Diagnostic approach to pulmonary hypertension for exam purpose 10 marks answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive, detailed information from multiple authoritative textbooks. Let me compile the full exam-ready answer.
Diagnostic Approach to Pulmonary Hypertension
Definition and Hemodynamic Criteria
Pulmonary hypertension (PH) is defined hemodynamically as a mean pulmonary artery pressure (mPAP) > 20 mmHg at rest, measured by right heart catheterization (RHC). Pulmonary arterial hypertension (PAH, Group I) additionally requires:
- Pulmonary artery wedge pressure (PAWP) ≤ 15 mmHg (to exclude left heart disease)
- Pulmonary vascular resistance (PVR) ≥ 3 Wood units
(Fishman's Pulmonary Diseases & Disorders)
WHO Clinical Classification (5 Groups)
| Group | Cause |
|---|---|
| I | Pulmonary arterial hypertension (idiopathic, heritable, drug/toxin-induced, CTD, HIV, portal HTN, congenital heart disease) |
| II | Left heart disease (LV systolic/diastolic dysfunction, valvular disease) |
| III | Lung disease / hypoxia (COPD, ILD, sleep-disordered breathing) |
| IV | Chronic thromboembolic PH (CTEPH) |
| V | Unclear/multifactorial (hematologic, systemic, metabolic disorders) |
Step-by-Step Diagnostic Approach
Step 1 - Clinical Suspicion (History & Symptoms)
Symptoms are nonspecific and often lead to delayed diagnosis:
- Progressive exertional dyspnea (most common presenting symptom)
- Fatigue, weakness
- Angina, syncope or pre-syncope on exertion (suggests low cardiac output)
- Peripheral edema, abdominal distension (right heart failure)
Risk factors / associations to screen for:
- Connective tissue disease (scleroderma, SLE, MCTD, RA)
- Prior pulmonary embolism or DVT
- HIV infection, cirrhosis/portal hypertension
- Congenital heart disease
- Drug/toxin exposure (anorexigens, methamphetamine, dasatinib)
- Family history of PAH (BMPR2 mutation)
Step 2 - Physical Examination
| Finding | Significance |
|---|---|
| Loud/accentuated P2 (heard at apex in >90%) | Elevated pulmonary pressure |
| Right parasternal heave/lift | RV hypertrophy |
| Early systolic click | High pulmonary pressure |
| Midsystolic ejection murmur over pulmonary area | Turbulent transpulmonary flow |
| RV S4 gallop (38%) | RV hypertrophy |
| Holosystolic murmur increasing with inspiration | Tricuspid regurgitation |
| Diastolic murmur (Graham Steell) | Pulmonary regurgitation |
| Elevated JVP with prominent "a" wave | Poor RV compliance |
| Elevated JVP with "v" waves, pulsatile liver | Tricuspid regurgitation |
| RV S3 (23%), hepatomegaly, edema, ascites | RV failure (advanced PH) |
| Sclerodactyly, telangiectasia, Raynaud's | Scleroderma-associated PAH |
| Clubbing | Congenital heart disease or PVOD |
(Fishman's Pulmonary Diseases & Disorders)
Step 3 - Initial Investigations
A. Electrocardiogram (ECG)
- Right axis deviation
- RV hypertrophy (tall R in V1, deep S in V5-V6)
- Right atrial enlargement (P pulmonale: peaked P in II > 2.5 mm)
- Right bundle branch block
- RV strain pattern: S1Q3T3 pattern
- Note: ECG has low sensitivity in early/mild PH
B. Chest X-Ray (CXR)
- Prominent central pulmonary arteries (hilar fullness)
- Peripheral vascular pruning (oligemia at periphery) - characteristic of PAH
- Cardiomegaly, RV enlargement (loss of retrosternal space on lateral view)
- Dilated right descending pulmonary artery (> 16 mm)
- Clues to etiology:
- Interstitial infiltrates - ILD
- Hyperinflated lungs - COPD
- Regional oligemia - CTEPH
- Plethoric lung fields throughout - congenital left-to-right shunt
Step 4 - Echocardiography (KEY Non-Invasive Test)
Transthoracic echocardiography (TTE) with Doppler is the initial test of choice when PH is suspected.
Key findings:
- Estimated PASP by Doppler of tricuspid regurgitant jet (sensitivity 80-100%; correlation with invasive measurement r = 0.6-0.9)
- PASP = 4 × (TR velocity)² + RAP
- RV changes: RV hypertrophy and dilation, reduced RV systolic function, reduced TAPSE (< 1.8 cm = worse survival)
- Septal flattening (D-shaped LV in systole) - pressure overload pattern
- Pericardial effusion - marker of severity
- LV compression from RV dilation
- Evidence of left heart disease: LV dysfunction, left-sided valvular disease, left atrial enlargement (diastolic dysfunction)
Echocardiographic probability of PH:
- Low probability: TRV ≤ 2.8 m/s, no other signs
- Intermediate probability: TRV ≤ 2.8 m/s with other signs, OR TRV 2.9-3.4 m/s without signs
- High probability: TRV > 3.4 m/s, OR TRV 2.9-3.4 m/s with other signs
Transesophageal echocardiogram (TEE): Indicated to exclude intracardiac shunts (ASD, PFO) suspected on TTE.
Step 5 - Laboratory Investigations
| Test | Purpose |
|---|---|
| CBC | Polycythemia (hypoxic PH), anemia (high-output PH) |
| LFTs | Portal hypertension (portopulmonary HTN) |
| Renal function | Cardiorenal syndrome |
| Hepatitis B & C serologies | Portal/hepatic disease |
| HIV serology | HIV-associated PAH |
| ANA, anti-Scl-70, anti-centromere, ENA | CTD-associated PAH |
| Antiphospholipid antibody, lupus anticoagulant | CTEPH predisposition |
| TSH (thyroid function) | Thyroid disease (high-output PH) |
| BNP / NT-proBNP | Severity assessment, prognosis, monitoring |
| 6-minute walk test (6MWT) | Functional capacity, correlates with WHO FC and prognosis |
| ABG | PaO2 (hypoxemia), PaCO2 (hypoventilation) |
Step 6 - Pulmonary Function Tests (PFTs)
- Spirometry + lung volumes: Exclude obstructive (COPD) or restrictive (ILD) disease
- DLCO:
- Mildly reduced in PAH
- Severely reduced (< 40% predicted) = suggests ILD or PAH with venous/capillary involvement (PVOD)
- ABG: Hypoxemia common; hypercapnia suggests hypoventilation
Step 7 - Ventilation-Perfusion (V/Q) Scan
- Critical test to exclude CTEPH (Group IV)
- Sensitivity for CTEPH is higher than CT-PA alone
- One or more segmental mismatched perfusion defects warrants CT pulmonary angiography or conventional pulmonary angiography
- May be abnormal in PAH with venous/capillary involvement and fibrosing mediastinitis
- A normal V/Q scan essentially excludes CTEPH
Step 8 - CT Imaging
- HRCT chest: Assess for ILD, emphysema, mediastinal fibrosis, PVOD (ground-glass opacities, septal lines, lymph node enlargement)
- CT pulmonary angiography: Confirms CTEPH if V/Q scan is suspicious; determines surgical feasibility (endarterectomy); should NOT be used as the primary screen for CTEPH
- Additional CT findings in PAH: Dilated main PA (> 29 mm), main PA:Aorta ratio > 1
Step 9 - Sleep Study
- Nocturnal oximetry / polysomnography if:
- Symptoms of sleep-disordered breathing (snoring, witnessed apneas, daytime somnolence)
- Daytime hypercapnia on ABG
- Nocturnal desaturations on oximetry
Step 10 - Right Heart Catheterization (RHC) - Gold Standard
Mandatory for:
- Confirming diagnosis of PH
- Determining hemodynamic severity
- Differentiating group (PAH vs. left heart disease vs. others)
- Guiding therapy
- Performing acute vasodilator testing
Key measurements:
| Parameter | Normal | PAH Criteria |
|---|---|---|
| mPAP | < 20 mmHg | > 20 mmHg |
| PAWP | ≤ 15 mmHg | ≤ 15 mmHg (to confirm pre-capillary PH) |
| PVR | < 3 WU | ≥ 3 Wood units |
| Cardiac output | Normal | Often reduced |
- PVR = (mPAP - PAWP) / Cardiac Output
- Serial O2 saturations at each level detect "step-up" (left-to-right shunting)
- PAWP measured at end-expiration to avoid respiratory artifact
- Left heart catheterization may be added to measure LVEDP directly (if PAWP is discrepant or left heart disease is suspected)
Acute Vasodilator Testing (AVT):
- Performed at time of RHC in selected PAH patients
- Agents: inhaled nitric oxide, IV adenosine, or IV epoprostenol
- Positive response (Sitbon criteria): mPAP fall ≥ 10 mmHg to an absolute value ≤ 40 mmHg, with unchanged or increased cardiac output
- ~7% of patients with idiopathic PAH respond positively - these may be treated with calcium channel blockers
Diagnostic Algorithm (Summary Flowchart)
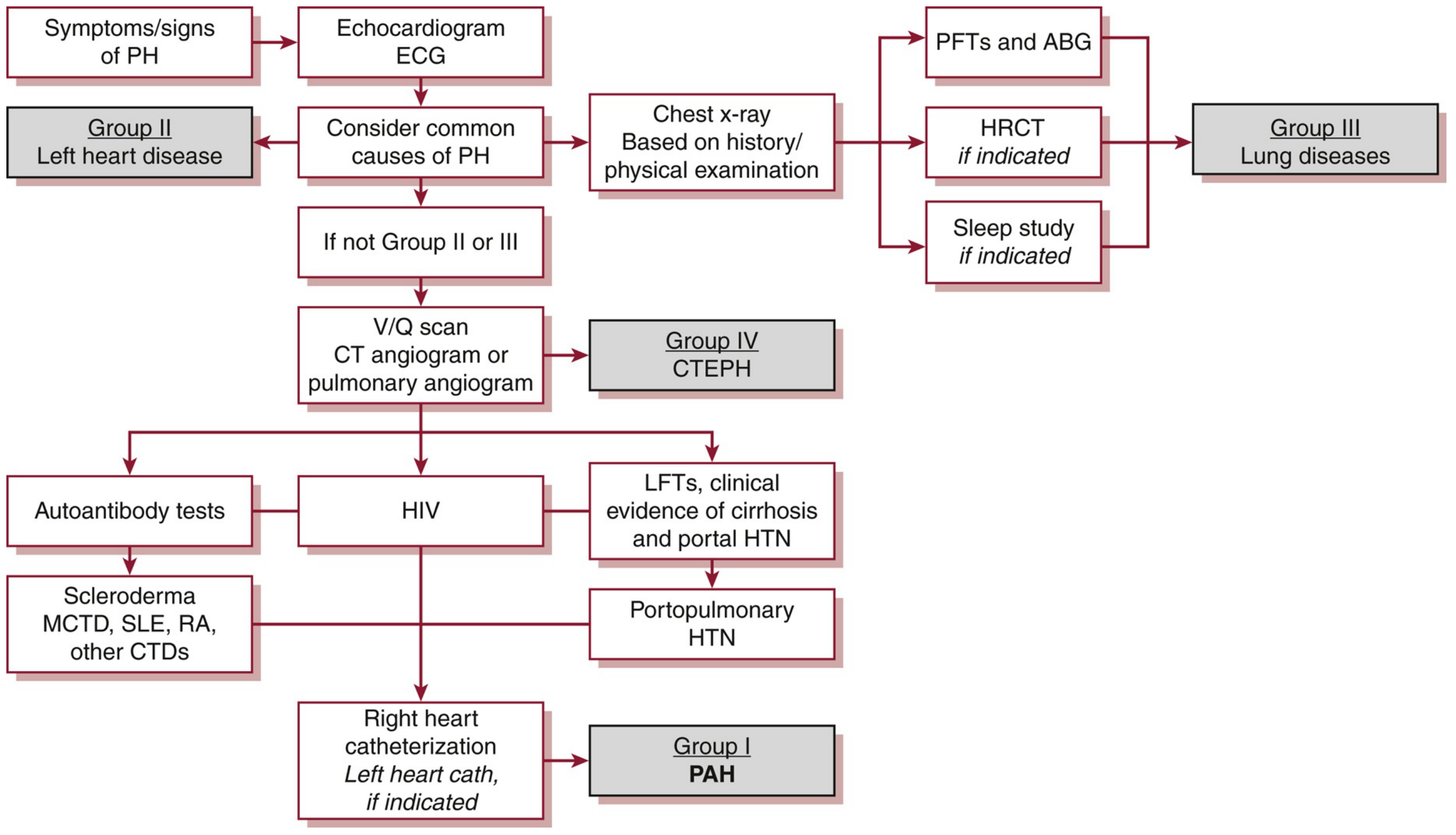
Figure: Diagnostic algorithm for PH. Symptoms/signs → Echo + ECG → Evaluate for Group II (left heart) and Group III (lung disease) → V/Q scan ± CT angiography to exclude Group IV (CTEPH) → Autoantibodies, HIV, LFTs → RHC to confirm Group I PAH. (Washington Manual of Medical Therapeutics)
Functional Assessment - WHO/NYHA Functional Classification
| Class | Description |
|---|---|
| I | No symptoms with ordinary activity |
| II | Slight limitation; comfortable at rest; symptoms with ordinary activity |
| III | Marked limitation; comfortable at rest; symptoms with less-than-ordinary activity |
| IV | Symptoms at rest; signs of RV failure |
Risk Stratification
Low-risk indicators for PAH (good prognosis):
- WHO FC I or II
- 6MWT distance > 440 m
- Normal or near-normal BNP/NT-proBNP
- No RV failure, no pericardial effusion, normal cardiac index
High-risk indicators: FC IV, rapidly progressive symptoms, RV failure, 6MWT < 165 m, markedly elevated NT-proBNP, pericardial effusion, severely reduced cardiac index.
Key Points to Remember for Exam
- Echo is the initial screening test; RHC is the gold standard for confirming diagnosis.
- V/Q scan is the investigation of choice to screen for CTEPH - CT-PA alone may miss it.
- New mPAP threshold is > 20 mmHg (updated from the old > 25 mmHg - per 2022 ESC/ERS guidelines).
- PAH diagnosis requires mPAP > 20 mmHg + PVR ≥ 3 WU + PAWP ≤ 15 mmHg.
- Acute vasodilator testing identifies the ~7% who may respond to calcium channel blockers.
- BNP/NT-proBNP reflects RV strain and is key for severity and monitoring.
- DLCO < 40% suggests ILD or PVOD rather than pure PAH.
- The S1Q3T3 and RV strain pattern on ECG indicate significant PH.
References:
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set (Table 72-6, 72-7)
- The Washington Manual of Medical Therapeutics (Chapter 10, Fig. 10-1)
- Goldman-Cecil Medicine, International Edition (Chapter 69)
- Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.