Anti epileptic drugs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Excellent — I have all the key content. Here is a comprehensive overview of antiepileptic drugs (AEDs).
Antiepileptic Drugs (AEDs)
Overview
The goal of AED therapy is a seizure-free state with minimal side effects. Approximately 70% of patients with epilepsy are fully or nearly fully controlled with medications; an additional 20–25% have significant reduction in seizure frequency. About half of patients respond to the first agent tried; a second monotherapy agent brings the total to ~65%. Those failing two adequate trials are considered drug-resistant epilepsy.
— Adams and Victor's Principles of Neurology, 12th Ed.
Mechanisms of Action
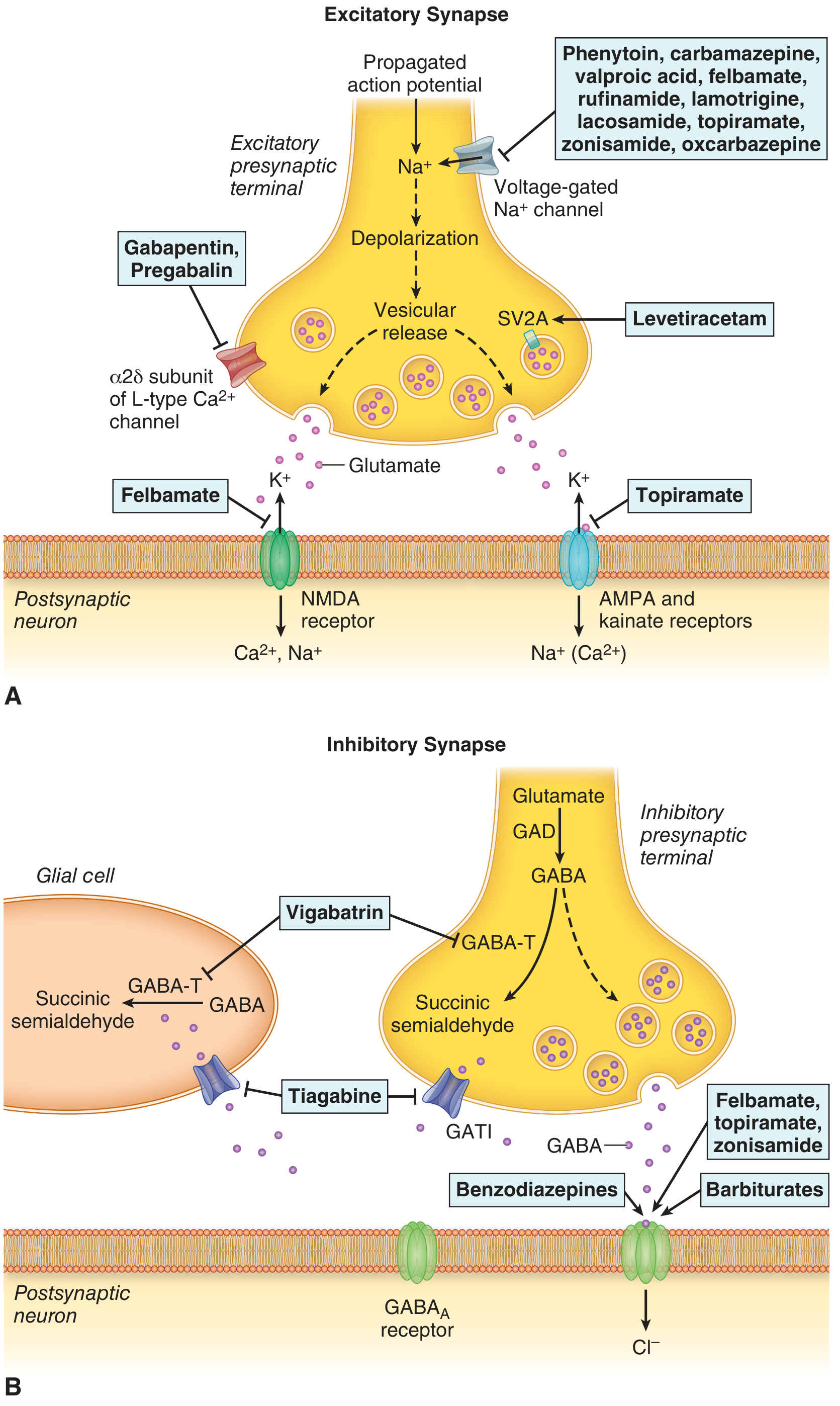
AEDs act via four main mechanisms:
| Mechanism | Drugs |
|---|---|
| Voltage-gated Na⁺ channel blockade (stabilize inactivated state, reduce repetitive firing) | Phenytoin, carbamazepine, oxcarbazepine, eslicarbazepine, lamotrigine, lacosamide, zonisamide, topiramate, valproate |
| GABA potentiation (enhance Cl⁻ influx via GABA-A, or increase GABA synthesis/availability) | Benzodiazepines (GABA-A receptor modulation), barbiturates, valproate, tiagabine (blocks GABA reuptake), vigabatrin (inhibits GABA-T), topiramate, gabapentin/pregabalin |
| Ca²⁺ channel blockade (T-type channels → absence seizures; α2δ subunit of L-type channels) | Ethosuximide, valproate (T-type); gabapentin, pregabalin (α2δ subunit of L-type) |
| Synaptic vesicle protein SV2A modulation (reduces vesicular neurotransmitter release) | Levetiracetam, brivaracetam |
| Glutamate receptor antagonism (AMPA/kainate or NMDA blockade) | Topiramate, perampanel (AMPA), felbamate (NMDA) |
Classification and Key Drugs
First-Generation AEDs
| Drug | Mechanism | Indications | Key Side Effects |
|---|---|---|---|
| Phenytoin | Na⁺ channel blocker | Focal & generalized seizures, status epilepticus | Nonlinear (zero-order) kinetics, gingival hypertrophy, hirsutism, nystagmus, coarsening of facial features, teratogenic; induces CYP450 |
| Carbamazepine | Na⁺ channel blocker | Focal & generalized seizures | Leukopenia, hyponatremia (SIADH), autoinduction, Stevens-Johnson syndrome (HLA-B*1502 in Asians), hepatic enzyme inducer |
| Phenobarbital | GABA-A potentiation, Na⁺ channel blockade | Focal & generalized, infantile seizures | Drowsiness, mental dullness, behavioral problems in children; strong CYP450 inducer; Dupuytren's contracture with long-term use |
| Ethosuximide | T-type Ca²⁺ channel blocker | Absence seizures only | GI upset, hiccups; does NOT worsen other seizure types |
| Valproate (Valproic acid) | Multiple (GABA ↑, Na⁺ channel, T-Ca²⁺, NMDA) | Focal & generalized, absence, myoclonic | Hepatotoxicity (esp. <2 yrs), weight gain, teratogenic (neural tube defects), tremor, polycystic ovarian syndrome; CYP inhibitor |
| Primidone | Metabolized to phenobarbital | Focal & generalized | Same as phenobarbital |
Second-Generation AEDs
| Drug | Mechanism | Indications | Key Side Effects |
|---|---|---|---|
| Lamotrigine | Na⁺ channel blocker | Focal & generalized (broad spectrum) | Stevens-Johnson syndrome (esp. with rapid titration), rash; slow titration required when combined with valproate |
| Topiramate | Multiple (Na⁺, AMPA, GABA ↑, Ca²⁺) | Focal & generalized | Cognitive impairment ("dopamax"), nephrolithiasis, weight loss, metabolic acidosis, angle-closure glaucoma |
| Gabapentin | α2δ subunit Ca²⁺ channel blocker | Focal seizures (adjunctive) | Sedation, weight gain; also used for neuropathic pain |
| Oxcarbazepine | Na⁺ channel blocker | Focal seizures | Hyponatremia (3%), fewer hematologic effects than carbamazepine; cross-hypersensitivity rash with carbamazepine |
| Levetiracetam | SV2A modulation | Focal & generalized (broad spectrum) | Irritability, mood disturbance, psychosis; no drug interactions (not hepatically metabolized) |
| Tiagabine | GABA reuptake inhibitor (blocks GATI) | Focal seizures (adjunctive) | May worsen generalized seizures; cognitive effects |
| Vigabatrin | Irreversible GABA-T inhibitor | Infantile spasms, refractory focal seizures | Irreversible peripheral visual field defects (retinal toxicity) |
| Zonisamide | Na⁺ channel + T-type Ca²⁺ blocker | Focal & generalized | Nephrolithiasis, cognitive impairment, weight loss (similar to topiramate) |
Third-Generation AEDs
| Drug | Mechanism | Indications | Key Side Effects |
|---|---|---|---|
| Lacosamide | Enhances slow inactivation of Na⁺ channels | Focal & generalized | PR interval prolongation, dizziness |
| Pregabalin | α2δ Ca²⁺ channel blocker | Focal seizures (adjunctive) | Weight gain, edema, dizziness; also used for neuropathic pain and GAD |
| Perampanel | Non-competitive AMPA antagonist | Focal & generalized (adjunctive) | Dizziness, aggression, psychiatric effects |
| Brivaracetam | SV2A modulation (higher affinity than LEV) | Focal & generalized | Less mood disturbance than levetiracetam |
| Eslicarbazepine | Na⁺ channel blocker (active metabolite of oxcarbazepine) | Focal seizures (adjunctive) | Hyponatremia, hepatic enzyme induction |
Drug Selection by Seizure Type
| Seizure Type | First-line Drugs | Avoid |
|---|---|---|
| Focal seizures | Carbamazepine, levetiracetam, lamotrigine, oxcarbazepine | — |
| Generalized tonic-clonic | Valproate, levetiracetam, lamotrigine | — |
| Absence | Ethosuximide (first choice), valproate, lamotrigine | Carbamazepine, phenytoin, gabapentin (may worsen) |
| Juvenile myoclonic epilepsy (JME) | Valproate (highly effective), levetiracetam | Carbamazepine, lamotrigine (may worsen myoclonus) |
| Infantile spasms (West syndrome) | ACTH, vigabatrin, corticosteroids | — |
| Lennox-Gastaut syndrome | Valproate, clobazam, rufinamide, lamotrigine | — |
| Status epilepticus | Lorazepam/diazepam IV → phenytoin/fosphenytoin → midazolam or propofol infusion | — |
Important Pharmacokinetic Notes
- Phenytoin: Zero-order (nonlinear) kinetics at therapeutic levels — small dose changes cause large plasma level changes. Highly protein-bound (90%). Half-life ~24 h.
- Carbamazepine: Autoinduction (induces its own metabolism); half-life shortens from ~36 h initially to ~12 h after weeks of use.
- Valproate: CYP inhibitor (raises levels of lamotrigine, phenobarbital). Short half-life → divided dosing.
- Phenobarbital, phenytoin, ethosuximide: Long half-lives → once daily dosing acceptable.
- Levetiracetam: Renally cleared; minimal drug interactions.
Key Drug Interactions
- Enzyme inducers (lower levels of co-medications): Phenytoin, carbamazepine, phenobarbital, primidone, oxcarbazepine, lamotrigine
- Enzyme inhibitors (raise levels of co-medications): Valproate
- Adding valproate + lamotrigine: Valproate doubles lamotrigine levels → requires slow titration to avoid severe rash
- Oral contraceptives: Enzyme-inducing AEDs reduce contraceptive efficacy
Teratogenicity (Pregnancy Considerations)
All major AEDs carry some teratogenic risk. Valproate has the highest risk (neural tube defects, reduced IQ in offspring) and is avoided in women of childbearing potential whenever possible. Levetiracetam and lamotrigine are generally preferred in pregnancy. Folate supplementation (5 mg/day) is recommended in all women with epilepsy planning pregnancy.
Hypersensitivity and Rash
Aromatic AEDs (phenytoin, carbamazepine, phenobarbital, primidone, lamotrigine) share cross-hypersensitivity. HLA-B*1502 (Asian populations) is strongly associated with Stevens-Johnson syndrome/toxic epidermal necrolysis with carbamazepine. Screening is recommended before initiating carbamazepine in at-risk populations.
Discontinuation
Withdrawal may be considered after 2 seizure-free years on monotherapy:
- ~30–40% relapse rate at 2.5 years after stopping
- EEG with paroxysmal activity favors continued treatment
- Juvenile myoclonic epilepsy: likely requires lifelong therapy
- Abrupt withdrawal risks precipitating status epilepticus
Sources: Adams and Victor's Principles of Neurology, 12th Ed., Katzung's Basic and Clinical Pharmacology, 16th Ed., Bradley and Daroff's Neurology in Clinical Practice
Anti emetics drugs
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.