Complication of thyriodectomy
Reading File
Finding Sources
Searching PubMed
"thyroidectomy"[MeSH Terms] AND "postoperative complications"[MeSH Terms]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to provide a comprehensive answer. Here is a detailed, textbook-sourced response:
Complications of Thyroidectomy
The overall complication rate in experienced hands is less than 1%, but total thyroidectomy carries roughly a twofold higher risk of most complications compared to lobectomy. - Sabiston Textbook of Surgery, Current Surgical Therapy 14e
I. Haemorrhage / Neck Haematoma
The most frequent life-threatening complication. Around 1 in 50 patients (2%) develop a post-operative haematoma, with almost all cases occurring within the first 24 hours.
Mechanism: An arterial bleed raises central compartment pressure, which exceeds venous pressure, causing venous oedema of the larynx and potentially fatal airway obstruction.
Management:
- Immediate removal of skin sutures to decompose pressure
- Secure airway with endotracheal intubation
- Return to theatre for haematoma evacuation and haemostasis
- Wound drains have NOT been shown to prevent haematoma
This complication is the primary reason thyroidectomy remains an inpatient procedure in many centres. - Bailey & Love's Short Practice of Surgery, 28th Ed.
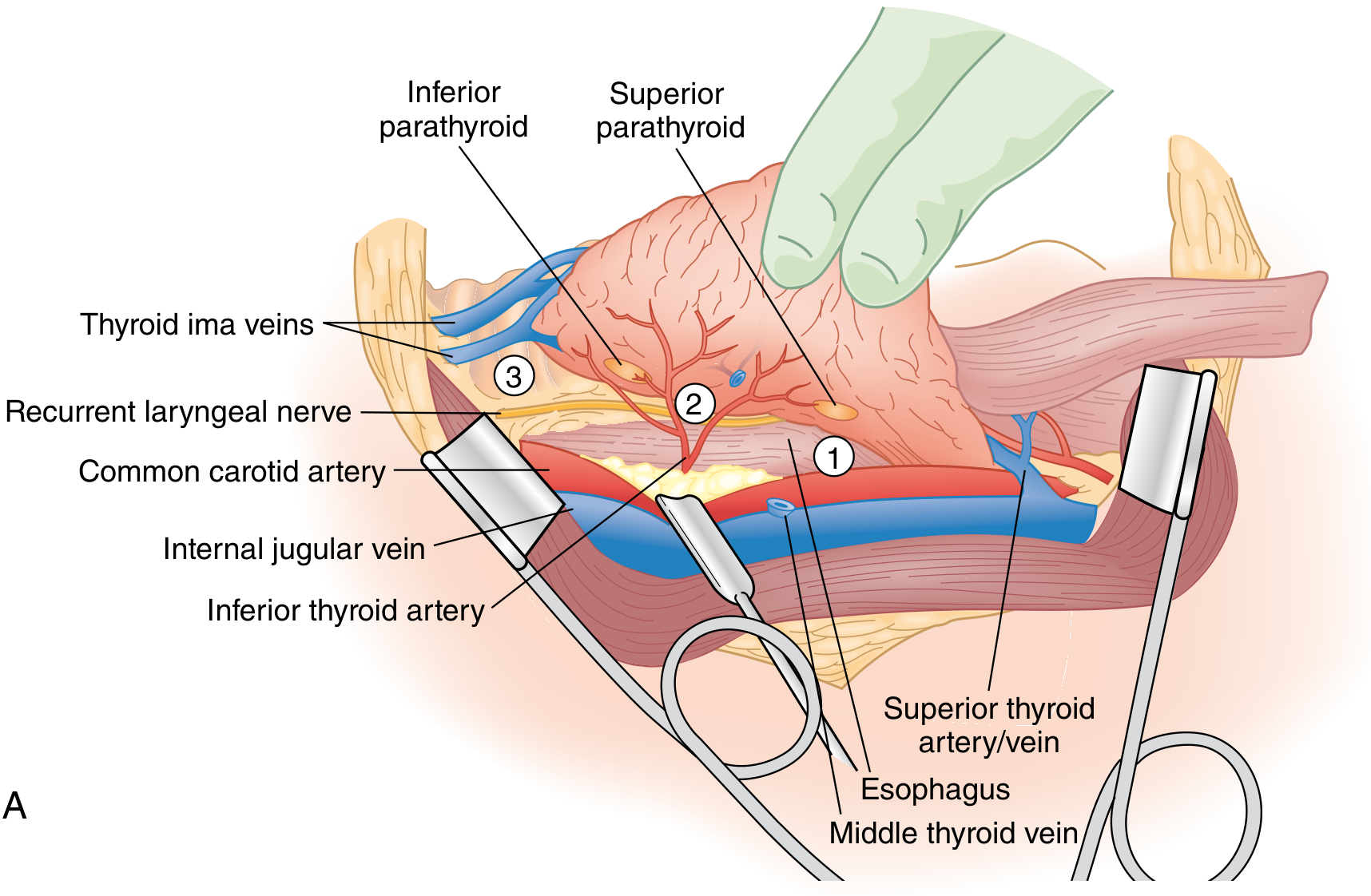
II. Recurrent Laryngeal Nerve (RLN) Injury
The most important nerve complication. The RLN is at greatest risk at three points (shown in figure below):
- The ligament of Berry
- During ligation of branches of the inferior thyroid artery
- At the thoracic inlet
Injury patterns:
- Unilateral - hoarse voice, weak cough; usually tolerated
- Bilateral - severe airway compromise; may require tracheostomy
- Transient - far more common; detected only by routine laryngoscopy
- Permanent - rare if the nerve was positively identified during surgery
Rates (BAETS audit): RLN palsy rate of 1.8% at 1 month, declining to 0.5% at 3 months for first-time operations.
Management:
- Transected ends: immediate reanastomosis if identified
- If a segment is excised (e.g. due to malignancy): ansa cervicalis anastomosis (does not restore cord mobility but prevents denervation atrophy and improves voice quality)
- Conservative: speech therapy for permanent paralysis
- Surgical: medialisation procedures if voice quality unacceptable
- Bailey & Love's Short Practice of Surgery, 28th Ed.
III. External Branch of the Superior Laryngeal Nerve (EBSLN) Injury
Injury is more common than appreciated because the EBSLN runs in close proximity to the superior thyroid artery.
Effect: Loss of vocal cord tension, resulting in diminished power and range of voice - particularly noticed by professional voice users (singers, teachers, lawyers). Changes are often subtle and only detectable on formal voice assessment. - Bailey & Love's
IV. Hypoparathyroidism
The most common endocrine complication of total thyroidectomy. Caused by:
- Inadvertent removal of parathyroid glands
- Infarction through damage to parathyroid end-arteries (more important)
- Both often occur together
Types:
| Type | Timing | Outcome |
|---|---|---|
| Transient | 2-5 days post-op | Very common; resolves |
| Permanent | Persistent >6 months | Should be <1% in expert hands |
Risk factors for permanent hypoparathyroidism (2024 meta-analysis, PMID 38652139): total thyroidectomy, central neck dissection, Graves disease, high surgical volume inversely protective.
Presentation:
- Perioral paraesthesia, tingling fingers/toes (early)
- Tetany, Chvostek's sign, Trousseau's sign
- Laryngospasm (severe cases)
- ECG changes (prolonged QT interval)
Important notes:
- Complication is essentially limited to total thyroidectomy - lobectomy leaves contralateral glands intact
- Total thyroidectomy + central neck dissection places parathyroids at greatest risk
- Most cases present 2-5 days post-op; rarely delayed 2-3 weeks
Management:
- Prophylactic oral calcium + calcitriol supplementation (especially for Graves)
- Monitor intraoperative PTH or early post-op PTH levels to guide supplementation
- Emerging: intraoperative parathyroid imaging using NIR autofluorescence or indocyanine green to identify and preserve glands
- Sabiston Textbook of Surgery
V. Thyroid Insufficiency (Hypothyroidism)
- Total thyroidectomy: thyroxine replacement required in ALL patients; started on post-op day 1
- Lobectomy: approximately 1 in 3 patients will require supplementation; higher rates in those with thyroid autoantibodies
- Subtotal thyroidectomy was historically performed to preserve function but has largely been abandoned because judging residual volume is imprecise and recurrence requires difficult re-operation. - Bailey & Love's
VI. Thyrotoxic Crisis (Thyroid Storm)
Now extremely rare due to better pre-operative preparation.
Mechanism: Occurs when a thyrotoxic patient is inadequately prepared for surgery - acute exacerbation of hyperthyroidism triggered by the operative stress.
Management:
- Supportive: IV fluids, cooling (ice packs), oxygen, diuretics, sedation, IV hydrocortisone, digoxin for AF
- Specific:
- Carbimazole 10-20 mg every 6 hours
- Lugol's iodine 10 drops every 8 hours (or sodium iodide 1 g IV)
- Propranolol 1-2 mg IV (or 40 mg orally every 6 hours) to block beta-adrenergic effects
- Bailey & Love's, p. 887
VII. Wound Complications
| Complication | Notes |
|---|---|
| Wound infection | Cellulitis is more common than surgeons appreciate; deep cervical abscess is rare and requires drainage |
| Hypertrophic/keloid scar | More likely over the sternum and in dark-skinned individuals; treat with intradermal corticosteroid injections monthly |
| Stitch granuloma | With or without sinus formation; occurs with non-absorbable (especially silk) sutures - use absorbable sutures throughout |
VIII. Dysphagia
A 2026 systematic review (PMID 41901524) confirmed that post-thyroidectomy dysphagia is a recognised but often underreported complication. Mechanisms include:
- Dissection around the tracheo-oesophageal region
- Injury to superior laryngeal nerve branches affecting pharyngeal sensation
- Scar tissue and adhesion formation
IX. Complications Specific to Remote-Access / Robotic Thyroidectomy
- Brachial plexus injury (transaxillary approach)
- Tracheo-oesophageal injury
- Lymph leak
- Arm lymphoedema
- Higher learning curve required - early US experience with robotic transaxillary approach showed increased complication rates leading to FDA warnings (2013)
- Sabiston Textbook of Surgery
Summary Table
| Complication | Frequency | When |
|---|---|---|
| Neck haematoma | ~2% | Within 24 hours |
| Transient RLN palsy | ~1.8% at 1 month | Immediate |
| Permanent RLN palsy | ~0.5% | Long-term |
| Transient hypoparathyroidism | Common | 2-5 days |
| Permanent hypoparathyroidism | <1% (expert) | >6 months |
| Hypothyroidism | 100% (total), ~33% (lobectomy) | Long-term |
| EBSLN injury | Underreported | Immediate |
| Thyroid storm | Rare (with prep) | Perioperative |
| Wound infection | Occasional | 1-2 weeks |
| Keloid/hypertrophic scar | Variable | Weeks-months |
Key preventive principle: Surgeon volume is the single most important modifiable risk factor - outcomes improve up to a threshold of ~26 total thyroidectomies per year. Positive identification of the RLN and all four parathyroid glands during surgery is mandatory. - Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.