Infective endocarditis diagnosis criteria and treatment approach
Reading File
Finding Sources
Searching PubMed
"infective endocarditis"[MeSH Terms] AND "diagnosis" AND "treatment"
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it:
Infective Endocarditis (IE): Diagnosis and Treatment
Overview
IE is an infection of the endocardial surface of the heart, most commonly affecting cardiac valves. It requires a multidisciplinary "endocarditis team" approach (infectious diseases, cardiology, cardiac surgery) and inpatient management at a center with appropriate expertise, which has been shown to improve outcomes.
Diagnosis: The 2023 Duke Criteria
The original Duke criteria (1994) were modified to improve performance in S. aureus bacteremia and culture-negative IE. In 2023, they were further updated to incorporate newer imaging modalities including PET/CT.
Classification
| Category | Criteria Required |
|---|---|
| Definite IE | 2 major criteria, OR 1 major + 3 minor, OR 5 minor criteria |
| Possible IE | 1 major + 1 minor, OR 3 minor criteria |
| Rejected | Firm alternative diagnosis; resolution with antibiotics <4 days; no pathologic evidence at surgery with antibiotics ≤4 days |
Major Criteria
A. Microbiologic (positive blood cultures)
- Typical organisms (Viridans streptococci, S. bovis, HACEK group, S. aureus, community-acquired enterococci) isolated from 2+ separate blood culture sets
- Less typical organisms isolated from 3+ separate culture sets
- At least 2 positive cultures drawn >12 hours apart, OR all of 3 or majority of >4 cultures (first and last drawn ≥1 hour apart)
- Single positive blood culture for Coxiella burnetii OR antiphase IgG antibody titer >1:800
B. Positive laboratory test
- Positive PCR/nucleic acid test from blood for Coxiella burnetii, Bartonella spp., or Tropheryma whipplei
C. Imaging criteria (any one of)
- Echocardiography/cardiac CT: vegetation, valvular perforation/aneurysm, abscess, pseudoaneurysm, intracardiac fistula, significant new valvular regurgitation (compared to prior imaging), new partial prosthetic valve dehiscence
- 18F-FDG PET/CT: abnormal metabolic activity (at least 3 months after implantation) involving native/prosthetic valve, ascending aortic graft, intracardiac device leads, or other prosthetic material
D. Surgical criteria
- Evidence of IE observed by direct inspection during cardiac surgery (in absence of major microbiologic or imaging criteria)
Minor Criteria
| Category | Features |
|---|---|
| Predisposition | Previous IE, prosthetic valve, prior valve repair, congenital heart disease, >mild regurgitation/stenosis, endovascular CIED, HOCM, injection drug use |
| Fever | Temperature >38.0°C (100.4°F) |
| Vascular phenomena | Arterial emboli, septic pulmonary infarcts, cerebral/splenic abscess, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, Janeway lesions |
| Immunologic phenomena | Osler's nodes, Roth's spots, positive rheumatoid factor, immune complex glomerulonephritis |
| Microbiologic | Positive blood cultures not meeting major criteria; or positive PCR/NAT for an organism consistent with IE from a sterile body site other than cardiac tissue |
| Imaging (minor) | Abnormal FDG-PET/CT within 3 months of prosthetic valve/device implantation |
| Physical exam | New valvular regurgitation on auscultation (if echocardiography unavailable) |
Echocardiographic Workup
The diagnostic flowchart below (from Goldman-Cecil Medicine) guides echocardiographic decision-making:
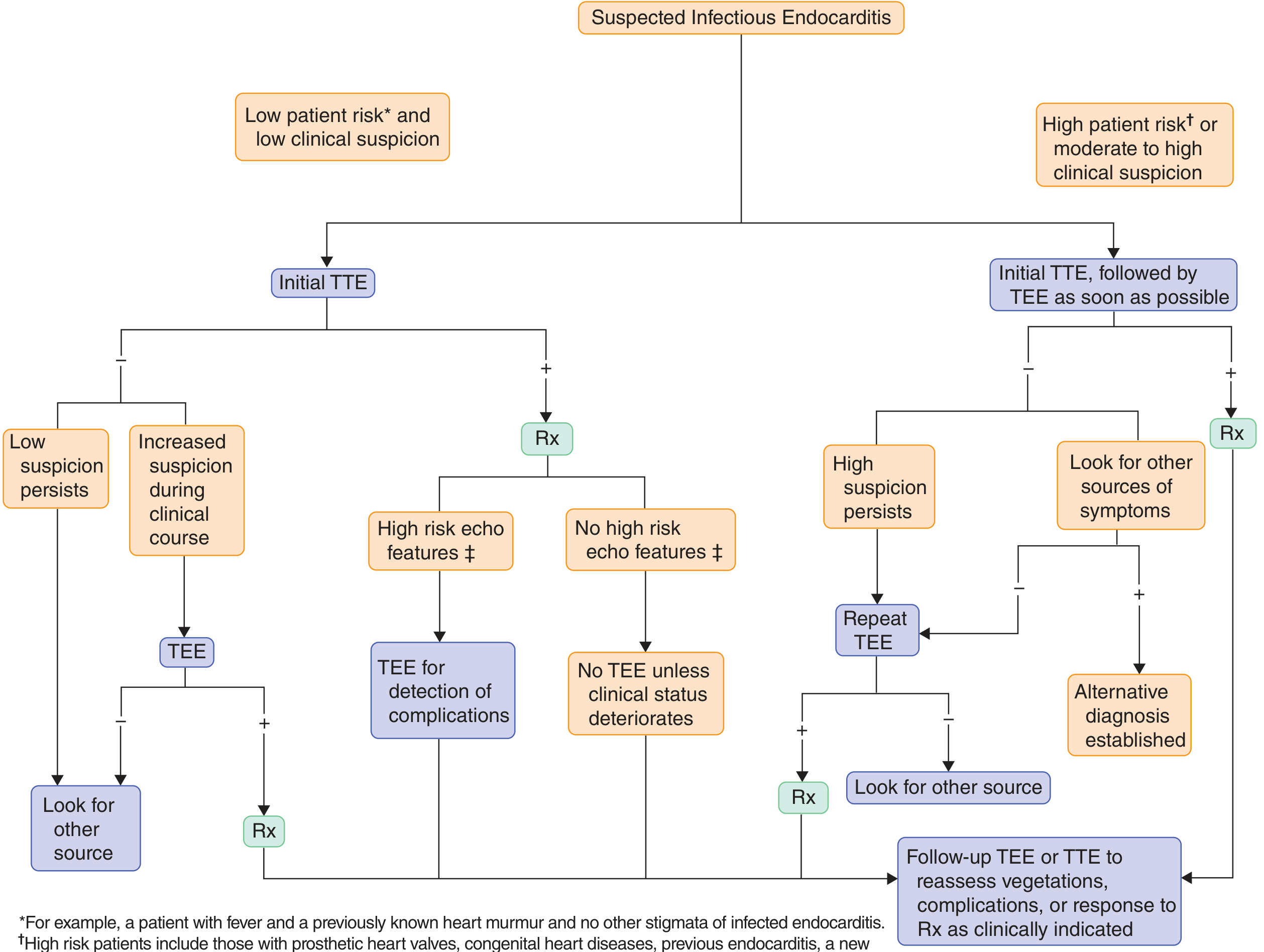
Key principles:
- TTE first in all patients; proceed to TEE when TTE is non-diagnostic or of poor quality
- TEE as first-line for prosthetic valve IE (sensitivity much higher than TTE)
- TEE immediately (Class I) when: TTE non-diagnostic with high suspicion, prosthetic valve involved, suspected complications (abscess, perforation, fistula), pre-operative planning, intraoperative guidance
- Repeat imaging is indicated with clinical deterioration, new murmur, persistent fever/bacteremia, or virulent organisms (e.g., S. aureus)
- High-risk echo features warranting closer follow-up: large/mobile vegetations, valvular insufficiency, perivalvular extension, secondary ventricular dysfunction
Treatment
Team-Based Approach
All patients should be managed inpatient at a center with an experienced IE team. An infectious diseases specialist is essential to guide empiric and definitive antibiotic therapy, and cardiac surgery must be available for emergent intervention.
Empiric Antibiotic Therapy
Begin empirics in acutely ill patients, those with complications, or high-risk patients (prosthetic valves). Stable patients with subacute presentation may be observed briefly to obtain blood cultures before starting antibiotics.
| Clinical Scenario | Empiric Regimen |
|---|---|
| Native valve, no MRSA concern | Nafcillin (or oxacillin) + penicillin + gentamicin |
| Native valve, MRSA possible (IDU, healthcare exposure) | Vancomycin + ceftriaxone + gentamicin |
| Prosthetic valve IE | Vancomycin + gentamicin + rifampin |
Definitive Antibiotic Therapy (by Organism)
Therapy is guided by susceptibility testing. Duration is typically 4-6 weeks for most cases.
Viridans streptococci / S. bovis (fully susceptible, MIC ≤0.12 mcg/mL):
- Penicillin G or ceftriaxone (4 weeks) - outpatient once-daily ceftriaxone is acceptable after initial hospital observation
Staphylococcus aureus:
- MSSA: Nafcillin or oxacillin (6 weeks); cefazolin is an alternative in beta-lactam intolerant patients
- MRSA: Vancomycin (6 weeks); note vancomycin has inferior microbiologic outcomes compared to nafcillin for MSSA
- Daptomycin is an option (particularly for right-sided IE)
Enterococci (fully susceptible):
- Penicillin/ampicillin + gentamicin (4-6 weeks) - gentamicin is critical for synergy in enterococcal IE
- Ampicillin + high-dose ceftriaxone (2g IV q12h) is an alternative to avoid aminoglycoside toxicity in E. faecalis
- VRE: daptomycin, linezolid, or quinupristin-dalfopristin (high relapse rates; surgery often needed)
HACEK organisms:
- Ceftriaxone or ampicillin-sulbactam (4 weeks)
- Often curable with antibiotics alone without surgery
Culture-negative / Coxiella burnetii (Q fever endocarditis):
- Doxycycline + hydroxychloroquine for ≥18 months (native valve); minimum until PCR becomes negative in blood
Note on gentamicin: Routine addition of gentamicin for synergy is no longer recommended in most regimens due to nephrotoxicity risk (3-fold increase in creatinine clearance reduction). It remains essential only in enterococcal IE.
Surgical Indications
Native Valve IE
Class I (Surgery indicated):
- Heart failure caused by valve dysfunction (severe regurgitation or obstruction)
- IE caused by fungi or highly resistant organisms
- Heart block, annular or aortic abscess, or destructive penetrating lesions
Class IIa (Surgery reasonable):
- Persistent bacteremia >5-7 days despite appropriate antibiotics
- Recurrent emboli and persistent/enlarging vegetations despite appropriate therapy
- Severe valve regurgitation + mobile vegetations >10 mm
Class IIb (Surgery may be considered):
- Mobile vegetations >10 mm (especially anterior mitral leaflet) with other relative indications
Prosthetic Valve IE (PVE)
Class I:
- Symptomatic heart failure from valve dehiscence, intracardiac fistula, or severe prosthetic dysfunction
- Persistent bacteremia >5-7 days despite appropriate therapy
- Heart block, annular/aortic abscess, or destructive lesions
- Fungi or highly resistant organisms
Class IIa:
- Recurrent emboli despite appropriate antibiotics
- Relapsing PVE
Right-Sided IE
- Surgery generally avoided if possible (especially in IV drug users)
- Indications include heart failure, recurrent emboli, resistant organisms, very large vegetations (≥20 mm), or persistent bacteremia
- Valve repair preferred over replacement when feasible
Timing of Surgery with Neurologic Complications
- No delay needed for: silent microembolism, TIA, cerebral abscess, ischemic stroke without hemorrhagic conversion and without severe neurological deficits
- Delay at least 4 weeks for: major ischemic stroke or intracranial hemorrhage
Antibiotic Prophylaxis (Prevention)
Per the 2021 AHA update, prophylaxis is recommended before invasive dental procedures only for high-risk patients:
- Prosthetic cardiac valve or valve repair with prosthetic material
- Previous IE
- Left ventricular assist devices or implantable hearts
- Certain congenital heart diseases (unrepaired cyanotic CHD, repaired CHD with residual defects)
- Cardiac transplant with valvulopathy
Preferred agent: Amoxicillin 2g PO 30-60 minutes before procedure. Allergy screening (90% of "penicillin allergic" patients have negative skin testing) is encouraged so amoxicillin can be used broadly. Clindamycin is no longer recommended as an alternative (risk of C. difficile). Doxycycline is now listed as an alternative in truly penicillin-allergic patients.
Key References:
- Textbook of Clinical Echocardiography (2023 Duke Criteria table)
- Fuster & Hurst's The Heart, 15th Ed. (modified Duke criteria, surgical indications)
- Goldman-Cecil Medicine (treatment algorithms, empiric/definitive regimens)
- Braunwald's Heart Disease (AHA 2021 prophylaxis update, echocardiographic approach)
Classification of causes for puo and relevant questions
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have everything needed for a comprehensive, well-structured response.
Pyrexia of Unknown Origin (PUO / FUO)
Definition
FUO was originally defined by Petersdorf and Beeson (1961) as fever ≥38.3°C (101°F) on at least two occasions, illness duration ≥3 weeks, and no established diagnosis despite 1 week of inpatient evaluation. The modern definition (used in current literature) is:
- Fever ≥38.3°C (101°F) on at least two occasions
- Illness duration of at least 3 weeks
- No known immunocompromised state (immunocompromised patients form a separate category requiring a more aggressive approach)
- No diagnosis despite appropriate evaluation
Note: immunocompromised, nosocomial, and HIV-associated fevers each constitute separate FUO subtypes with different approaches.
The "FUO Paradox"
Paradoxically, the proportion of patients remaining undiagnosed has increased over time despite advances in imaging, because easier-to-diagnose cases now resolve before 3 weeks - leaving only the hardest cases to fulfill FUO criteria. In Western Europe today, up to 50% of FUO cases remain undiagnosed.
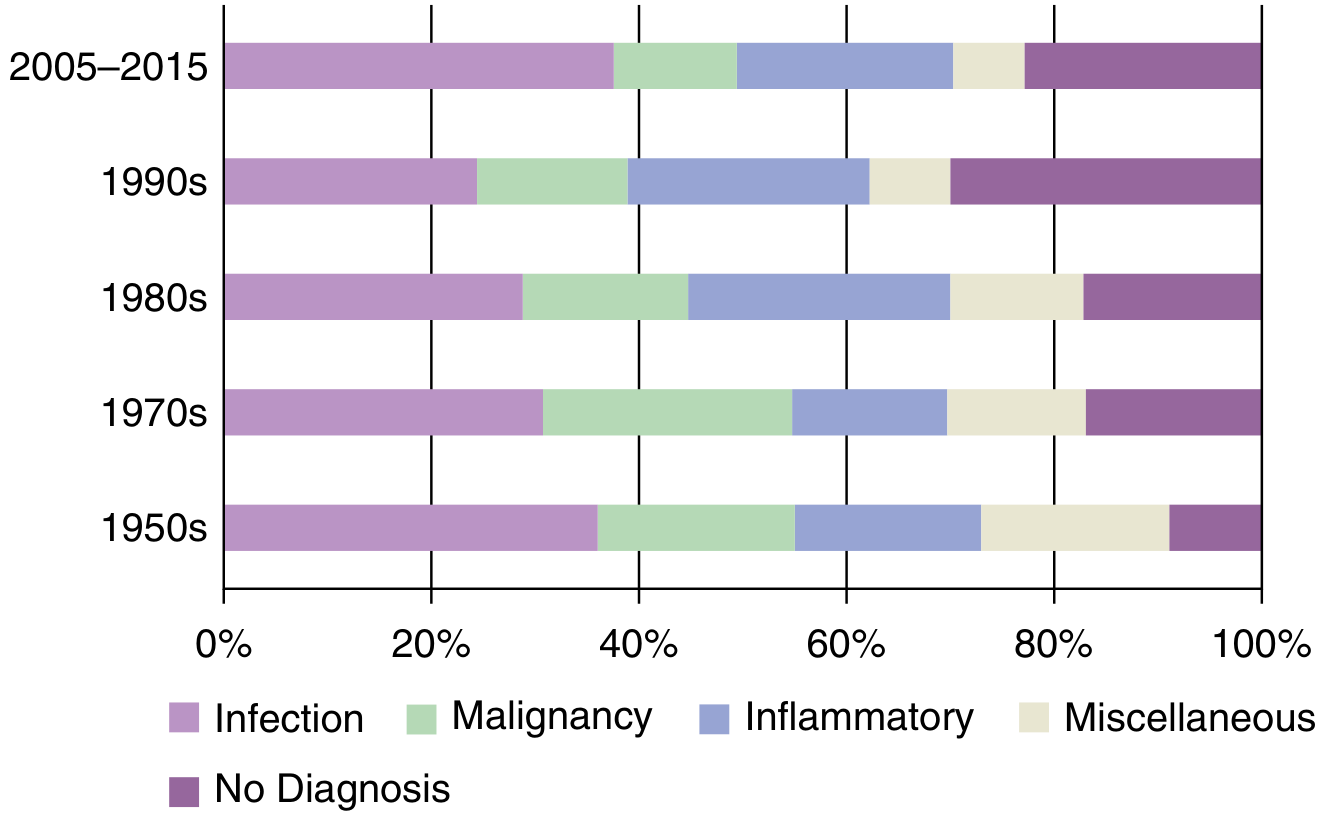
Classification of Causes
FUO is grouped into five domains. The relative prevalence of each varies significantly by geography (infections dominate in Asia and the Middle East; non-infectious inflammatory diseases dominate in Western Europe).
1. Infections (~15-66% by region)
Bacterial - non-specific (occult foci):
- Abdominal/pelvic abscess, epidural abscess, intracranial abscess, muscle abscess, renal abscess
- Endocarditis (culture-negative), osteomyelitis, spondylodiscitis
- Sinusitis, cholangitis, cholecystitis, diverticulitis, prostatitis, pyelonephritis
- Septic arthritis, infected vascular/joint prosthesis, infected vascular catheter
- Mycotic aneurysm
Bacterial - specific organisms:
- Mycobacterium tuberculosis (most common single infectious cause globally; responsible for up to 50% of infections in non-Western cohorts)
- Brucellosis, bartonellosis, leptospirosis, typhoid fever, listeriosis
- Q fever (Coxiella burnetii), rickettsiosis, ehrlichiosis
- Whipple disease (Tropheryma whipplei)
- Actinomycosis, nocardiosis, nontuberculous mycobacteria
- Lyme disease, relapsing fever (Borrelia spp.)
- Legionellosis, melioidosis, tularemia, psittacosis
- Syphilis, gonococcus, chronic meningococcemia
Viral:
- Epstein-Barr virus (EBV), Cytomegalovirus (CMV)
- Acute HIV infection
- Hepatitis A, B, or E
- COVID-19 (post-acute sequelae)
- Dengue, West Nile virus, enteroviruses, hantavirus, Lassa fever
Parasitic/Fungal:
- Malaria, visceral leishmaniasis (kala-azar), toxoplasmosis
- Babesiosis, filariasis, trichinosis
- Aspergillosis, candidiasis, histoplasmosis, coccidioidomycosis, Pneumocystis
2. Non-Infectious Inflammatory Diseases (NIIDs) - ~15-25%
The largest single category in Western cohorts. Includes autoimmune, autoinflammatory, granulomatous diseases, and vasculitides.
Most common:
- Adult-onset Still disease (AOSD)
- Giant cell arteritis / temporal arteritis
- Polymyalgia rheumatica
- Systemic lupus erythematosus (SLE)
- Inflammatory bowel disease (Crohn's disease more than UC)
- Sarcoidosis
Other:
- Rheumatoid arthritis (with systemic features)
- Polyarteritis nodosa, granulomatosis with polyangiitis (GPA), Takayasu arteritis
- Antiphospholipid syndrome
- Sjögren's syndrome, mixed connective tissue disease
- Autoinflammatory syndromes: Familial Mediterranean fever (FMF), TRAPS, CAPS, PFAPA
- Hemophagocytic lymphohistiocytosis (HLH)
- Castleman disease
- Kikuchi-Fujimoto disease (necrotizing lymphadenitis)
- Behçet's disease
- Kawasaki disease
3. Malignancy (~7-14%)
The proportion has decreased over time due to earlier detection with CT/PET.
Hematologic (most common):
- Hodgkin lymphoma
- Non-Hodgkin lymphoma
- Leukemia (especially AML, CLL)
- Multiple myeloma, myelodysplastic syndrome
- Intravascular lymphoma (often undetected until autopsy)
Solid tumors:
- Renal cell carcinoma (classic fever-flank pain-hematuria triad, but often presents with fever alone)
- Hepatocellular carcinoma
- Colon and gastric adenocarcinoma
- Melanoma, mesothelioma
- Atrial myxoma (cardiac tumour mimicking IE or embolic disease)
4. Miscellaneous (~5-8%)
- Drug fever - virtually any drug can cause fever, even after long-term use; common culprits: allopurinol, carbamazepine, phenytoin, sulfonamides, minocycline, vancomycin, beta-lactams, isoniazid, furosemide. Often accompanied by eosinophilia ± lymphadenopathy (DRESS/DIHS)
- Factitious fever - patient manipulates thermometer (fraudulent); dissociation between pulse rate and temperature is a clue; confirm by simultaneous multi-site temperature measurement
- Self-induced fever - injection of contaminated material; more common in those with healthcare access
- Hematoma (especially retroperitoneal)
- Pulmonary embolism / chronic thromboembolic disease
- Drug-induced hyperthermia (neuroleptic malignant syndrome, serotonin syndrome, malignant hyperthermia)
- Subacute thyroiditis
- Hyperthyroidism / hypoadrenalism (Addison disease) - endocrine causes
- Pheochromocytoma
- Periodic fever syndromes
- Central causes: hypothalamic dysfunction, CVA, encephalitis, brain tumor
- Peripheral dysregulation: anhidrotic ectodermal dysplasia, exercise-induced hyperthermia, heat stroke
5. No Diagnosis (~16-50%)
The proportion with no final diagnosis is much higher in Western Europe (up to >50%) than in Asia or the Middle East (~8-17%). The prognosis in undiagnosed FUO is generally favorable - the large majority become symptom-free spontaneously. However, periodic re-evaluation is necessary.
Relevant History Questions
The most important step in diagnosis is identifying potentially diagnostic clues (PDCs) - all localizing signs, symptoms, and abnormalities pointing toward a diagnosis. History-taking should be exhaustive and repeated at follow-up visits.
Fever Characteristics
- Pattern: continuous/sustained (typhoid, brucellosis), intermittent (malaria - tertian/quartan pattern), relapsing (Borrelia, lymphoma, FMF), hectic/spiking (abscess, lymphoma, Still disease)
- Duration: how long has fever been present? Any episodes before?
- Height and timing: morning vs. evening predominance
- Associated symptoms: rigors (bacteremia, malaria), night sweats (TB, lymphoma, HIV)
- Response to antipyretics
Travel and Geographic Exposure
- Recent AND remote travel history (malaria, typhoid, brucellosis, visceral leishmaniasis, melioidosis, histoplasmosis, coccidioidomycosis vary by region)
- Country of origin (TB endemic areas, FMF in Mediterranean/Middle East populations)
- Rural vs. urban exposure
- Water sources (leptospirosis, tularemia)
Animal and Environmental Contacts
- Farm animals / cattle / goats (Q fever, brucellosis)
- Cats (bartonellosis/cat scratch, Q fever)
- Dogs (leptospirosis, brucellosis)
- Ticks (Lyme, rickettsiosis, ehrlichiosis, tick-borne relapsing fever, tularemia)
- Birds/poultry (psittacosis, histoplasmosis)
- Rodents (leptospirosis, hantavirus)
- Unpasteurized dairy (brucellosis, TB, listeriosis)
- Soil/construction/caves (histoplasmosis, coccidioidomycosis, melioidosis)
Past Medical and Surgical History
- Previous cardiac valve disease, prosthetic valves (endocarditis, infected prosthesis)
- Previous surgery (intra-abdominal abscess, spondylodiscitis)
- Previous TB or TB contacts
- Malignancy history (recurrence, post-treatment lymphoma)
- Autoimmune disease history
- Recurrent infections (immunodeficiency)
Drug History (Critical)
- All current and recently stopped medications (drug fever can occur after months of use)
- Over-the-counter drugs, herbal/traditional remedies, supplements
- Recent antibiotic or corticosteroid use (can mask diagnosis and render cultures sterile)
- Vaccinations (BCG infection)
Sexual and Social History
- HIV risk factors (unprotected sex, intravenous drug use, transfusions)
- Injection drug use (endocarditis, septic emboli, HIV, hepatitis)
- Occupation (healthcare workers - TB; veterinarians/abattoir workers - Q fever, brucellosis)
- Alcohol use (hepatic abscess, TB predisposition)
Family History
- Familial Mediterranean fever (FMF) or other periodic fever syndromes
- Hereditary malignancies
- Autoimmune diseases
Systemic Review - Key Symptoms to Ask
- Weight loss (TB, lymphoma, malignancy, HIV, inflammatory disease)
- Night sweats (TB, lymphoma, HIV, brucellosis)
- Lymphadenopathy (lymphoma, EBV, CMV, HIV, TB, toxoplasmosis, cat scratch, sarcoidosis, Still disease)
- Rash (Still disease - classic evanescent salmon-colored rash during fever spikes; SLE malar rash; drug rash; rickettsia; viral exanthem; vasculitis)
- Joint pains (Still disease, SLE, reactive arthritis, brucellosis, Lyme, IBD)
- Headache/neck stiffness (CNS infection, vasculitis)
- Visual symptoms (giant cell arteritis - jaw claudication, scalp tenderness, visual loss)
- Abdominal pain (abscess, IBD, FMF attacks)
- Urinary symptoms (occult UTI, pyelonephritis, renal abscess, renal cell carcinoma)
- Cardiac symptoms - new murmur, palpitations (endocarditis, atrial myxoma)
- Respiratory symptoms (TB, fungal, sarcoidosis, lymphoma mediastinal adenopathy)
Structured Diagnostic Approach
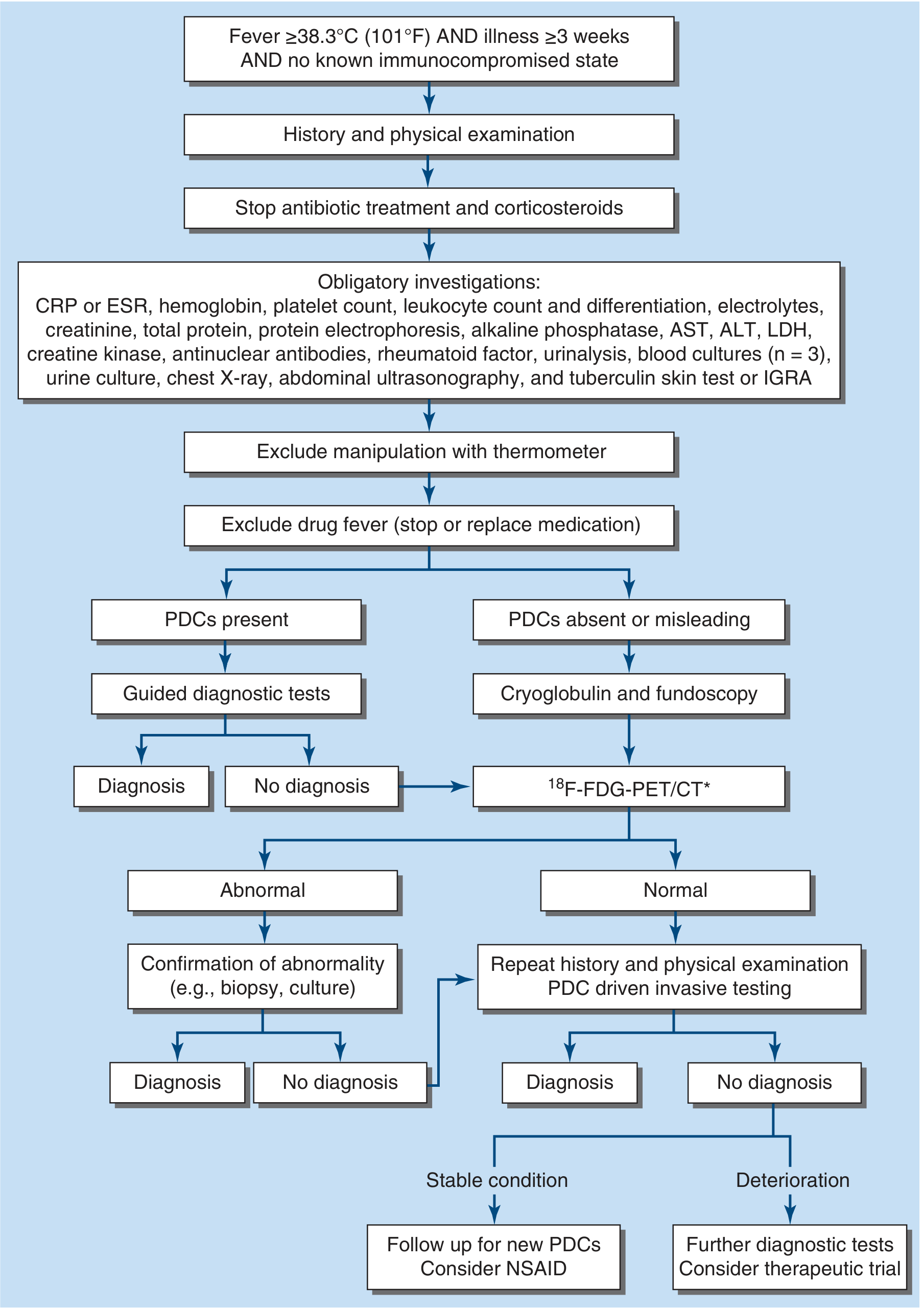
Key principle: Before further testing, stop antibiotics and corticosteroids (they mask cultures, reduce lymph node size, and suppress fever regardless of cause). Then:
- Identify all PDCs (potentially diagnostic clues) from history + exam + obligatory tests
- If PDCs present → targeted, diagnosis-directed investigations
- If PDCs absent → 18F-FDG-PET/CT (detects a cause in 30-60% of cases; identifies metabolically active foci for biopsy, and can itself be diagnostic for large-vessel vasculitis)
- If still no diagnosis → tissue biopsy (lymph node, liver, bone marrow, temporal artery) guided by PET/CT
- Undiagnosed + stable → watchful waiting, periodic re-evaluation, consider NSAIDs
- Undiagnosed + deteriorating → empirical therapeutic trial (antibiotics if infection suspected, antituberculars if TB likely, NSAIDs/colchicine/IL-1 inhibitors if inflammatory disease probable)
Empirical glucocorticoids should be avoided unless infection and lymphoma have been adequately excluded - they can mask fever while permitting spread of both.
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Chapter 22 - Fever of Unknown Origin
- Goldman-Cecil Medicine, Chapter 259 - Approach to Fever / FUO
What will be the discharge plan for infective endocarditis patient
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.