
Screenshot_2026-07-11-20-03-01-121_com.google.android.googlequicksearchbox.jpg
What is this at the foot
Reading File
analyse_media
Finding Sources
Searching the Web
lichenified skin foot thickened hyperpigmented skin lines dermatology causes
Reading File
Loading Image
The skin on your foot shows classic features of lichenification - most likely Lichen Simplex Chronicus (LSC), also called circumscribed neurodermatitis. Here is a comparison with a textbook case:
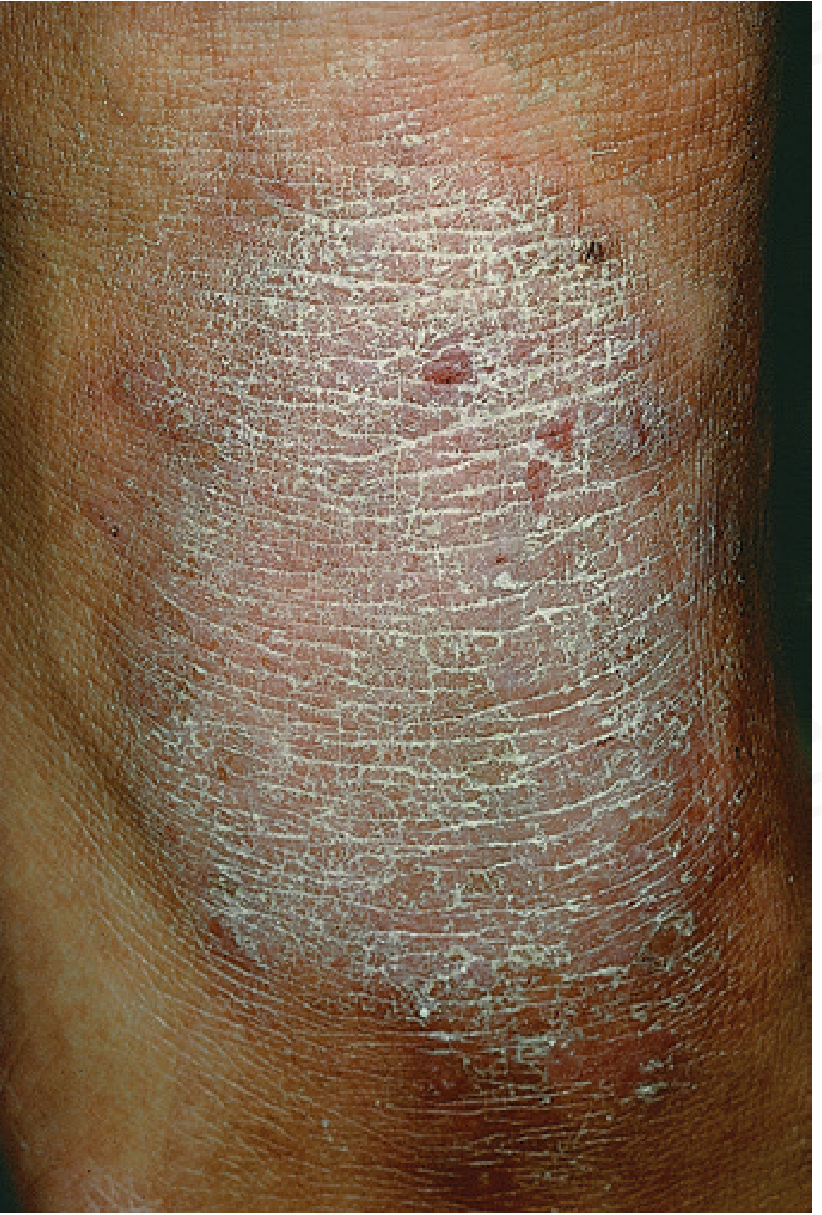
What You're Seeing
The image shows three characteristic features:
- Thickened, leathery skin - the skin has grown thicker than normal
- Exaggerated/deep skin lines - the natural markings form a prominent crisscross mosaic pattern of flat-topped facets
- Hyperpigmentation - darkening of the affected area
This pattern is called lichenification, and the foot/ankle area is one of the classic sites for it.
Most Likely Cause: Lichen Simplex Chronicus
According to Andrews' Diseases of the Skin (Clinical Dermatology), LSC "results from long-term chronic rubbing and scratching, more vigorously than a normal pain threshold would permit, with the skin becoming thickened and leathery. The normal markings of the skin become exaggerated so that the striae form a crisscross pattern." The soles, ankles, and wrist flexures are common sites.
The itch-scratch cycle is the core driver: an itch triggers scratching, which thickens the skin, which causes more itch, and so on.
Other Conditions to Rule Out
| Condition | Key Feature |
|---|---|
| Chronic eczema / atopic dermatitis | Often the underlying trigger for LSC |
| Tinea pedis (fungal infection) - moccasin type | Dry, thick, scaling; usually itchy |
| Callus/frictional dermatitis | From repetitive shoe friction; no intense itch |
| Acanthosis nigricans | Velvety texture; linked to insulin resistance/diabetes |
What to Ask Yourself
- Does it itch constantly, especially at night?
- Do you find yourself rubbing or scratching this spot habitually?
- Do you have a history of eczema, allergies, or asthma?
- Have you had athlete's foot (tinea) before?
Self-Care While You Wait for a Doctor
- Stop scratching - this is the most important step; breaking the itch-scratch cycle is the goal
- Moisturize heavily with a thick cream containing urea or lactic acid after bathing
- Check your footwear - if shoes are rubbing this area, change to better-fitting ones or use padding
- Cut nails short to reduce damage from scratching
Treatment (by a doctor)
Per Andrews' Diseases of the Skin:
- High-potency topical corticosteroid (e.g., betamethasone cream/ointment) - first-line, but not for indefinite use
- Occlusive dressings (e.g., Unna boot for severe cases) to break the scratch cycle
- Intralesional triamcinolone injections for stubborn patches
- Topical calcineurin inhibitors (tacrolimus/pimecrolimus) as alternatives
- Addressing any underlying anxiety or OCD if that is driving the scratching behavior
A dermatologist visit is recommended to confirm the diagnosis and exclude a fungal infection (which requires a completely different treatment - antifungals, not steroids).
Disclaimer: This is for informational purposes only and is not a medical diagnosis. Please consult a dermatologist or your doctor for a proper evaluation.
It doesn't itch
Asking for Preferences
Finding Sources
Reading File
This fits the picture very well now. Here is the most likely explanation:
Callus (Hyperkeratosis) from Barefoot Walking
The combination of:
- No itching
- Side of the foot
- Walking barefoot often
...points strongly to a callus - a non-penetrating, diffuse thickening of the skin caused by repeated pressure and friction against the ground.
According to Andrews' Diseases of the Skin, a callus is "a nonpenetrating, circumscribed hyperkeratosis produced by pressure. It occurs on parts of the body subject to intermittent pressure, particularly the palms and soles, and especially the bony prominences." The skin lines become exaggerated and the area darkens over time as a mechanical protective response - exactly what's visible in your image.
The side of the foot is a classic spot because it bears lateral pressure when walking, especially on uneven ground without footwear.
Is It Dangerous?
No. A callus is completely benign. It is your skin protecting itself. There is no risk of it becoming cancerous or spreading.
What You Can Do
| Step | What to do |
|---|---|
| Wear footwear | Even simple sandals or slippers when walking on hard or rough surfaces will reduce the pressure |
| Moisturize daily | Apply a thick cream with urea (10-20%) or lactic acid (12%) after bathing - these soften thickened skin |
| Gentle filing | After soaking the foot in warm water for 10-15 minutes, use a pumice stone or foot file to gently reduce the thickness |
| 40% salicylic acid plaster | Available at pharmacies; placed over the callus to chemically soften it |
As Andrews' notes: "Callus tends to disappear spontaneously when the pressure is removed." So if you start wearing footwear regularly, it will gradually thin out on its own over weeks to months.
No doctor visit is urgently needed for a simple callus, but if it becomes painful, cracks open, or grows rapidly, it is worth seeing a dermatologist to confirm and rule out other causes.
Can callus be formed on side of foot
Finding Sources
Searching the Web
callus on side of foot lateral border causes barefoot walking
Yes, 100%. The side of the foot is actually one of the named classic locations for callus formation.
The Cleveland Clinic specifically lists calluses as forming "along the sides of your feet" - it is explicitly mentioned as a typical site, not an unusual one.
Here is why the side of the foot gets calluses:
1. Lateral weight-bearing during barefoot walking
When you walk barefoot, especially on hard floors or ground, the outer (lateral) border of the foot takes significant ground contact with each step. Over time this repeated pressure triggers skin thickening.
2. Gait pattern
Many people naturally supinate (roll slightly outward) when walking, which concentrates pressure on the outer edge of the foot - a well-known callus zone.
3. No shoe protection
Footwear normally cushions and distributes this lateral pressure. Walking barefoot removes that buffer entirely, so the skin compensates by thickening.
4. Bony prominence
The 5th metatarsal head (the bony bump on the outer side of the foot) creates a natural pressure point - calluses frequently form directly over it.
So to summarize: what you have is almost certainly a lateral foot callus from habitual barefoot walking. It is benign, very common, and will gradually reduce if you:
- Start wearing footwear or cushioned slippers regularly
- Apply a urea-based moisturizer (10-20% urea cream) daily
- Occasionally use a pumice stone after soaking in warm water
This is a shared conversation. Sign in to Orris to start your own chat.