper lobes (apical and posterior segments)
- Combined fibrosis and calcification = "fibro-calcific change"
- Associated volume loss of the affected lobe with compensatory hyperinflation of adjacent lung
Ghon Focus / Ranke Complex
- A Ghon focus = residual well-defined rounded or irregular opacity (with or without calcification) from healed primary TB
- Heterogeneous, irregular nodal calcification in the ipsilateral hilum or mediastinum
- Ghon focus + ipsilateral calcified lymph node = Ranke complex
- Calcification of the Ghon focus occurs in ~15% of cases
Tuberculoma
- Rounded soft-tissue density, usually 1-4 cm, often with central or irregular calcification (in 20-30%)
- Smooth, well-defined margins; frequently stable for years
- Satellite nodules present in up to 80% of cases
- May be solitary or multiple
Thin-Walled (Residual) Cavity
- After cavitary TB resolves, a thin-walled, air-filled cavity may persist without active disease
- Wall thickness < 2 mm; no surrounding consolidation
- Clinically significant as a site for aspergilloma formation
Aspergilloma (Mycetoma)
- A fungus ball (Aspergillus) colonising an existing TB cavity or bronchiectatic space
- CXR: rounded opacity within a cavity, often with an "air crescent sign" (air cap between the ball and cavity wall)
- Changes position with posture (pathognomonic when present)
Cicatrization Collapse (Destroyed Lung)
- The most severe parenchymal sequela
- Complete or near-complete destruction of a lobe or entire lung from prolonged cavitation, endobronchial spread, and fibrosis
- CXR shows: dense opacification, marked volume loss, ipsilateral mediastinal and tracheal shift, crowded ribs, and compensatory emphysema on the opposite side
- More often unilateral
2. Airway Disease
Bronchiectasis
- Common and characteristic sequela; occurs by destruction and fibrosis of parenchyma with irreversible secondary bronchial dilatation (traction bronchiectasis)
- Location in the apical and posterior segments of the upper lobes is highly suggestive of tuberculous origin
- CXR: tram-track opacities, ring shadows, crowded vascular markings; better seen on CT
Tracheobronchial Stenosis
- Results from healed endobronchial TB or extrinsic compression by calcified lymph nodes
- CXR may show lobar atelectasis or air-trapping; can be subtle on plain film, better assessed on CT
3. Pleural / Chest Wall Changes
Pleural Thickening
- Common residual finding; may be unilateral or bilateral
- Ranges from mild apical capping to extensive fibrous pleural rind (fibrothorax)
- CXR: blunted costophrenic angle, dense band along the chest wall
Pleural Calcification
- Dense, often irregular calcification along the visceral and/or parietal pleura
- Often associated with old tuberculous empyema
- "Eggshell" pattern or broad sheet of calcification is characteristic
Fibrothorax
- Extensive pleural fibrosis encasing the entire lung
- CXR: marked volume loss, scoliosis, and ipsilateral mediastinal shift; ipsilateral ribs are crowded
Empyema Necessitatis
- Rare: direct spread of infection through chest wall to soft tissues
- CXR: soft-tissue mass at chest wall, often with rib involvement
4. Vascular Changes
Rasmussen Aneurysm
- Pseudoaneurysm of a pulmonary artery branch that traverses or is adjacent to a tuberculous cavity
- CXR: a nodular opacity within or adjacent to a cavity (the aneurysm itself)
- Can rupture and cause massive haemoptysis
- Best characterised on contrast-enhanced CT
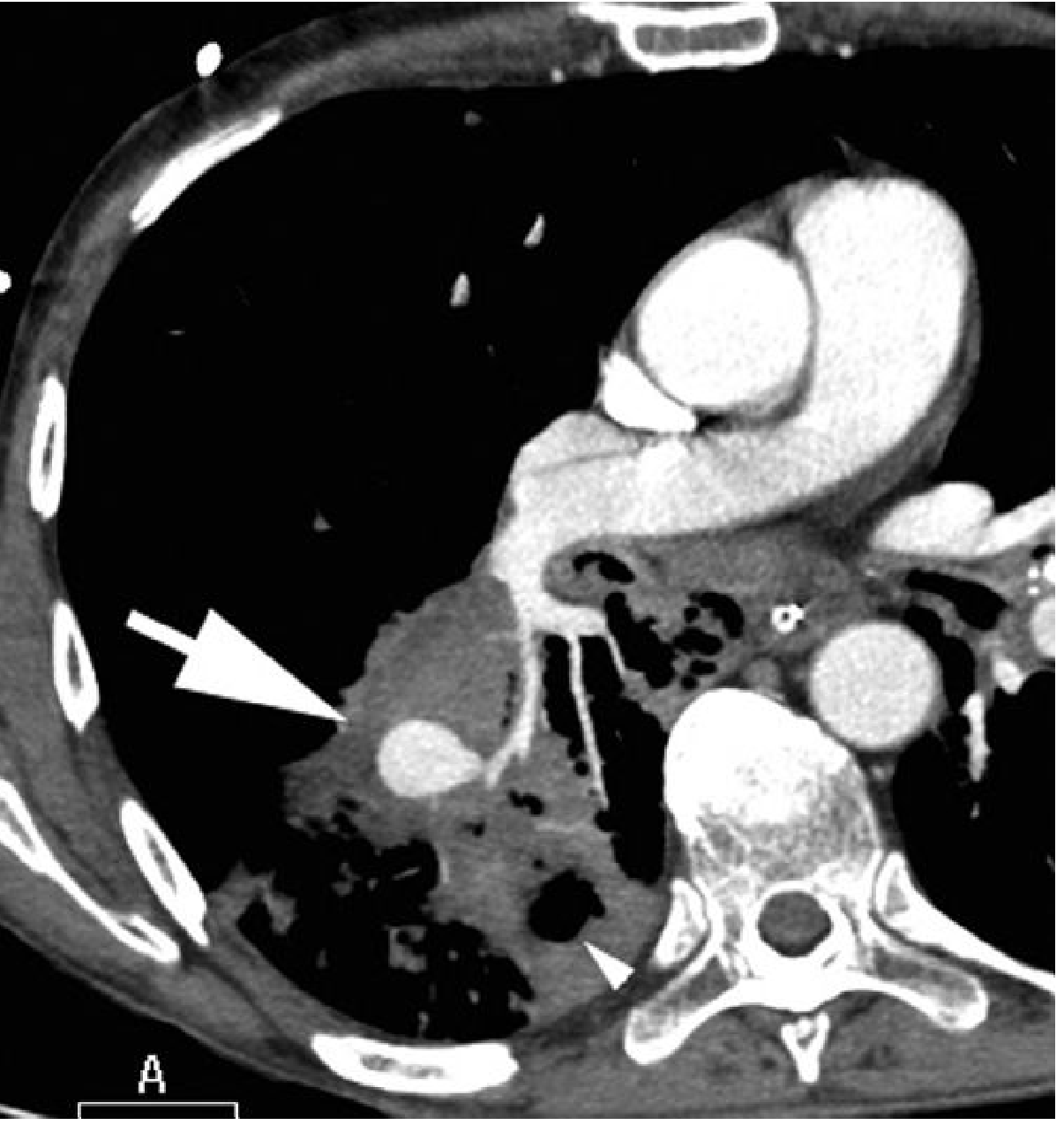
Fig: Rasmussen Aneurysm in a 65-year-old man with chronic destructive pulmonary TB. Contrast-enhanced CT shows a contrast-filling aneurysm (arrow) within parenchymal consolidation in the superior segment of the right lower lobe. Note the associated parenchymal cavity (arrowhead). - Grainger & Allison's Diagnostic Radiology
5. Mediastinal / Lymph Node Changes
Calcified Mediastinal/Hilar Lymph Nodes
- Heterogeneous, irregular, often stippled calcification in hilar and mediastinal nodes
- Usually asymptomatic residual finding
- Rarely can compress adjacent bronchi causing atelectasis or broncholithiasis
Summary Table
| Category | CXR Finding | Key Features |
|---|---|---|
| Parenchymal | Fibro-calcific scarring | Upper lobes, apical, volume loss |
| Parenchymal | Ghon focus / Ranke complex | Calcified peripheral nodule + ipsilateral hilar nodes |
| Parenchymal | Tuberculoma | Round soft-tissue density, calcified, satellite nodules |
| Parenchymal | Thin-walled residual cavity | Air-filled, no surrounding consolidation |
| Parenchymal | Aspergilloma | Fungus ball + air crescent in cavity |
| Parenchymal | Cicatrization/destroyed lung | Dense opacification + ipsilateral mediastinal shift |
| Airway | Bronchiectasis | Upper lobe, traction type; tram-tracks |
| Airway | Bronchostenosis | Lobar atelectasis |
| Pleural | Pleural thickening | Blunted costophrenic angle, apical capping |
| Pleural | Pleural calcification | Dense irregular, sheet-like calcification |
| Pleural | Fibrothorax | Encased lung, mediastinal shift |
| Vascular | Rasmussen aneurysm | Nodular opacity in/adjacent to cavity |
| Mediastinal | Calcified lymph nodes | Hilar/mediastinal, irregular calcification |
Clinical Pearls
- Upper lobe location of fibrosis, cavitation, bronchiectasis, or calcification is the strongest indicator of a tuberculous aetiology
- Residual thin-walled cavities and bronchiectatic spaces are the most common sites for superimposed aspergilloma
- Cicatrization collapse can make it difficult to assess for residual active disease radiologically - CT and bronchoscopy are required
- Mediastinal tracheal shift toward the side of volume loss is an important sign of post-primary sequelae and should not be confused with a mediastinal mass
- Some findings (mild pleural fibrosis, calcified nodes) are incidental and asymptomatic; others like fibrothorax and destroyed lung cause significant respiratory compromise
Sources: Grainger & Allison's Diagnostic Radiology; ECR 2019 Pictorial Review (Kim HY et al., Radiographics 2001, post-TB sequelae)
This is a shared conversation. Sign in to Orris to start your own chat.