Give me information about consciousness and states of consciousness
Reading File
Searching the Web
consciousness states of consciousness neuroscience overview 2025
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have excellent material from multiple authoritative neuroscience textbooks plus a key diagram. Let me compile a comprehensive answer.
Consciousness and States of Consciousness
What Is Consciousness?
Consciousness is the state of full awareness of the self and one's relationship to the environment. Clinically, it is defined operationally by a patient's responses to the examiner -- but a person can be conscious yet unresponsive due to sensory or motor impairment (e.g., locked-in syndrome), so the determination of conscious state requires care.
Consciousness has two major dimensions:
- Content - the sum of all functions mediated at the cerebral cortical level, including both cognitive and affective responses. These are subserved by unique networks of cortical neurons. A strategically placed lesion can cause a fractional loss of consciousness -- a patient may be unaware of one class of stimuli (e.g., language symbols, the left side of space, faces) but otherwise fully conscious.
- Arousal (Level) - the overall level of behavioral responsiveness, regulated by brainstem and diencephalic pathways (the ascending reticular activating system) that regulate cortical function globally. A reduced level of consciousness results from widespread cortical impairment or injury to these specific arousal pathways -- not from focal cognitive deficits alone.
"Consciousness is the state of full awareness of the self and one's relationship to the environment."
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma
The Neuroscience of Consciousness
Neuroscientists generally subscribe to materialism/physicalism -- consciousness arises from physical processes in the brain. The alternative is dualism, the view that mind and body are fundamentally different. Most modern neuroscience assumes physicalism, though the "hard problem" remains unresolved.
The Easy vs. Hard Problems
- "Easy" problems: Explaining how the brain processes sensory information, how attention works, how behavior is integrated -- these are accessible to standard neuroscientific methods.
- The "hard problem": Why do subjective experiences (qualia) exist at all? Why does a mother's touch feel pleasant rather than producing the smell of burnt toast? We can find neural correlates of experience (the easy part), but explaining why the experience is the way it is remains far more difficult.
"The hard problem of consciousness is the experience itself. We experience the emotion called happiness, the sound of a saxophone playing jazz, the color blue. Why and how do these subjective experiences arise from physical processes?"
- Neuroscience: Exploring the Brain, 5th Edition
Neural Correlates of Consciousness (NCCs)
In the 1990s, Francis Crick and Christof Koch proposed studying neural correlates of consciousness (NCCs) - the minimal neuronal events sufficient for a specific conscious percept - as a tractable approach. Classic experiments use binocular rivalry (where two different images presented to separate eyes cause perception to alternate) to identify which brain areas track the conscious percept vs. the unchanged physical stimulus. fMRI studies show that the fusiform face area (FFA) and parahippocampal place area (PPA) activity alternates in concert with perception switches, suggesting they are NCCs for faces and places. Activation of the frontal cortex is considered necessary for visual percepts to enter consciousness. Synchronization of inputs through the thalamus to the cortex may be required before a perception becomes conscious.
States of Consciousness
The diagram below from Neuroscience: Exploring the Brain maps states by two axes: level of consciousness (wakefulness) on the x-axis and content of consciousness (awareness) on the y-axis:
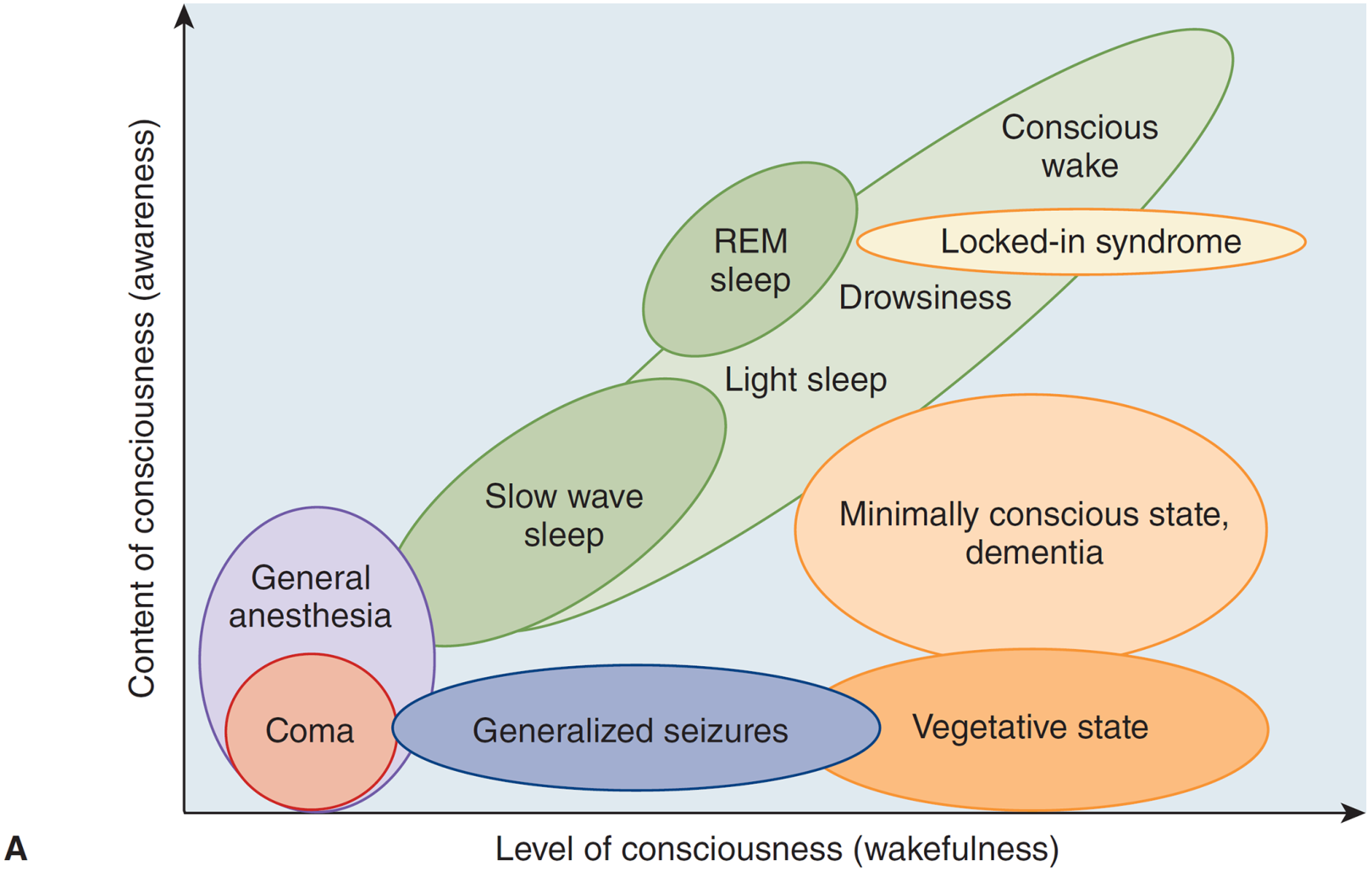
Normal States
| State | Wakefulness | Content/Awareness |
|---|---|---|
| Conscious wakefulness | High | High |
| Drowsiness | Moderate | Moderate |
| Light (NREM) sleep | Low-moderate | Low |
| Slow-wave (deep NREM) sleep | Low | Low |
| REM sleep | Low (physiologically) | Moderate-high (dreams) |
Sleep is a recurrent, physiologic form of reduced consciousness where brain systems responsible for cognitive function are globally reduced and do not respond readily to environmental stimuli. A key feature: sleep is intrinsically reversible -- sufficient stimulation returns the individual to wakefulness. REM sleep is unique in that content (dreams) can be relatively rich while the level of wakefulness is low.
Acute Altered States of Consciousness (Depressed)
These terms describe a spectrum of reduced arousal, from mild to profound, as outlined in Plum and Posner's Diagnosis and Treatment of Stupor and Coma:
Clouding of consciousness
Minimally reduced wakefulness or awareness, often with hyperexcitability and irritability alternating with drowsiness. Associated with reduced cerebral blood flow and oxygen consumption (e.g., hepatic encephalopathy, Wernicke's encephalopathy).
Delirium
A more florid abnormal mental state characterized by:
- Disturbance of attention and awareness
- Acute onset (hours to days) with fluctuating severity
- Additional disturbances in cognition (memory, orientation, language, perception)
- Often accompanied by misperceptions, vivid hallucinations, and disorientation
- Tends to last no more than 4-7 days in full form
Obtundation
Mild to moderate reduction in alertness with slower psychologic responses to stimulation. Increased sleep hours with drowsiness between bouts, but the patient remains responsive.
Stupor
Deep sleep-like state from which the subject can be aroused only with vigorous and continuous stimulation. Even when maximally aroused, cognitive function may be impaired.
Coma
A state of unresponsiveness in which the patient:
- Lies with eyes closed
- Cannot be aroused to respond appropriately to stimuli even with vigorous stimulation
- May grimace or show stereotyped limb withdrawal to pain
- Does not make localizing responses or discrete defensive movements
- As it deepens, even responses to pain may disappear
Continuous coma from brain injury rarely lasts more than 2-4 weeks. After this period, wake-sleep cycles gradually emerge as arousal circuitry reorganizes.
Subacute or Chronic Alterations of Consciousness
Vegetative state (Unresponsive Wakefulness Syndrome)
The patient opens eyes and may make facial expressions and body movements (wake-sleep cycles restored), but there is no evidence of awareness of self or environment. Little or no cortical activity, with brainstem activity persisting. Brain injury or stroke is the usual cause.
Minimally conscious state (MCS)
Superficially similar to vegetative state, but there is some evidence of self or environmental awareness (intelligible speech, purposeful movement in response to a stimulus). EEG shows notably greater activity than in vegetative state, including both primary sensory and association cortex. This distinction is clinically important for estimating recovery.
Locked-in syndrome
The patient is not unconscious, but de-efferented -- paralysis of all four limbs and lower cranial nerves, typically from a lesion at the base/tegmentum of the midpons interrupting descending motor pathways while leaving the cerebral cortex intact. Vertical eye movements and eyelid opening are usually preserved. PET scans show brain activity comparable to a conscious control. These patients suffer greatly if treated as nonresponsive, and the examiner must verify responsiveness via eye blink codes.
Dementia
An enduring, often progressive decline in mental processes due to organic disorder, not typically accompanied by reduced arousal (until very advanced stages).
Brain death
Complete and irreversible cessation of all brain function, including the brainstem.
Altered States (Not Purely Depressed)
| State | Notes |
|---|---|
| General anesthesia | Pharmacologically induced; low content and level; reversible |
| Generalized seizures | Paradoxically high electrical activity, low awareness |
| Hallucinogen-induced states | Altered content of consciousness with variable arousal |
| Meditation / flow states | Modified content with sustained or altered arousal |
Theories of Consciousness
Several major neuroscientific frameworks attempt to explain how consciousness arises:
-
Global Workspace Theory (GWT) - Consciousness arises when information is "broadcast" across a global workspace to many brain modules simultaneously. Information that reaches this workspace becomes conscious; everything else remains unconscious processing.
-
Integrated Information Theory (IIT) - Proposed by Giulio Tononi. Consciousness is identical to integrated information (measured as Φ, "phi"). Any system with high Φ has some degree of consciousness. This theory predicts that consciousness is graded and potentially present in simple systems.
-
Higher-Order Theories - A mental state is conscious only when represented by a higher-order mental state (a thought about a thought). Frontal cortical involvement is key.
-
Attention Schema Theory - The brain builds a simplified model ("attention schema") of its own attention process, and this model is what we call consciousness.
Neural Substrates of Consciousness
- Ascending Reticular Activating System (ARAS): Brainstem network (reticular formation, locus coeruleus, raphe nuclei, pedunculopontine nucleus) that drives thalamocortical arousal. Damage here causes coma even with intact cortex.
- Thalamus: Acts as a relay and gating system. Thalamocortical synchrony is thought essential for conscious awareness.
- Cerebral cortex: Provides the content of consciousness. The posterior parietal cortex and prefrontal cortex are especially implicated.
- Default Mode Network (DMN): Active during rest/daydreaming, involved in self-referential thought and internal consciousness.
- Prefrontal cortex: Necessary for conscious percepts to reach awareness; interacts with visual association cortex for attention and working memory.
Key Clinical Takeaway
The distinction between level (wakefulness/arousal) and content (awareness/cognition) is the most practically important framework. A person can be awake (high level) but unaware (low content) -- as in vegetative state -- or aware (relatively high content) while appearing unresponsive -- as in locked-in syndrome. Treatment and prognosis differ fundamentally across these states.
Sources:
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma (9780190208875), pp. 23-29
- Neuroscience: Exploring the Brain, 5th Edition (9781284286878), pp. 1918-1930
- Bradley and Daroff's Neurology in Clinical Practice (9780323642613), pp. 96-97
- Stanford Encyclopedia of Philosophy: Neuroscience of Consciousness (Summer 2025 edition)
This is a shared conversation. Sign in to Orris to start your own chat.