provide defenition, types, causes, pathophysiology, diagnostic approach , management along with pharmacology for ARF
"acute kidney injury"[MeSH Terms] AND management
Acute Renal Failure (ARF) / Acute Kidney Injury (AKI)
Note on terminology: The term "Acute Renal Failure" (ARF) has largely been replaced by Acute Kidney Injury (AKI) in current literature, as it better reflects the spectrum from mild to severe dysfunction. Both terms refer to the same clinical entity.
1. Definition
KDIGO Staging Criteria
| Stage | Serum Creatinine | Urine Output |
|---|---|---|
| 1 | 1.5-1.9× baseline OR ≥0.3 mg/dL (≥26.5 µmol/L) increase | <0.5 mL/kg/hr for 6-12 hours |
| 2 | 2.0-2.9× baseline | <0.5 mL/kg/hr for ≥12 hours |
| 3 | ≥3.0× baseline OR ≥4.0 mg/dL (≥353.6 µmol/L) OR initiation of RRT OR in patients <18 yr, eGFR <35 mL/min/1.73 m² | <0.3 mL/kg/hr for ≥24 hours OR anuria for ≥12 hours |
- Goldman-Cecil Medicine, International Edition, pp. 1241-1248
- Brenner and Rector's The Kidney, 2-Volume Set
2. Classification / Types
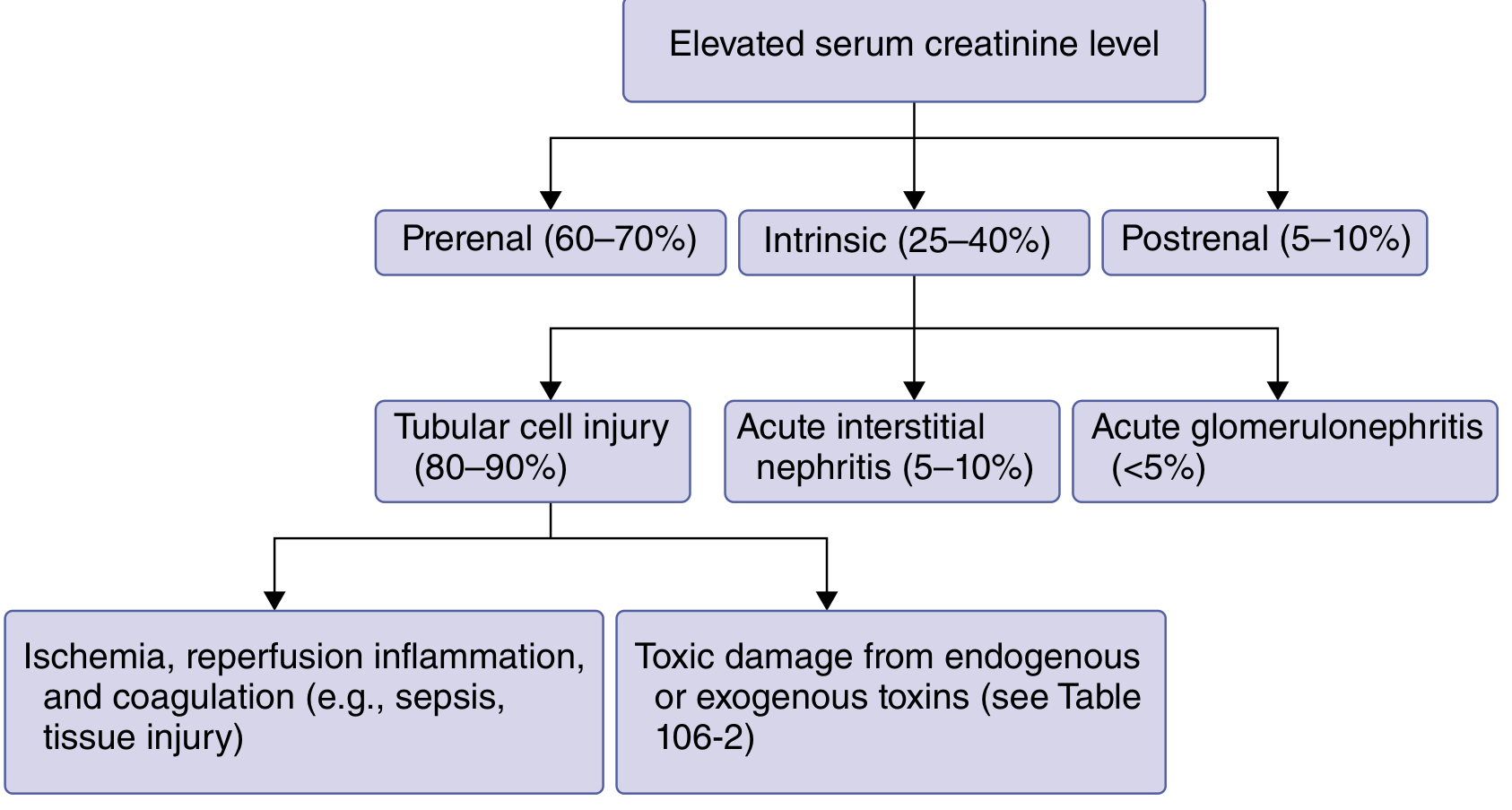
A. Prerenal AKI (60-70% of cases)
B. Intrinsic (Renal/Intrarenal) AKI (25-40% of cases)
- Tubular cell injury (80-90% of intrinsic): ATN from ischemia/toxins
- Acute Interstitial Nephritis (5-10%)
- Acute Glomerulonephritis (<5%)
C. Postrenal AKI (5-10% of cases)
3. Causes
Prerenal Causes
- Hemorrhage (traumatic, GI, surgical)
- GI losses (vomiting, diarrhea, NG suction)
- Renal losses (overdiuresis, diabetes insipidus)
- Third-spacing (pancreatitis, hypoalbuminemia, burns, fever/sweating)
- Cardiogenic shock / acute cardiac failure
- Septic shock
- Cirrhosis/liver failure
- Anaphylaxis
- NSAIDs (reduce prostaglandin-mediated afferent dilation)
- ACE inhibitors and ARBs (reduce efferent vasoconstriction)
- Cyclosporine, radiocontrast agents
Intrinsic Renal Causes
- Any prolonged prerenal cause that is not corrected promptly
- Drug nephrotoxicity: aminoglycosides, amphotericin B, cisplatin, radiocontrast agents, vancomycin, tenofovir, acyclovir, foscarnet, NSAIDs
- Endogenous toxins: myoglobin (rhabdomyolysis), hemoglobin (hemolysis), uric acid, calcium oxalate, pancreatic enzymes
- Exogenous toxins: metals (iron, cadmium), toluene, ethylene glycol, cocaine, methotrexate, tacrolimus
- Drugs: sulfonamides, penicillins, cephalosporins, ciprofloxacin, rifampin, NSAIDs, proton pump inhibitors, furosemide, thiazides, allopurinol, checkpoint inhibitors
- Infections: Legionella, leptospirosis, streptococcus, EBV, CMV, SARS-CoV-2, TB
- Systemic disease: SLE, Sjögren syndrome, sarcoidosis, cryoglobulinemia
- Rapidly progressive glomerulonephritis (RPGN): ANCA-associated vasculitides, Goodpasture disease, crescentic GN
- Thrombotic microangiopathies (TTP, HUS)
- Cryoglobulinemia
- Aortic dissection
- Renal artery/vein thrombosis
- Atheroembolism
- Rhabdomyolysis
- Hepatorenal syndrome
- Urate nephropathy
Postrenal Causes
-
Lower tract: Prostatic hypertrophy (most common in older men), prostate/bladder/cervical cancer, neurogenic bladder (diabetes, spinal cord disease)
-
Ureteral: Bilateral renal calculi, retroperitoneal fibrosis, endometriosis, metastatic colon cancer, lymphoma, papillary necrosis, blood clots
-
Tietz Textbook of Laboratory Medicine, 7th Edition; Goldman-Cecil Medicine; Brenner & Rector's The Kidney
4. Pathophysiology
Prerenal Pathophysiology
- Sympathetic activation and catecholamine release (norepinephrine) → afferent arteriolar constriction
- RAAS activation → Angiotensin II production → preferential efferent arteriolar constriction → initially preserves GFR via maintained glomerular hydrostatic pressure → also stimulates proximal tubular Na+/H+ exchangers to augment Na reabsorption
- ADH release → vasoconstriction, water retention, urea back-diffusion into the papillary interstitium
- Prostaglandins (PGE₂, PGI₂) counteract vasoconstriction - hence NSAIDs that block these worsen prerenal AKI
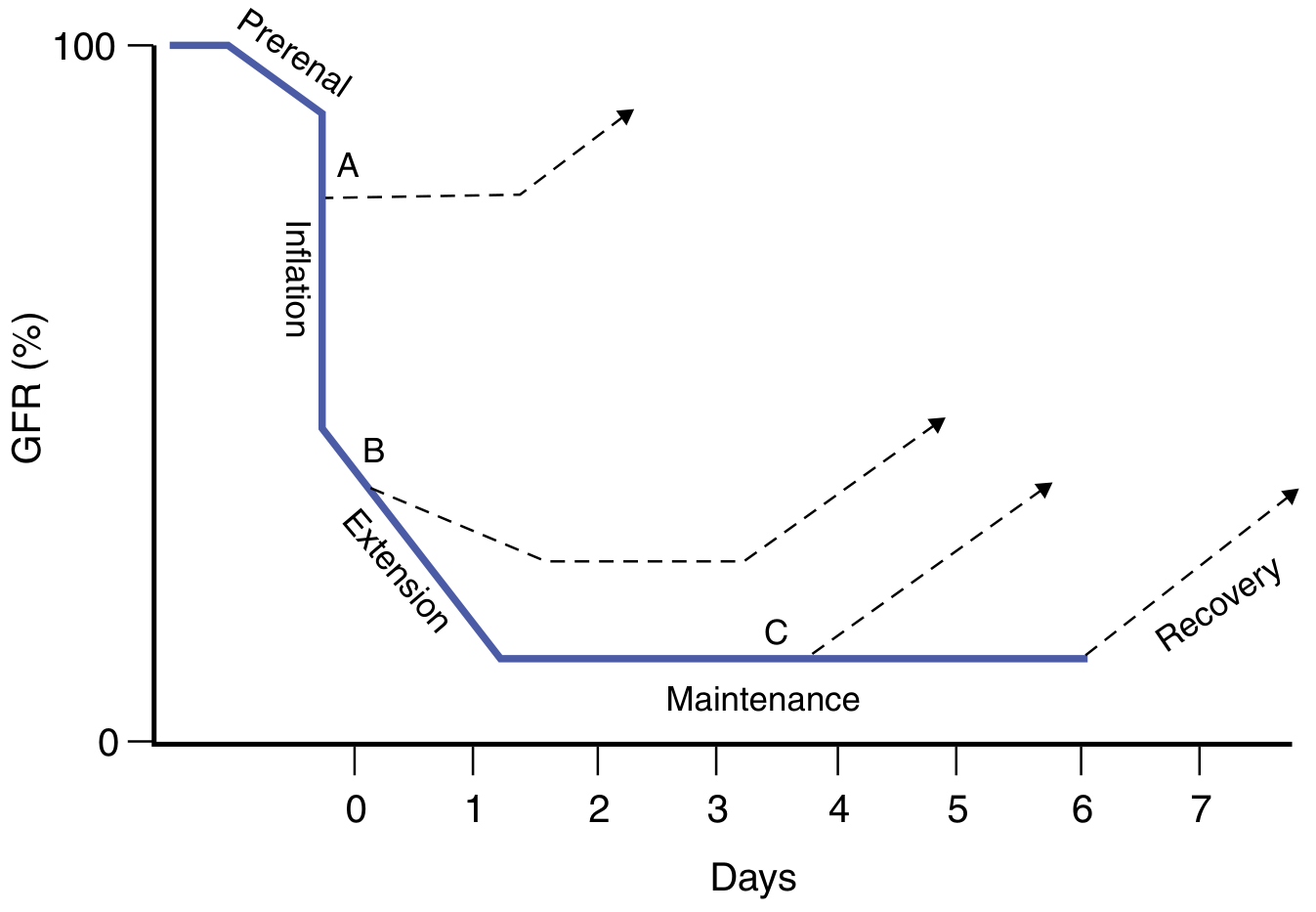
Intrinsic Renal Pathophysiology (ATN - Ischemic)
-
Initiation/Inflation phase (hours): Ischemia causes tubular epithelial injury, loss of brush border, cellular swelling, and loss of polarity. Sublytic injury disrupts cytoskeletal architecture - Na/K-ATPase loses its basolateral orientation, allowing back-leak of filtrate. ROS generation begins.
-
Extension phase: Continued microvascular ischemia especially in the outer medulla (S3 segment of proximal tubule is particularly vulnerable due to its high metabolic demand but low oxygen supply). Inflammatory mediators are activated - TNF-α, IL-10, CXCL1, neutrophil elastase. Endothelial dysfunction leads to coagulation and continued vasoconstriction. Cell death occurs via necrosis and apoptosis.
-
Maintenance phase (days to weeks): GFR stabilizes at a low level. Tubular obstruction by cellular debris (casts), back-leak of filtrate across denuded tubular epithelium, and intense vasoconstriction maintain reduced GFR.
-
Recovery phase: Tubular epithelial cell regeneration and redifferentiation. GFR gradually recovers over days to weeks.
Postrenal Pathophysiology
- Brenner and Rector's The Kidney, 2-Volume Set, pp. 906, 912
5. Diagnostic Approach
Clinical Presentation
- Often clinically silent in early stages
- Some patients note change in urine volume/color
- Obstructive AKI may cause hematuria and flank pain
- Advanced AKI: uremic symptoms (anorexia, fatigue, nausea/vomiting, pruritus, reversal of sleep-wake cycle)
- Examination: pulmonary/peripheral edema, pericardial/pleural friction rub, myoclonus, asterixis
Serum Labs
- Serum creatinine (serial measurements - single values are insufficient; influenced by muscle mass, medications)
- BUN/creatinine ratio: >20:1 suggests prerenal; <10-15:1 suggests intrinsic
- Electrolytes: Na+, K+, Cl-, HCO3-
- Calcium, phosphorus
- CBC with differential
- Serum uric acid (in tumor lysis syndrome context)
Urine Studies
Urinalysis and Microscopy
| Cause | Urinalysis Findings |
|---|---|
| Prerenal | Normal sediment or hyaline casts only |
| ATN | Muddy brown granular casts, renal tubular epithelial cells |
| AIN | WBC casts, eosinophils (eosinophiluria), mild proteinuria |
| Glomerulonephritis | RBC casts, dysmorphic RBCs, heavy proteinuria |
| Postrenal | May be normal, or hematuria if stone/tumor |
Fractional Excretion of Sodium (FENa)
| Value | Interpretation |
|---|---|
| <1% | Prerenal (tubules actively reabsorbing Na+) |
| >2% | Intrinsic ATN (tubular dysfunction, unable to reabsorb Na+) |
Renal Failure Index (RFI)
- RFI <1: Prerenal
- RFI >2: ATN
Novel Biomarkers
- NGAL (Neutrophil gelatinase-associated lipocalin): Elevated within 2 hours of tubular injury
- KIM-1 (Kidney Injury Molecule-1): Proximal tubule injury marker
- Cystatin C: Earlier indicator of GFR decline than creatinine
- IL-18: Marker of ischemic ATN
- TIMP-2 and IGFBP7 (urinary): Combined test (NephroCheck) for cell cycle arrest in tubular injury
- α1-microglobulin and urinary cystatin C: Predict need for RRT (AUC ~0.86)
Imaging
- Renal ultrasound (first-line): Assess kidney size, echogenicity, hydronephrosis (postrenal), blood flow (Doppler)
- Bladder catheterization: Simultaneous diagnostic and therapeutic for lower tract obstruction
- CT scan/MRI: Retroperitoneal causes, renal vasculature
- Renal biopsy: When cause of intrinsic AKI is unclear after non-invasive workup
Fluid Challenge
- Goldman-Cecil Medicine, pp. 1246-1247; Henry's Clinical Diagnosis and Management by Laboratory Methods; Roberts and Hedges' Clinical Procedures in Emergency Medicine
6. Management
General Principles
- Remove or treat the offending cause
- Optimize intravascular volume
- Avoid nephrotoxins
- Manage electrolyte and metabolic complications
- Initiate RRT when indicated
Prerenal AKI
- Prompt volume resuscitation: IV crystalloids (balanced crystalloids preferred over normal saline in critically ill patients - SMART trial evidence)
- Treat underlying cause (heart failure, cirrhosis, sepsis - these may not respond to fluids alone)
- Discontinue NSAIDs, ACE inhibitors, ARBs where possible
- For acute hypertension-related ARF: fenoldopam, nicardipine, or clevidipine (preserve renal blood flow while reducing SVR)
Intrinsic AKI (ATN)
- No specific therapy reverses established ATN
- Supportive care is the cornerstone
- Daily loop diuretics (furosemide 40-80 mg IV) for volume overload; note diuretics do not shorten ATN duration or prevent it
- Restrict sodium, potassium, and protein intake
- Hyperkalemia: Sodium zirconium cyclosilicate (Lokelma) or patiromer, low-K+ diet; in emergency - calcium gluconate, insulin/dextrose, sodium bicarbonate, kayexalate, dialysis
- Hyperphosphatemia: Oral phosphate binders
- Hypocalcemia: Calcium tablets
- Metabolic acidosis: Sodium bicarbonate tablets/infusion
Intrinsic AKI (Glomerulonephritis/Vasculitis)
- Immunosuppressive therapy: Prednisone (often 1 mg/kg/day with gradual taper over 1 month) for AIN and immune-mediated GN
- Cyclophosphamide + corticosteroids for ANCA vasculitis
- Plasmapheresis for Goodpasture disease
Postrenal AKI
- Urethral/bladder catheter for lower tract obstruction (both diagnostic and therapeutic)
- Ureteral stent or percutaneous nephrostomy for ureteral obstruction from tumor/stone
- Post-obstructive diuresis should be anticipated and managed with fluid replacement
7. Pharmacology in ARF Management
Diuretics
Loop Diuretics (Furosemide, Bumetanide, Torsemide, Ethacrynic acid)
- Mechanism: Block Na+/K+/2Cl- cotransporter (NKCC2) in the thick ascending limb of Henle (TAL) → increase urine flow and K+ excretion
- Use in ARF: Convert oliguric to non-oliguric ARF (facilitates fluid management); do NOT prevent or shorten duration of ARF; may worsen cast formation in myeloma/light-chain nephropathy
- Adverse effects: Hypokalemic metabolic alkalosis, ototoxicity (especially with aminoglycosides), hyperuricemia, hypomagnesemia, dehydration, allergic reactions (sulfonamide class - except ethacrynic acid)
Osmotic Diuretics (Mannitol)
- Mechanism: Freely filtered but not reabsorbed → osmotic water retention in proximal tubule and descending limb → water diuresis; also opposes ADH in collecting tubule
- Use: Flush nephrotoxins from tubules, reduce intracranial/intraocular pressure in concurrent injury
- Caution: Must be used carefully in renal insufficiency (can worsen fluid overload if not excreted)
K+-Sparing Diuretics (Spironolactone, Eplerenone, Triamterene, Amiloride)
- Generally avoided in ARF due to risk of severe, fatal hyperkalemia
- Triamterene + indomethacin specifically reported to cause ARF
- Triamterene may precipitate kidney stones
Vasopressors/Vasodilators
| Agent | Role in ARF |
|---|---|
| Norepinephrine | Septic shock - restore MAP and renal perfusion pressure |
| Vasopressin | Adjunct in septic shock; may reduce norepinephrine requirement |
| Fenoldopam | Selective DA1 agonist - reduces SVR while improving natriuresis and creatinine clearance in hypertensive emergencies with renal impairment |
| Dopamine (low dose) | No longer recommended for renal protection - landmark trials showed no benefit |
Electrolyte-Stabilizing Agents
| Agent | Indication | Mechanism |
|---|---|---|
| Sodium zirconium cyclosilicate (Lokelma) | Hyperkalemia | Traps K+ in GI tract via ion exchange |
| Patiromer | Hyperkalemia | Binds K+ in colon |
| Calcium gluconate | Emergency hyperkalemia | Membrane stabilization (cardiac protection) |
| Insulin + dextrose | Emergency hyperkalemia | Shifts K+ intracellularly |
| Sodium bicarbonate | Metabolic acidosis, emergency hyperkalemia | Alkalinization shifts K+ intracellularly; corrects acidosis |
| Calcium carbonate/phosphate binders | Hyperphosphatemia | Binds dietary phosphate in GI tract |
Nephroprotective Agents
| Agent | Context | Evidence |
|---|---|---|
| IV hydration before contrast | Contrast nephropathy prevention | Recommended (isotonic NaCl or NaHCO3) |
| N-Acetylcysteine | Contrast nephropathy prevention | Conflicting evidence (PRESERVE trial: no benefit over saline) |
| Niacinamide | Experimental for ischemic ATN (β-hydroxybutyrate pathway) | Investigational only |
| Statins | Periprocedural contrast nephropathy prevention | Some systematic review evidence |
Renal Replacement Therapy (RRT)
- Acidosis: Refractory metabolic acidosis
- Electrolytes: Refractory hyperkalemia
- Intoxication: Drug/toxin removal
- Overload: Refractory volume overload/pulmonary edema
- Uremia: Uremic symptoms (encephalopathy, pericarditis, myoclonus, asterixis, seizures, pleuritis)
-
Intermittent hemodialysis (IHD): Standard for hemodynamically stable patients
-
Continuous RRT (CRRT - CVVH, CVVHD, CVVHDF): Preferred for hemodynamically unstable ICU patients
-
Peritoneal dialysis: Alternative where vascular access is unavailable
-
Goldman-Cecil Medicine, p. 1247; Katzung's Basic and Clinical Pharmacology, 16th Edition, pp. 409-417
8. Prognosis
- About one-third of hospitalized patients with AKI have resolution within 24 hours, ~60% by 48 hours, ~70% by 72 hours
- Intrinsic AKI requiring dialysis carries high mortality (40-80% in ICU)
- Survivors of AKI have increased long-term risk of progressing to chronic kidney disease (CKD)
- Risk factors for non-recovery: pre-existing CKD, elderly age, sepsis, multiorgan failure, oliguria lasting >3 days
9. Prevention
- Identify high-risk patients (elderly, CKD, diabetics, heart failure, volume depletion)
- Limit nephrotoxin exposure (contrast, aminoglycosides, NSAIDs)
- Adequate IV hydration before contrast procedures
- Dose-adjust renally-cleared medications
- Avoid RAAS blockers + NSAIDs combination in volume-depleted patients
- Close monitoring of serum creatinine in patients receiving nephrotoxic drugs
- Goldman-Cecil Medicine, International Edition (pp. 1241-1248)
- Brenner and Rector's The Kidney, 2-Volume Set (pp. 906-912)
- Katzung's Basic and Clinical Pharmacology, 16th Edition (pp. 409-417)
- Tietz Textbook of Laboratory Medicine, 7th Edition (p. 1915)
- Henry's Clinical Diagnosis and Management by Laboratory Methods
- Tintinalli's Emergency Medicine: A Comprehensive Study
provide defenition, types, causes, pathophysiology, diagnostic approach , management along with pharmacology for CRF
"chronic kidney disease"[MeSH Terms] AND management
Chronic Renal Failure (CRF) / Chronic Kidney Disease (CKD)
Terminology note: "Chronic Renal Failure" (CRF) is now standardized as Chronic Kidney Disease (CKD) per KDIGO guidelines, reflecting the spectrum from mild kidney damage through complete kidney failure. CRF typically refers to advanced CKD (stages 4-5).
1. Definition
- A marker of kidney damage (e.g., albumin excretion ≥30 mg/day, urine sediment abnormalities, imaging abnormalities, pathologic abnormalities)
- OR a GFR <60 mL/min/1.73 m²
- Goldman-Cecil Medicine, International Edition, p. 1333
- Textbook of Family Medicine, 9th Edition
2. Classification / Staging (KDIGO)
GFR Stages
| Stage | Description | GFR (mL/min/1.73 m²) |
|---|---|---|
| G1 | Normal or high | ≥90 |
| G2 | Mildly decreased | 60-89 |
| G3a | Mildly to moderately decreased | 45-59 |
| G3b | Moderately to severely decreased | 30-44 |
| G4 | Severely decreased | 15-29 |
| G5 | Kidney failure | <15 |
Albuminuria Stages
| Stage | ACR (mg/g) | Description |
|---|---|---|
| A1 | <30 | Normal to mildly increased |
| A2 | 30-300 | Moderately increased (microalbuminuria) |
| A3 | >300 | Severely increased (macroalbuminuria/nephrotic range) |
- Goldman-Cecil Medicine, p. 1337
3. Causes
Glomerular Diseases
- Type 1 and Type 2 diabetes - progressive albuminuria → nephrosclerosis → GFR decline
- IgA nephropathy (most common glomerulonephritis worldwide)
- Focal segmental glomerulosclerosis (FSGS)
- Membranous nephropathy
- Lupus nephritis (SLE)
- ANCA-associated vasculitis
- Goodpasture disease
- Membranoproliferative GN
Vascular Diseases
- Hypertensive nephrosclerosis (second most common cause; most common nondiabetic cause)
- Renovascular disease / renal artery stenosis
- Thrombotic microangiopathies
- Cholesterol emboli / atheroembolism
- Sickle cell nephropathy
Tubulointerstitial Diseases
- Chronic pyelonephritis / reflux nephropathy
- Analgesic nephropathy (NSAIDs, phenacetin)
- Drug nephrotoxicity (long-term: cyclosporine, tacrolimus, lithium, aristolochic acid)
- Heavy metal toxicity (lead, cadmium)
- Sarcoidosis
- Chronic interstitial nephritis
Cystic and Congenital Diseases
- Autosomal dominant polycystic kidney disease (ADPKD) - GFR declines ~4.4-5.9 mL/min/year once renal function begins to fall
- Medullary cystic kidney disease
- Alport syndrome
- Congenital anomalies (hypoplasia, dysplasia)
Obstructive Uropathy (Postrenal)
- Benign prostatic hypertrophy
- Nephrolithiasis
- Retroperitoneal fibrosis
- Neurogenic bladder
- Posterior urethral valves (pediatric)
Other / Systemic
- Amyloidosis (AL, AA)
- Multiple myeloma / light-chain nephropathy
- Systemic infections (TB, hepatitis B/C, HIV - in developing countries)
- Environmental exposures (aristolochic acid in Balkans and Asia)
- Obesity-related CKD
- Goldman-Cecil Medicine, pp. 1335-1336; Tietz Textbook of Laboratory Medicine
4. Pathophysiology
The Intact Nephron Hypothesis / Hyperfiltration
Mechanisms of Progression
-
Proteinuria as a mediator of injury: Filtered proteins (especially albumin) are taken up by proximal tubular cells, causing tubular toxicity, interstitial inflammation, and fibrosis. This is the mechanism by which reducing proteinuria slows CKD progression.
-
RAAS over-activation: Angiotensin II drives efferent arteriolar vasoconstriction → elevated intraglomerular pressure → mechanical stress on glomerular basement membrane → podocyte injury and detachment.
-
Tubulo-interstitial fibrosis: TGF-β mediates epithelial-to-mesenchymal transition, myofibroblast activation, and excess extracellular matrix deposition → irreversible fibrosis.
-
Chronic hypoxia: Reduced peritubular capillary density and microvascular rarefaction → tubular ischemia → further injury.
-
Metabolic disturbances: Metabolic acidosis activates complement and promotes tubular injury; uremic toxins accumulate and drive inflammation.
Metabolic and Endocrine Consequences of Reduced GFR
| GFR Stage | Key Consequences |
|---|---|
| G3a-G3b | Anemia begins (↓ EPO), secondary hyperparathyroidism starts (↓ calcitriol, ↑ PTH, ↑ FGF-23) |
| G3b-G4 | Hyperkalemia, metabolic acidosis (↓ ammonia production), sexual dysfunction (elevated prolactin) |
| G4-G5 | Uremic neuropathy, pericarditis, bleeding diathesis, severe metabolic derangements |
| G5 (ESRD) | Full uremic syndrome: encephalopathy, pericarditis, platelet dysfunction, immune dysfunction |
- Erythropoietin deficiency (main mechanism)
- Hepcidin accumulation → functional iron deficiency (impaired iron mobilization)
- Shortened RBC survival in uremic milieu
- Bone marrow suppression by uremic toxins
Uremic Syndrome
- Indoxyl sulfate: cardiovascular and tubular toxin
- p-Cresyl sulfate: vascular injury
- TMAO, guanidines: neurologic toxicity
- Parathyroid hormone: pruritis, osteitis fibrosa, encephalopathy
- Brenner and Rector's The Kidney, pp. 2378
- Goldman-Cecil Medicine, pp. 1337-1340
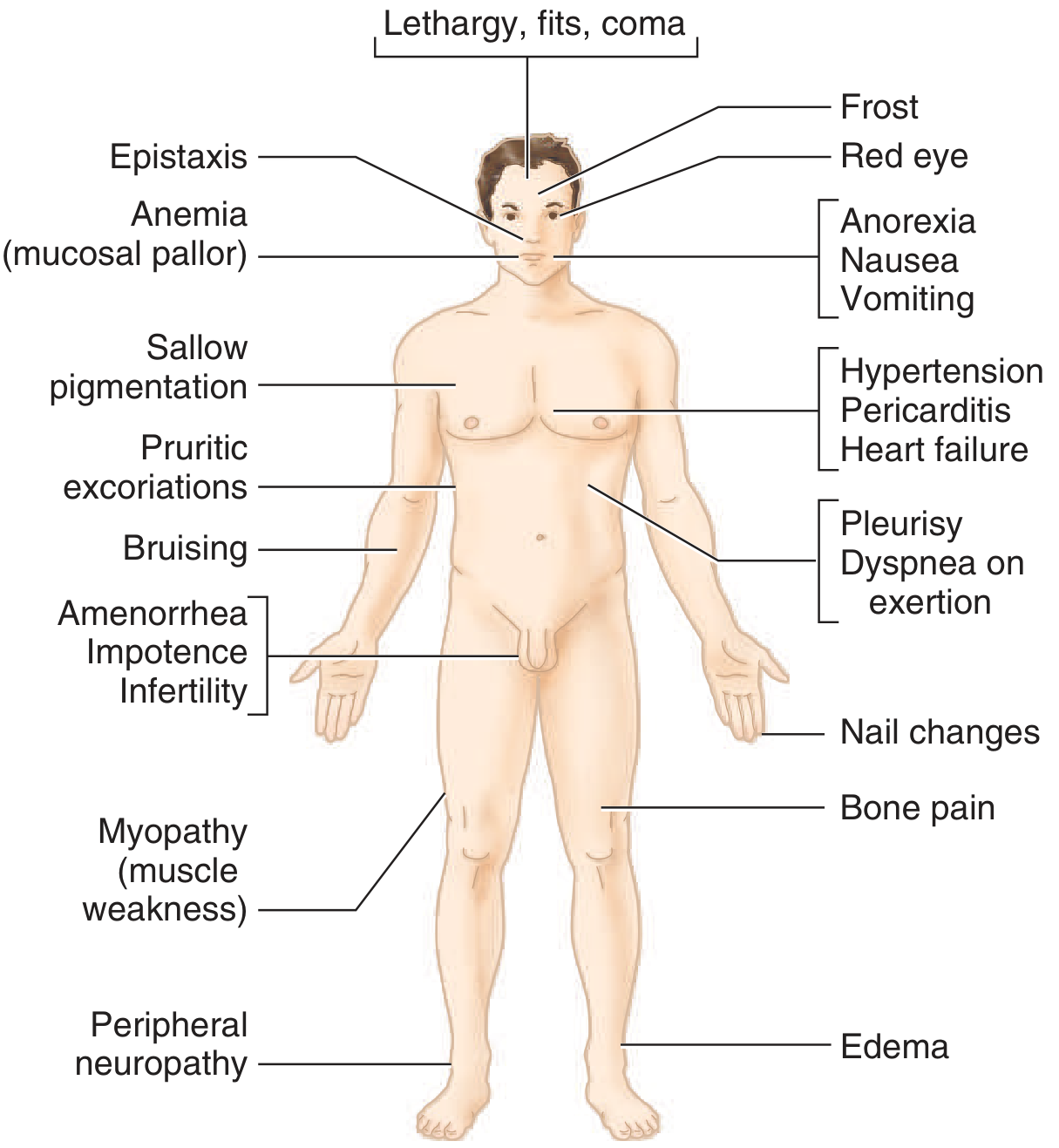
5. Clinical Manifestations
By System
| System | Manifestations |
|---|---|
| General | Fatigue, lassitude, anorexia, weight loss, sallow pigmentation |
| Neurological | Peripheral neuropathy (stocking-glove), uremic encephalopathy (lethargy, fits, coma), restless legs syndrome |
| Cardiovascular | Hypertension (early), pericarditis (uremic - late), heart failure, LV hypertrophy, accelerated atherosclerosis |
| Respiratory | Pleurisy, Kussmaul breathing (acidosis), pulmonary edema |
| GI | Anorexia, nausea, vomiting, uremic fetor, GI bleeding (platelet dysfunction), gastritis |
| Hematologic | Normochromic normocytic anemia (mucosal pallor), bleeding/bruising (platelet dysfunction), epistaxis |
| Dermatological | Pruritus, pruritic excoriations, uremic frost (late), nail changes (half-and-half nails), xerosis |
| Musculoskeletal | Bone pain, fractures (renal osteodystrophy), myopathy/muscle weakness |
| Endocrine/Reproductive | Amenorrhea, impotence, infertility (elevated prolactin), secondary hyperparathyroidism |
| Immunological | Increased susceptibility to infections, impaired vaccine response |
| Eyes | Red eye (conjunctival calcium deposits), hypertensive retinopathy |
| Fluid/Electrolytes | Edema, hyperkalemia, hyperphosphatemia, hypocalcemia, hyponatremia |
6. Diagnostic Approach
Criteria for CKD Diagnosis
- Albuminuria (ACR ≥30 mg/g)
- Urine sediment abnormalities
- Electrolyte abnormalities from tubular disorders
- Imaging abnormalities
- Pathologic abnormalities on biopsy
- History of kidney transplantation
- GFR <60 mL/min/1.73 m²
Step 1 - Establish Diagnosis and Stage
- CKD-EPI creatinine equation (2021, race-free): preferred initial test
- CKD-EPI cystatin C or combined creatinine + cystatin C: used as confirmatory tests; together more accurate than either alone
- Cockcroft-Gault: used for drug dosing
- Cystatin C is not affected by muscle mass or diet (but is affected by smoking, obesity, inflammation, thyroid disease, glucocorticoids)
- Spot urine albumin-to-creatinine ratio (UACR): recommended initial test (convenience, specificity)
- 24-hour urine albumin excretion rate: gold standard
- A1 (<30 mg/g), A2 (30-300 mg/g), A3 (>300 mg/g)
Step 2 - Evaluate Duration
- Review past records: prior creatinine values
- Indicators of chronicity: small echogenic kidneys on imaging, bilateral cortical thinning, chronic illness, polyuria/nocturia (loss of concentrating ability)
- Small kidneys (<9 cm) = chronic; normal or large kidneys may suggest infiltrative disease (amyloid, myeloma, polycystic kidneys, diabetic nephropathy)
Step 3 - Evaluate Markers of Kidney Damage
| Finding | Significance |
|---|---|
| RBC casts | Proliferative glomerulonephritis (GN) |
| WBC casts | Pyelonephritis or interstitial nephritis |
| Oval fat bodies/fatty casts | Heavy proteinuria (nephrotic syndrome) |
| Granular casts, RTECs | Non-specific parenchymal disease |
| Waxy/broad casts | Advanced CKD (late sign) |
- Renal ultrasound (first line): kidney size, echogenicity, cortical thickness, hydronephrosis, cysts, masses
- Small (<9 cm), echogenic kidneys = advanced CKD
- Enlarged kidneys: ADPKD, amyloid, myeloma, diabetic nephropathy
- Doppler ultrasound: renal artery stenosis
- CT/MRI: detailed anatomy, vascular, obstruction
- Nuclear scans (DMSA/MAG3): split renal function, scarring
Step 4 - Evaluate Cause
- Serum electrolytes, BUN, creatinine
- eGFR
- CBC (normochromic, normocytic anemia)
- Glucose, HbA1c (diabetic CKD)
- Lipid panel
- Serum calcium, phosphorus, PTH, alkaline phosphatase (CKD-MBD)
- 25-OH vitamin D
- Serum protein electrophoresis (SPEP), free light chains (myeloma)
- ANA, anti-dsDNA, ANCA, anti-GBM antibodies (autoimmune/vasculitis)
- Complement C3/C4
- Hepatitis B, C, HIV serology
- Protein excretion
- Creatinine clearance (if GFR estimation is uncertain)
- Cause is unclear after non-invasive workup
- Suspected treatable glomerulonephritis or vasculitis
- Unexpectedly rapid decline in GFR
- Disproportionate proteinuria
Monitoring
- Serum creatinine/eGFR: every 3-12 months depending on stage
- UACR: every 3-12 months
- Electrolytes, bicarbonate, calcium, phosphorus, PTH: every 3-6 months at G4-G5
- CBC: every 6-12 months (earlier if anemic)
- Refer to nephrology at GFR <30 (stage G4) or earlier if rapid decline, unexplained cause, or complex management
7. Management
- Treatment of the underlying cause
- Slowing disease progression
- Managing complications
- Preparing for renal replacement therapy
A. Treating Underlying Cause (Cause-Specific)
- Diabetic CKD: intensive glycemic control (HbA1c ~7%), BP control, RAAS blockade
- Hypertensive nephrosclerosis: BP target <130/80 mmHg
- Glomerulonephritis: immunosuppression (corticosteroids, cyclophosphamide, rituximab based on specific type)
- Obstruction: relieve surgically/endoscopically
- Drugs/toxins: stop offending agent
B. Slowing Progression (CGA Stage-Independent)
Blood Pressure Control
- Target: <130 mmHg systolic (regardless of CKD stage)
- First-line: ACE inhibitors or ARBs if proteinuria is present (reduce intraglomerular pressure and proteinuria independently of BP)
- Monitor serum K+ and creatinine after initiation
- A 10-30% rise in creatinine after starting RAAS blockade is acceptable and expected (efferent dilation reduces filtration pressure)
- Avoid combination ACE inhibitor + ARB (increased adverse effects without added benefit)
- Additional agents: calcium channel blockers, diuretics, beta-blockers as needed
SGLT2 Inhibitors - New Cornerstone of Therapy
- Empagliflozin, dapagliflozin, canagliflozin: Now recommended for CKD with or without Type 2 diabetes (at appropriate eGFR thresholds)
- Mechanism: Reduce intraglomerular pressure via tubuloglomerular feedback; reduce albuminuria; cardioprotective
- Evidence: DAPA-CKD trial - dapagliflozin reduced risk of ESKD, AKI, and death in CKD patients regardless of diabetes status
- "Cornerstone of therapy except in patients who have type 1 diabetes"
Reducing Proteinuria
- ACE inhibitors / ARBs: first-line
- SGLT2 inhibitors: additional antiproteinuric effect
- Finerenone (novel non-steroidal mineralocorticoid receptor antagonist): approved for diabetic CKD with albuminuria - reduces CKD progression and cardiovascular events
- GLP-1 agonists (e.g., semaglutide, liraglutide): in type 2 diabetes with albuminuria - additional option to slow CKD progression
Dietary Counseling
- Protein restriction: 0.6-0.8 g/kg/day in pre-dialysis CKD (may slow GFR decline; avoid in malnourished patients)
- Sodium restriction: <2 g/day (reduces BP, edema, and potentiates RAAS blockade)
- Potassium restriction: <2 g/day if hyperkalemia (K >5.5 mEq/L)
- Phosphate restriction: limit high-phosphate foods (dairy, processed foods, nuts)
C. Managing Complications
Metabolic Acidosis
- Sodium bicarbonate 650 mg twice daily, titrated to serum bicarbonate target ~22-24 mEq/L
- Slows CKD progression independently
- Risk: sodium load may worsen fluid retention/hypertension
Hyperkalemia
- Mild (K 5.0-5.5): dietary restriction (<2 g/day), avoid K-sparing drugs
- Moderate-severe (K >5.5): pharmacologic treatment
- Sodium zirconium cyclosilicate (Lokelma): fast-acting K+ binder; available for both acute and chronic management
- Patiromer (Veltassa): calcium-matched potassium binder; for chronic hyperkalemia maintenance
- Sodium polystyrene sulfonate (Kayexalate): older agent; less preferred
- Emergency: Calcium gluconate (cardiac membrane stabilization), insulin + dextrose (K+ shift), loop diuretics
Anemia (Anemia of CKD)
- Replete iron before/alongside ESA therapy
- Target ferritin 200-500 ng/mL and TSAT 20-40% in non-dialysis CKD
- Oral iron: ferrous sulfate 325 mg 2-3 times/day (often inadequate due to GI absorption impairment by hepcidin)
- IV iron (preferred in dialysis patients on ESAs): ferric carboxymaltose, iron sucrose, low-molecular-weight iron dextran
- Start when Hgb <9-10 g/dL with symptoms; generally reserved for G4-G5
- Target Hgb: avoid levels >11.5 g/dL (TREAT trial: higher targets increase stroke and thrombosis risk)
- Epoetin alfa: 50-100 units/kg SC 3 times/week; or 10,000-20,000 units every other week for non-dialysis patients. Average maintenance 75 units/kg 3×/week. SC preferred (20-40% dose savings)
- Darbepoetin alfa: 0.45 μg/kg IV or SC once weekly, or 0.75 μg/kg every 2 weeks. Longer half-life (3× longer than epoetin alfa)
- ESA resistance: suspect in patients who do not respond to 12-week escalation; causes include iron deficiency, infection/inflammation, occult bleeding, folate deficiency, carnitine deficiency, hyperparathyroidism, aluminum toxicity, inadequate dialysis
- Roxadustat, daprodustat: oral agents that stabilize HIF → stimulate endogenous EPO production; also reduce hepcidin
- Approved in some countries; under review in others
Mineral and Bone Disease (CKD-MBD)
-
Phosphate restriction: dietary + oral phosphate binders
- Calcium-based binders (calcium carbonate, calcium acetate): first-line; bind dietary phosphate in gut; avoid if Ca >10.2 mg/dL or PTH is suppressed (risk of vascular calcification)
- Non-calcium binders:
- Sevelamer hydrochloride/carbonate: also lowers LDL; safe in vascular calcification
- Lanthanum carbonate: chewed with meals
- Ferric citrate: also treats iron deficiency
- Sucroferric oxyhydroxide: iron-based binder
-
Active Vitamin D supplementation:
- Calcitriol (1,25-dihydroxyvitamin D): 0.25-0.5 μg orally daily or every other day, titrated to PTH/GFR
- Paricalcitol, doxercalciferol: vitamin D analogues; less hypercalcemia risk
- First correct 25-OH vitamin D deficiency with cholecalciferol/ergocalciferol before active vitamin D
-
Calcimimetics (dialysis patients with secondary hyperparathyroidism):
- Cinacalcet 30 mg orally daily (titrate to 60-90-120-180 mg) - allosteric activator of calcium-sensing receptor → suppresses PTH
- Etelcalcetide (IV, dialysis only)
-
Parathyroidectomy: for refractory tertiary hyperparathyroidism (subtotal or total + autotransplantation)
Cardiovascular Risk Reduction
- Statins: recommended to lower LDL and reduce cardiovascular events (similar benefit to non-CKD population, but start before dialysis; less clear benefit in dialysis)
- Blood pressure control: <130/80 mmHg
- Smoking cessation, physical activity, weight loss
- Aspirin: when indicated for cardiovascular disease; increased bleeding risk in CKD
Fluid and Edema Management
- Loop diuretics (furosemide): high doses often required due to impaired tubular secretion; can combine with thiazides for synergistic effect
- Salt restriction
D. Preparation for Renal Replacement Therapy (RRT)
- Nephrologist referral: GFR <30 (earlier if rapid decline, or complex management)
- Vascular access creation (AV fistula preferred over graft or catheter): 6-12 months before anticipated dialysis start
- Peritoneal dialysis catheter placement: 4-6 weeks before start
- Kidney transplant evaluation: should begin at GFR 20-25 to allow time for workup and listing
- Refractory hyperkalemia, acidosis, or fluid overload
- Uremic symptoms (encephalopathy, pericarditis, platelet dysfunction causing bleeding)
- GFR <10 regardless of symptoms (G5)
- GFR 10-15 with symptoms or nutritional failure
8. Pharmacology Summary
Renoprotective Agents
| Drug Class | Examples | Mechanism in CKD | Key Notes |
|---|---|---|---|
| ACE inhibitors | Enalapril, lisinopril, ramipril | ↓ Ang II → efferent dilation → ↓ intraglomerular pressure; ↓ proteinuria | Monitor K+, creatinine; contraindicated in pregnancy; avoid in bilateral RAS |
| ARBs | Losartan, valsartan, irbesartan | Same as ACE-I; better tolerated (no cough) | Same monitoring; evidence stronger for ARBs in type 2 diabetic nephropathy |
| SGLT2 inhibitors | Dapagliflozin, empagliflozin, canagliflozin | Tubuloglomerular feedback → ↓ intraglomerular pressure; natriuresis; anti-inflammatory; antiproteinuric | Work even at low GFR (≥20 for dapagliflozin); risk of DKA in T1DM; genital mycotic infections |
| GLP-1 agonists | Semaglutide, liraglutide | Weight loss, glycemic control, anti-inflammatory, ↓ albuminuria | Use in T2DM with CKD + obesity/CVD |
| Finerenone (MRA) | Finerenone | Non-steroidal MRA; ↓ fibrosis, ↓ proteinuria | Approved for T2DM + CKD with albuminuria; monitor K+ |
Anemia Agents
| Drug | Class | Dose | Notes |
|---|---|---|---|
| Epoetin alfa | ESA | 50-100 U/kg SC 3×/week | Target Hgb <11.5 g/dL; SC preferred over IV |
| Darbepoetin alfa | Long-acting ESA | 0.45 μg/kg SC/IV q1-4 wk | Less frequent dosing |
| Ferrous sulfate | Oral iron | 325 mg 2-3×/day | Often inadequate in advanced CKD |
| IV iron preparations | Parenteral iron | Ferric carboxymaltose, iron sucrose | Preferred in dialysis patients, when oral iron fails |
| Roxadustat | HIF-PHI | Oral | Stimulates endogenous EPO; approved in EU/Asia |
Bone and Mineral Agents
| Drug | Use | Key Points |
|---|---|---|
| Calcitriol (1,25-OH D) | Active vitamin D | 0.25-0.5 μg daily; suppresses PTH; risk of hypercalcemia/hyperphosphatemia |
| Paricalcitol | Vitamin D analogue | Less hypercalcemia risk than calcitriol |
| Calcium carbonate | Phosphate binder | With meals; avoid if Ca elevated or PTH suppressed |
| Sevelamer | Non-calcium phosphate binder | Also ↓ LDL; safe in vascular calcification |
| Lanthanum carbonate | Non-calcium phosphate binder | Chew with meals |
| Cinacalcet | Calcimimetic | 30-180 mg daily; suppresses PTH; nausea common; dialysis patients only |
| Etelcalcetide | IV Calcimimetic | IV at dialysis; more potent; nausea/hypocalcemia |
Hyperkalemia Agents
| Drug | Mechanism | Notes |
|---|---|---|
| Sodium zirconium cyclosilicate (Lokelma) | Traps K+ in GI tract (non-absorbed) | Rapid onset (within hours); both acute and chronic use |
| Patiromer (Veltassa) | Calcium-matched K+ exchanger in colon | Slower onset (7-48 hrs); chronic maintenance; administer 3 hrs away from other oral drugs |
| Sodium polystyrene sulfonate (Kayexalate) | Resin K+ exchanger | Older; risk of intestinal necrosis |
Cardiovascular/BP Agents Used in CKD
| Agent | Notes in CKD |
|---|---|
| Loop diuretics (furosemide) | High doses often needed; useful for volume/edema management |
| Statins | Reduce CV events; recommended at all CKD stages before dialysis |
| Calcium channel blockers | Amlodipine: no dose adjustment needed; safe in CKD |
| Beta-blockers | Carvedilol preferred; atenolol requires dose adjustment |
| NaHCO₃ | Treats acidosis; also slows CKD progression |
Renal Replacement Therapy Modalities
| Modality | Indication | Key Features |
|---|---|---|
| Intermittent hemodialysis (IHD) | Standard ESRD | 3-4 hrs, 3×/week; requires AV fistula/graft/catheter |
| Peritoneal dialysis (PD) | ESRD; home-based preference | CAPD or CCPD; preserves residual renal function longer |
| Kidney transplantation | Best long-term outcome | Living donor preferred; requires immunosuppression |
9. Prognosis
- CKD progression is measured by rate of GFR decline (slope of eGFR over time; normally ~1 mL/min/year after age 40)
- Risk of ESRD depends on stage, albuminuria, cause, and modifiable factors
- Patients with CKD have significantly increased risk of cardiovascular death compared to progression to ESRD - especially at G3-G4
- With optimal treatment (RAAS blockade, SGLT2 inhibitors, BP control), progression can be markedly slowed or halted
- AKI episodes accelerate CKD progression
- Goldman-Cecil Medicine, International Edition (pp. 1333-1347)
- Brenner and Rector's The Kidney, 2-Volume Set (pp. 2378)
- Textbook of Family Medicine, 9th Edition (pp. 1192)
- Goodman & Gilman's Pharmacological Basis of Therapeutics (pp. 922)
- Katzung's Basic and Clinical Pharmacology, 16th Edition
- Tietz Textbook of Laboratory Medicine, 7th Edition
provide defenition, types, causes, pathophysiology, diagnostic approach , management along with pharmacology for URAEMIA
"uremia"[MeSH Terms] AND management
provide defenition, types, causes, pathophysiology, diagnostic approach , management along with pharmacology for URAEMIA
Uraemia (Uremia)
1. Definition
- Acute uremia: AKI reaching GFR <10-15 mL/min with failure to recover
- Chronic uremia: Advanced CKD (Stage G5, GFR <15 mL/min/1.73 m²) - end-stage renal disease (ESRD)
- Acute-on-chronic uremia: Acute decompensation of established CKD
- Ganong's Review of Medical Physiology, 26th Edition, p. 692
- Harrison's Principles of Internal Medicine, 22nd Edition
- Brenner and Rector's The Kidney, 2-Volume Set
2. Types / Classification
A. By Temporal Pattern
| Type | Description |
|---|---|
| Acute uremia | Rapid-onset, from AKI (ischemic, toxic, or obstructive). Potentially reversible. |
| Chronic uremia | Progressive, irreversible. Develops over months-years in CKD stage G4-G5. |
| Acute-on-chronic uremia | Acute decompensation superimposed on CKD. Common precipitants: infection, dehydration, nephrotoxins, urinary tract obstruction. |
B. By Underlying Renal Pathology
| Category | Examples |
|---|---|
| Prerenal uremia | Severe hypoperfusion (heart failure, septic shock, dehydration) causing azotemia; may be pre-uremic |
| Intrinsic renal uremia | ATN, glomerulonephritis, interstitial nephritis, diabetic/hypertensive nephropathy |
| Postrenal/Obstructive uremia | Bilateral ureteral obstruction, bladder outlet obstruction (BPH, cancer) |
C. By Clinical Presentation (Severity)
- Pre-uremic state: Elevated BUN/creatinine, biochemical abnormalities, minimal or no symptoms
- Overt uremic syndrome: Full multi-system clinical syndrome with symptoms (GFR typically <10-15 mL/min)
- Uremic emergency: Life-threatening manifestations requiring emergency dialysis (uremic encephalopathy, pericarditis, uremic bleeding, severe hyperkalemia/acidosis)
3. Causes
Primary Renal Causes
- Diabetic nephropathy (most common worldwide)
- IgA nephropathy
- Focal segmental glomerulosclerosis (FSGS)
- Lupus nephritis, ANCA vasculitis, Goodpasture disease
- Membranous nephropathy
- Hypertensive nephrosclerosis (second most common)
- Renovascular disease/renal artery stenosis
- Thrombotic microangiopathies (TTP, HUS, aHUS)
- Cholesterol atheroembolism
- Chronic pyelonephritis / reflux nephropathy
- Analgesic nephropathy (NSAIDs, phenacetin)
- Chronic drug nephrotoxicity (cyclosporine, lithium, aristolochic acid)
- Heavy metal toxicity (lead, cadmium)
- Autosomal dominant polycystic kidney disease (ADPKD)
- Alport syndrome
- Ischemic ATN
- Toxic ATN (aminoglycosides, contrast, cisplatin, myoglobin, hemoglobin)
- Rapidly progressive glomerulonephritis
Systemic Causes Affecting the Kidney
- Amyloidosis (AL/AA)
- Multiple myeloma / light-chain nephropathy
- Systemic infections (hepatitis B/C, HIV, TB - in developing countries)
- Sarcoidosis
Obstructive/Postrenal
- Bilateral ureteral obstruction (stones, retroperitoneal fibrosis, tumor)
- Bladder outlet obstruction (BPH, prostate/bladder/cervical cancer)
- Neurogenic bladder
4. Pathophysiology
A. The Uremic Toxin Problem
Small-Molecule Uremic Toxins (<500 Da, water-soluble)
- Urea: Quantitatively the most abundant. BUN >180 mg/dL causes nausea, weakness, lethargy. At lower levels, serves more as a surrogate marker than a direct toxin.
- Creatinine: Not directly toxic even at very high concentrations; its metabolites methylguanidine (MG) and creatol are toxic
- Guanidines (guanidinosuccinic acid [GSA], methylguanidine): Derived from arginine. GSA inhibits platelets in vitro and stimulates nitric oxide generation → inhibits platelet adhesion. Guanidino compounds antagonize GABA receptors and are NMDA agonists → uremic encephalopathy and seizures
- Uric acid: Contributes to gout, vascular disease
- Phenols (phenol, p-cresol/p-cresyl sulfate): Disrupt cell membranes, impair immune cell function
- Oxalate: Contributes to soft tissue calcification
- Phosphate: Drives secondary hyperparathyroidism, vascular calcification, CKD-MBD
Middle Molecules (500 Da - 60 kDa)
- β2-Microglobulin (~11 kDa): Accumulates in long-term dialysis → deposits as amyloid fibrils in joints, carpal tunnel, bone (dialysis-related amyloidosis)
- Parathyroid hormone (PTH): Elevated in secondary hyperparathyroidism; contributes to encephalopathy (raises brain calcium), osteitis fibrosa cystica, pruritis
- FGF-23: Rises early; drives LV hypertrophy and cardiovascular risk
- Advanced glycosylation end products (AGEs): Vascular injury, inflammation
- Leptin, ghrelin, resistin: Adipokines elevated due to reduced renal clearance → insulin resistance, appetite dysregulation
Protein-Bound Solutes
- Indoxyl sulfate: Derived from intestinal tryptophan metabolism; cardiovascular toxin, promotes tubular fibrosis
- p-Cresyl sulfate: Endothelial toxicity, inflammation
- Asymmetric dimethylarginine (ADMA): Inhibits endothelial NO synthase → endothelial dysfunction, hypertension, accelerated cardiovascular disease; levels correlate with cerebrovascular complications
Low-Molecular-Weight Proteins Accumulating in Uremia
B. Loss of Renal Synthetic/Endocrine Functions
| Lost Function | Consequence |
|---|---|
| ↓ Erythropoietin | Normochromic, normocytic anemia (hypoproliferative) |
| ↓ 1,25-dihydroxyvitamin D (calcitriol) | Hypocalcemia → ↑PTH → secondary hyperparathyroidism → renal osteodystrophy |
| ↓ Ammoniagenesis | Metabolic acidosis (type B uremic acidosis - decreased production, not secretion) |
| ↓ Urine-concentrating ability | Isosthenuria, polyuria/nocturia early; oliguria/anuria late |
| ↓ Acid excretion | Anion gap metabolic acidosis (retained sulfates, phosphates, urate at G4-G5) |
C. Pathophysiology of Key Uremic Manifestations
- Brenner and Rector's The Kidney, pp. 2368-2380
- Comprehensive Clinical Nephrology, 7th Edition, pp. 1197-1198
5. Clinical Manifestations
Symptoms and Signs by System
Neurological (Uremic Encephalopathy)
- Mood swings, depression, anxiety
- Impaired concentration, loss of recent memory
- Insomnia, fatigue, apathy
- Hyperreflexia, tremor
- Asterixis (negative myoclonus - intermittent loss of muscle tone in anti-gravity muscles; elicited with outstretched hands, protruded tongue, or raised index finger)
- Myoclonus (activation of anti-gravity muscles, millisecond duration)
- Restless legs syndrome
- Sleep disturbances, altered sleep-wake cycle
- Peripheral neuropathy (stocking-glove distribution; dying-back axonal neuropathy)
- Delirium, psychosis
- Generalized seizures
- Coma → death if untreated
Cardiovascular
- Hypertension (most common; due to fluid retention and RAAS activation)
- Uremic pericarditis: chest pain (pleuritic character), pericardial friction rub; may progress to pericardial effusion or tamponade
- Heart failure / pulmonary edema (from fluid overload and hypertensive cardiomyopathy)
- LV hypertrophy (from hypertension and FGF-23)
- Accelerated atherosclerosis (coronary artery disease, stroke, PVD)
- Arrhythmias (from hyperkalemia)
Respiratory
- Pleurisy / uremic pleuritis: fibrinous pleuritis, exudative pleural effusion
- Kussmaul breathing: deep sighing respiration from metabolic acidosis
- Pulmonary edema (from fluid overload)
- "Uremic lung" (pulmonary edema from increased permeability, butterfly pattern on CXR)
Gastrointestinal
- Anorexia (earliest and most consistent GI symptom)
- Nausea, vomiting
- Uremic fetor: ammoniacal or urine-like breath odor (from urea converted to ammonia by salivary urease)
- Gastritis, peptic ulceration (increased gastrin production)
- GI bleeding (from platelet dysfunction, mucosal fragility)
- Diarrhea, constipation
- Hiccups (diaphragm irritation)
Hematological
- Normochromic, normocytic anemia (from EPO deficiency + shortened RBC survival + hepcidin-mediated iron sequestration)
- Platelet dysfunction (qualitative defect): prolonged bleeding time, bruising, epistaxis, gum bleeding, GI bleeding, menorrhagia. PT, aPTT, and platelet COUNT are usually normal.
- Shortened erythrocyte lifespan (from uremic toxin-induced membrane fragility)
- Lymphocyte and granulocyte dysfunction (impaired immune response, increased infection susceptibility)
- Thrombocytopenia may occur from dialysis membrane activation
Dermatological
- Pruritus (most distressing symptom; from phosphate deposition in skin, secondary hyperparathyroidism, mast cell proliferation, peripheral neuropathy)
- Uremic frost: white-yellow crystalline deposits on skin (urea crystallizing from sweat); seen in very severe uremia
- Sallow/yellow-grey pigmentation (from urochrome accumulation and anemia)
- Pruritic excoriations, dry skin (xerosis)
- Nail changes: half-and-half nails (Lindsay's nails) - proximal white, distal brown/pink band
- Pallor (anemia)
- Bruising, petechiae (from platelet dysfunction)
Musculoskeletal
- Renal osteodystrophy (umbrella term for CKD-MBD): bone pain, fractures
- Osteitis fibrosa cystica: from high PTH → osteoclastic resorption
- Osteomalacia: from calcitriol deficiency → defective bone mineralization
- Adynamic bone disease: low PTH (from over-suppression) → low turnover
- Osteoporosis: multifactorial
- Calciphylaxis (calcific uremic arteriolopathy): calcification of small arteries → ischemic skin necrosis; severe pain
- Dialysis-related amyloidosis: β2-microglobulin deposits → carpal tunnel syndrome, destructive arthropathy (in long-term dialysis patients)
- Myopathy, muscle weakness
- Muscle cramps (from electrolyte disturbances)
Endocrine/Metabolic
- Insulin resistance (glucose intolerance without overt diabetes)
- Dyslipidemia: hypertriglyceridemia (from impaired lipoprotein lipase)
- Secondary hyperparathyroidism (↓ calcitriol → ↑ PTH)
- Elevated prolactin → gonadal dysfunction: amenorrhea, impotence, infertility
- Altered thyroid metabolism
- Altered thyroxine metabolism (euthyroid sick-like picture)
Electrolyte/Acid-Base
- Hyperkalemia: life-threatening arrhythmias
- Metabolic acidosis: anion gap type (↑ sulfates, phosphates, urate) at advanced stages
- Hyperphosphatemia: secondary hyperparathyroidism, vascular calcification
- Hypocalcemia: from calcitriol deficiency and phosphate retention
- Sodium abnormalities: hypo- or hypernatremia depending on water balance
- Fluid overload: edema, pulmonary edema, hypertension
6. Diagnostic Approach
Confirming Uremia
- Symptoms: anorexia, nausea/vomiting, fatigue, pruritus, edema, oliguria, confusion, restless legs
- History of CKD, diabetes, hypertension, nephrotoxin exposure
- Drug history (nephrotoxic medications)
- Family history (ADPKD, Alport syndrome)
- Pallor, sallow complexion, uremic frost (late)
- Pruritic excoriations, half-and-half nails
- Asterixis, altered consciousness, seizures
- Pericardial friction rub
- Kussmaul breathing
- Peripheral edema, pulmonary edema signs (raised JVP, crepitations)
- Peripheral neuropathy signs
Laboratory Investigations
| Test | Finding in Uremia |
|---|---|
| Serum creatinine + BUN | Markedly elevated; BUN:Cr ratio ~10:1 (intrinsic) or >20:1 (prerenal) |
| eGFR | <15 mL/min/1.73 m² in ESRD |
| Serum electrolytes | Hyperkalemia, hyponatremia, elevated anion gap |
| Serum bicarbonate | Low (12-18 mEq/L; anion gap metabolic acidosis) |
| Serum calcium | Low (hypocalcemia) |
| Serum phosphorus | High (hyperphosphatemia) |
| PTH (intact/iPTH) | High (secondary hyperparathyroidism) |
| CBC | Normochromic normocytic anemia; normal platelet count; prolonged bleeding time |
| Serum albumin | Low (from protein-energy wasting and inflammation) |
| Serum uric acid | Elevated |
| Blood glucose / HbA1c | Elevated in diabetic nephropathy (HbA1c may be falsely low due to shortened RBC lifespan) |
| Urinalysis + microscopy | Proteinuria; waxy/broad casts (highly specific for advanced CKD); RBC casts (GN); WBC casts (interstitial nephritis) |
| Urine ACR/PCR | Elevated in glomerular disease |
| LFTs | May be abnormal; hepatorenal involvement |
| Coagulation screen | PT/aPTT usually normal; bleeding time prolonged |
- HbA1c, fasting glucose: diabetic nephropathy
- ANA, anti-dsDNA, ANCA, anti-GBM: autoimmune/vasculitis
- SPEP, UPEP, free light chains: myeloma
- Complement C3/C4: lupus, MPGN
- Hepatitis B/C, HIV serology
- 25-OH vitamin D + 1,25-OH vitamin D: bone disease
- Renal ultrasound (essential): kidney size (small + echogenic = CKD; large = acute or infiltrative disease), cortical thickness, hydronephrosis (postrenal), cysts (ADPKD)
- CXR: cardiomegaly, pulmonary edema, "bat-wing" perihilar edema, pleural effusion, pericardial effusion
- ECG: peaked T waves, wide QRS, sine wave pattern (hyperkalemia); low-voltage/electrical alternans (pericardial effusion)
- Echocardiography: LV hypertrophy, pericardial effusion, wall motion abnormalities
7. Management
A. Treat Underlying Cause
- Remove nephrotoxins / offending drugs
- Aggressive blood pressure control (target <130/80 mmHg)
- Glycemic control in diabetic CKD
- Immunosuppression for GN/vasculitis
- Relieve obstruction (catheter, nephrostomy, stent)
- Volume resuscitation for prerenal component
B. Conservative Management of Uremic Complications
- Protein restriction: 0.6-0.8 g/kg/day (reduces nitrogenous waste generation and delays dialysis need; avoid in malnourished patients)
- Sodium restriction: <2 g/day
- Potassium restriction: <2 g/day if hyperkalemia
- Phosphate restriction: avoid high-phosphate foods (dairy, processed meats, nuts, cola)
- Adequate caloric intake: 30-35 kcal/kg/day to prevent catabolism
- Fluid restriction: if oliguric
- Dietary restriction
- Sodium zirconium cyclosilicate (Lokelma) or patiromer for chronic management
- Emergency: calcium gluconate IV (cardiac membrane stabilization), insulin + dextrose (10 U + 50 mL 50% dextrose IV), sodium bicarbonate, loop diuretics
- Dialysis if refractory
- Sodium bicarbonate 650 mg orally twice daily, titrated to serum bicarbonate target 22-24 mEq/L
- Slows CKD progression as well as treating acidosis
- Calcium carbonate (phosphate binder) also provides alkali
- Dietary phosphate restriction
- Phosphate binders (calcium carbonate, sevelamer, lanthanum carbonate)
- Active vitamin D (calcitriol 0.25-0.5 μg/day)
- Calcimimetics (cinacalcet) for dialysis patients with secondary hyperparathyroidism
- Parathyroidectomy for tertiary hyperparathyroidism refractory to medical treatment
- Adequate dialysis dose
- Control of hyperphosphatemia/hyperparathyroidism
- Topical emollients, topical capsaicin
- Gabapentin (use with caution due to accumulation in renal failure)
- Naltrexone (opioid antagonist) or nalfurafine (κ-opioid agonist - approved in some countries)
- UVB phototherapy
- Antihistamines (limited evidence)
- Initiate/optimize dialysis (primary treatment)
- Treat hyperkalemia, acidosis, hyponatremia
- Avoid/dose-adjust neurotoxic drugs (meperidine, gabapentin, metoclopramide, acyclovir, certain antibiotics)
- Seizure management with appropriate AEDs (phenobarbital, levetiracetam preferred; phenytoin absorption altered in uremia)
- Dialysis reverses encephalopathy in most patients
C. Uremic Bleeding (Pharmacological Management)
| Agent | Mechanism | Dose / Route | Onset | Duration |
|---|---|---|---|---|
| Desmopressin (DDAVP) | Releases vWF from endothelial cells → enhances platelet adhesion and aggregation | 0.3 μg/kg IV or SC | 1 hour | ≥4 hours |
| Cryoprecipitate | Provides vWF, fibrinogen, factor VIII, factor XIII | 10 units IV over 30 minutes | 4 hours | 24-36 hours |
| Conjugated estrogens | Reduce NO production → decrease platelet inhibition; long-term platelet correction | 0.5-0.6 mg/kg/day IV for 5 days (or 50 mg/day oral for 7 days) | 6 hours | 2 weeks |
| RBC transfusion / Erythropoietin | Correct anemia → improve platelet-vessel wall rheology; correction of Hct to >30% shortens bleeding time | Target Hgb >10 g/dL | Hours-days | Sustained |
| Hemodialysis | Removes guanidinosuccinic acid and other platelet-inhibiting toxins | Standard HD session | Hours | Partial correction only |
| Platelet transfusion | Infused platelets quickly acquire the uremic defect - generally ineffective alone | Only as part of multi-modal Rx for life-threatening bleeding | Immediate | Short (hours) |
D. Cardiovascular Management
- Antihypertensives: RAAS blockade (ACEi/ARB) as first-line; additional agents as needed
- Diuretics: Loop diuretics (furosemide, high doses often required) for volume control/edema
- Uremic pericarditis: Intensify dialysis (primary treatment); NSAIDs/corticosteroids if dialysis inadequate; pericardiocentesis for tamponade; pericardiectomy for constrictive pericarditis
- Statins: Reduce cardiovascular mortality (in pre-dialysis CKD; less clear benefit in dialysis)
E. Anemia Management
- Erythropoiesis-stimulating agents (ESAs): Epoetin alfa 50-100 U/kg SC 3×/week or darbepoetin alfa 0.45 μg/kg once weekly; target Hgb 10-11.5 g/dL (avoid >11.5 g/dL due to thrombosis/stroke risk)
- Iron supplementation: Iron repletion before/with ESAs; IV iron preferred in dialysis patients (ferric carboxymaltose, iron sucrose)
- HIF-PHIs (roxadustat, daprodustat): Oral agents stimulating endogenous EPO synthesis; approved in EU/Asia/Japan
8. Pharmacology Summary
Renal Replacement Therapy (RRT) - Definitive Treatment
- Acidosis: pH <7.1 or refractory metabolic acidosis
- Electrolytes: Refractory hyperkalemia (K+ >6.5 mEq/L or with ECG changes)
- Intoxication: Toxin removal (methanol, ethylene glycol, salicylates, metformin, lithium, barbiturates, valproate in overdose)
- Overload: Refractory pulmonary edema/volume overload
- Uremia: Uremic encephalopathy (asterixis, seizures, coma), uremic pericarditis, uremic bleeding unresponsive to medical management, BUN >100 mg/dL without clinical recovery
| Modality | Principle | Solutes Cleared | Best For |
|---|---|---|---|
| Intermittent Hemodialysis (IHD) | Diffusive + convective across semipermeable membrane | Small molecules best; 3-4 hrs, 3-4×/week | Hemodynamically stable patients |
| CRRT (CVVH, CVVHD, CVVHDF) | Continuous; convective (CVVH), diffusive (CVVHD), or both (CVVHDF) | Small + middle molecules | Hemodynamically unstable ICU patients; cerebral edema |
| SLED / Extended Daily Dialysis (EDD) | Hybrid; lower blood and dialysate flows, 8-12 hrs | Small + some middle molecules | Intermediate hemodynamic instability |
| Peritoneal Dialysis (PD) | Diffusion across peritoneal membrane | Small + middle molecules (better than IHD); protein-bound less well | Home setting; residual renal function preserved longer; pediatrics |
| Kidney Transplantation | Restore complete kidney function | All uremic solutes + synthetic functions | Best long-term outcome; reverses nearly all uremic manifestations |
- Kt/V urea ≥1.4 per session (IHD) - measures urea clearance per session
- Inadequate dialysis → persistent uremic symptoms (anorexia, malaise, pericarditis, fluid overload)
Key Drug Dosing Adjustments in Uremia
| Drug | Concern in Uremia | Action Required |
|---|---|---|
| Aminoglycosides | Accumulate → ototoxicity, nephrotoxicity | Extend dosing interval; monitor levels |
| Vancomycin | Accumulates | Extend interval; monitor trough/AUC |
| Digoxin | Narrow TI; accumulates | Reduce dose; monitor levels |
| Metformin | Lactic acidosis risk | Contraindicated if eGFR <30 |
| NSAIDs | Worsen renal function; impair platelet function | Avoid |
| ACE inhibitors / ARBs | Hyperkalemia, ↑ creatinine | Use with caution; monitor K+ |
| LMWH (enoxaparin) | Unpredictable pharmacokinetics in severe AKI | Avoid if possible; use UFH |
| Meperidine (pethidine) | Normeperidine accumulates → seizures | Avoid |
| Gabapentin | Accumulates → myoclonus, sedation | Dose reduce significantly |
| Acyclovir | Neurotoxic metabolite accumulates | Dose reduce; adequate hydration |
| Contrast agents | Contrast nephropathy | Pre-hydration; minimize dose |
| Opioids | Active metabolites accumulate | Use with caution; fentanyl preferred |
9. Prognosis
- Acute uremia from AKI: Prognosis depends on severity of underlying cause and timeliness of treatment. Many cases are reversible with appropriate management.
- Chronic uremia (ESRD): Without RRT, chronic uremia is fatal, typically within weeks to months.
- With hemodialysis: 5-year survival rates ~40-50% (varies widely with age, diabetes, cardiovascular status)
- With kidney transplantation: Best outcomes; 5-year graft survival ~80%; life expectancy near-normal in young recipients
- Quality of life consistently improves with transplantation versus dialysis
- Cardiovascular disease is the leading cause of death in ESRD patients on dialysis (~50% of deaths)
- Brenner and Rector's The Kidney, 2-Volume Set (pp. 2368-2382)
- Comprehensive Clinical Nephrology, 7th Edition (pp. 1197-1198)
- Harrison's Principles of Internal Medicine, 22nd Edition
- Ganong's Review of Medical Physiology, 26th Edition (p. 692)
- Henry's Clinical Diagnosis and Management by Laboratory Methods (p. 976)
- Tintinalli's Emergency Medicine: A Comprehensive Study (p. 760-761)
- The Washington Manual of Medical Therapeutics (pp. 1132-1145)
- Goldman-Cecil Medicine, International Edition
provide defenition, types, causes, pathophysiology, diagnostic approach , management along with pharmacology for BPH and provide defenition, types, causes, pathophysiology, diagnostic approach , management along with pharmacology for impotence
PART 1: Benign Prostatic Hyperplasia (BPH)
1. Definition
- Goldman-Cecil Medicine, International Edition, p. 1316
- Sabiston Textbook of Surgery, p. 2824
- Robbins & Kumar Basic Pathology
2. Types / Classification
By Symptom Type (LUTS Classification)
| Category | Symptoms |
|---|---|
| Storage (irritative) symptoms | Urinary frequency, urgency, urge incontinence, nocturia |
| Voiding (obstructive) symptoms | Hesitancy, poor/intermittent stream, straining to void, prolonged voiding, incomplete emptying |
| Post-void symptoms | Post-void dribbling, sensation of incomplete bladder emptying |
By Severity (International Prostate Symptom Score - IPSS)
| Score | Severity |
|---|---|
| 0-7 | Mild |
| 8-19 | Moderate |
| 20-35 | Severe |
By Tissue Composition (Histological)
- Stromal-predominant BPH (fibromuscular): responds better to alpha-blockers (smooth muscle relaxation)
- Glandular-predominant BPH: responds better to 5α-reductase inhibitors
- Mixed stromal-glandular BPH: combination therapy most effective
By Complication Status
- Uncomplicated BPH: LUTS without complications
- Complicated BPH: with urinary retention, UTI, bladder stones, hydronephrosis/azotemia, hematuria
3. Causes and Risk Factors
Primary Cause
- Functioning testes (BPH does not occur in men castrated before puberty)
- Androgens (BPH does not develop with genetic diseases that block androgen activity)
- Age (the only non-modifiable risk factor)
Hormonal Pathogenesis
- Dihydrotestosterone (DHT): the ultimate prostatic growth mediator; 10× more potent than testosterone. Synthesized from testosterone in the prostate by 5α-reductase type 2.
- Estrogen effect: With aging, testosterone declines while estrogen remains unchanged or increases (via peripheral aromatization). Estrogens act synergistically with DHT to drive growth of epithelial and stromal cells (which express estrogen receptors).
Risk Factors
| Factor | Role |
|---|---|
| Age | #1 risk factor; 50% prevalence in men >50 yr; 90% in men >80 yr |
| Family history | Genetic predisposition, particularly for early-onset BPH |
| Race | Higher in Black men; lower in Asian men |
| Obesity/Metabolic syndrome | Higher insulin → ↑ IGF-1 → prostatic growth; higher estrogen from adipose conversion |
| Physical inactivity | Associated with higher LUTS severity |
| Diet | High-fat diet; red meat; low vegetable intake |
4. Pathophysiology
Molecular Mechanism of Prostatic Growth
- Testosterone enters prostatic stromal and epithelial cells
- 5α-reductase type 2 converts testosterone → DHT (10× more potent)
- DHT binds nuclear androgen receptors (ARs) → activates gene expression
- DHT-induced growth factors (e.g., EGF, KGF/FGF-7, IGF-1, TGF-β):
- Increase stromal cell proliferation
- Decrease epithelial cell apoptosis (shift in proliferation-apoptosis equilibrium)
- With aging: ↓ testosterone, unchanged/↑ estrogen → estrogen synergizes with DHT via AR upregulation → continued growth
Anatomical Consequences
Mechanisms of LUTS
- Enlarged prostate mass compresses urethra → increased urethral resistance → ↓ urine flow → bladder hypertrophy (detrusor muscle thickening)
- Sympathetic α1-adrenergic receptors (especially α1A subtype) in prostatic stroma and bladder neck → smooth muscle contraction → functional obstruction
- This component is reversible and the target of α-blocker therapy
- Chronically elevated intravesical pressure → bladder wall hypertrophy → trabeculation → diverticula
- Overactive bladder (OAB): Bladder hypertrophy leads to increased detrusor instability → urgency, frequency, nocturia
- Incomplete emptying → post-void residual urine → increased UTI risk
- With long-standing obstruction: bladder decompensation → hypotonicity, chronic retention, overflow incontinence, hydronephrosis
Complications of Untreated BPH
-
Acute urinary retention (AUR): sudden inability to void; precipitated by sympathomimetics (cold remedies), anticholinergics, postponing micturition
-
Chronic urinary retention: painless high-volume retention; risk of renal failure
-
UTI / cystitis: residual urine provides bacterial culture medium
-
Bladder calculi: from stasis, infection, altered urine composition
-
Hematuria: from increased prostatic vascularity; can be gross
-
Hydronephrosis and CKD/azotemia: from obstructive uropathy
-
Robbins & Kumar Basic Pathology, p. 659
-
Campbell Walsh Wein Urology
5. Diagnostic Approach
History
- Document LUTS type (storage vs. voiding vs. post-void)
- IPSS questionnaire: quantify symptom severity; includes QoL question
- Duration of symptoms, rate of progression
- Medication history (alpha-stimulants, anticholinergics, diuretics - can worsen LUTS)
- Sexual function history (BPH/LUTS commonly co-exist with ED)
- Prior urological history (catheterization, STDs, urethral stricture)
- Medical history (neurologic disease, diabetes - can cause similar LUTS)
Physical Examination
- Digital Rectal Examination (DRE): Size (normal ~20 mL = size of walnut); consistency (BPH = soft/rubbery, uniform; cancer = hard/nodular); median sulcus (present in BPH, absent in cancer)
- Focused neurological exam: exclude neurogenic bladder (tone, perianal sensation, bulbocavernosus reflex)
- Abdominal palpation: palpable bladder (retention), flank tenderness (hydronephrosis/UTI)
Laboratory Tests
| Test | Purpose |
|---|---|
| Urinalysis + MSU culture | Exclude UTI, hematuria, glucosuria (diabetic neuropathy) |
| Serum PSA | Screen for prostate cancer (should be offered to men with >10 yr life expectancy); note: BPH elevates PSA (use free:total PSA ratio and PSA density to distinguish from cancer) |
| Serum creatinine / BUN | Assess for obstructive nephropathy/azotemia |
| Blood glucose | Exclude diabetic cystopathy |
| Serum testosterone | If hypogonadism suspected |
Urological Investigations
| Investigation | Purpose |
|---|---|
| Post-void residual (PVR) urine | Ultrasound or catheter; >300 mL = significant retention; correlates with bladder decompensation |
| Uroflowmetry | Non-invasive; Qmax <10 mL/sec = significant obstruction; Qmax 10-15 = borderline; >15 = likely normal |
| Transrectal Ultrasound (TRUS) | Accurate prostate volume measurement; guides biopsy if cancer suspected |
| Renal/Bladder Ultrasound | Kidneys (hydronephrosis), bladder wall thickness, PVR, bladder stones |
| Cystoscopy | Visualize urethra, prostate, bladder; identify stricture, bladder neck obstruction, stones, tumors; guides surgical planning |
| Urodynamic studies | Differentiate BOO from detrusor underactivity; indicated when diagnosis uncertain or before surgery |
| Intravenous Urography (IVU) | Now largely replaced by ultrasound; used if upper tract involvement suspected |
| Frequency volume chart | Documents fluid intake, voiding times, volumes; especially useful for nocturia |
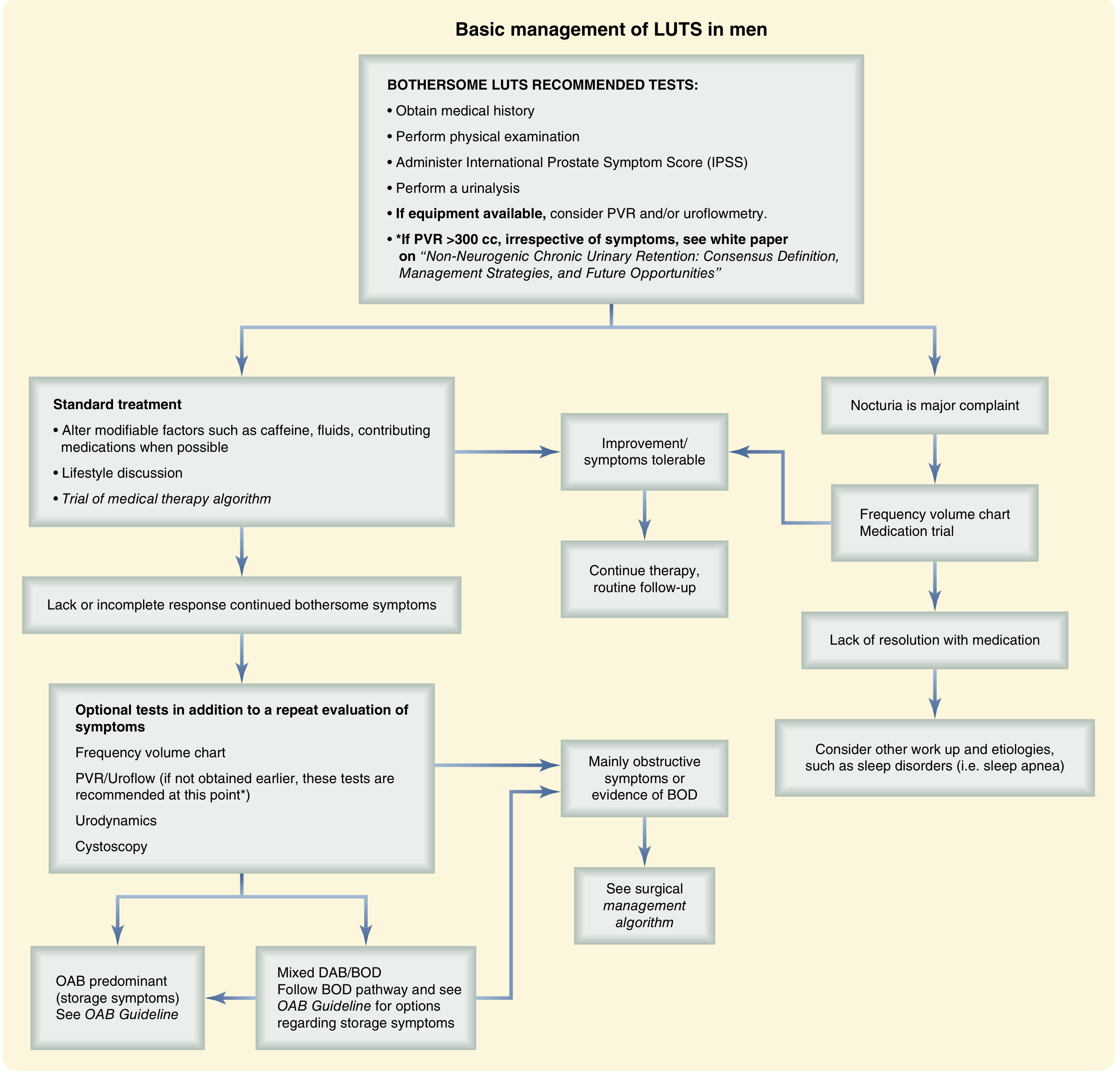
AUA/IPSS Management Algorithm
6. Management
A. Watchful Waiting (Active Surveillance)
- Lifestyle and behavioral modifications (see below)
- Annual reassessment with IPSS, PVR, uroflowmetry
- Appropriate for patients who are not bothered by their symptoms
- Reduce evening fluid intake (limit after 6 PM)
- Avoid caffeine and alcohol (irritants → increase frequency/urgency)
- Bladder training (timed voiding, urgency suppression techniques)
- Double voiding (void, wait a few minutes, void again)
- Avoid constipation (worsen BOO)
- Weight loss
- Review medications that worsen LUTS (decongestants/alpha-stimulants, anticholinergics, diuretics)
B. Surgical Indications (Absolute)
- Acute urinary retention (failed voiding trial after catheter removal)
- Recurrent UTIs attributed to BPH
- Bladder calculi from BOO
- Gross hematuria recurrent from BPH
- Azotemia/hydronephrosis from obstructive uropathy
- Bladder diverticula causing complications
7. Pharmacology
First-line: Alpha-1 Adrenergic Receptor Blockers (α1-Blockers)
| Drug | Selectivity | Dose | Key Features |
|---|---|---|---|
| Tamsulosin (Flomax) | α1A/α1D selective | 0.4-0.8 mg once daily | Most widely used; uroselective; minimal BP effect; retrograde ejaculation most common SE |
| Silodosin (Rapaflo) | α1A highly selective | 8 mg once daily | Most uroselective; highest rate of retrograde ejaculation (~28%) |
| Alfuzosin (Uroxatral) | α1 non-subtype selective | 10 mg once daily | Uroselective formulation; good BP profile |
| Doxazosin (Cardura) | Non-selective α1 | 1-8 mg once daily | Also treats hypertension; orthostatic hypotension common |
| Terazosin (Hytrin) | Non-selective α1 | 1-10 mg once daily | Also treats hypertension; dose titration required |
| Prazosin (Minipress) | Non-selective α1 | 2-20 mg daily divided | Older, less commonly used for BPH now |
Second-line: 5α-Reductase Inhibitors (5ARIs)
| Drug | 5AR Isoform Inhibited | Dose | Key Features |
|---|---|---|---|
| Finasteride (Proscar) | Type 2 only | 5 mg once daily | Generic available; 6 months for full effect; reduces PSA by ~50% |
| Dutasteride (Avodart) | Types 1 AND 2 | 0.5 mg once daily | Greater DHT suppression (~98%); longer half-life (5 weeks) |
Combination Therapy (α1-Blocker + 5ARI)
- Tamsulosin + dutasteride (Jalyn): fixed-dose combination
- Provides rapid symptom relief (from α-blocker) + long-term disease modification (from 5ARI)
Phosphodiesterase Type 5 Inhibitors (PDE5 Inhibitors)
- Tadalafil (Cialis) 5 mg daily: FDA-approved for both BPH/LUTS and ED. Well-tolerated. Contraindicated with nitrates.
- Particularly useful in men with both BPH and ED (very common co-morbidity)
Anticholinergic Agents / Beta-3 Agonists (for OAB/Storage Symptoms)
- Solifenacin, oxybutynin, tolterodine, fesoterodine: Antimuscarinics; block M2/M3 receptors in detrusor → reduce involuntary contractions. Use with caution: can precipitate urinary retention if PVR >200 mL.
- Mirabegron (beta-3 agonist): Activates β3-adrenergic receptors → detrusor relaxation during filling; safer than antimuscarinics (less retention risk); can be combined with anticholinergics.
Phytotherapy (Herbal)
- Saw palmetto (Serenoa repens): widely used; mechanism unclear; conflicting evidence from RCTs; not strongly recommended in AUA guidelines
- Beta-sitosterol, Pygeum africanum: some benefit in small studies; limited evidence
Surgical Options
| Procedure | Description | Key Points |
|---|---|---|
| TURP (Transurethral Resection of Prostate) | Gold standard; resects obstructing prostate tissue with electrocautery loop | Bipolar/monopolar; saline irrigation with bipolar avoids dilutional hyponatremia |
| HoLEP (Holmium Laser Enucleation) | Enucleates whole adenoma; suitable for large prostates | Excellent outcomes; less blood loss; steep learning curve |
| ThuLEP (Thulium Laser Enucleation) | Similar to HoLEP; continuous-wave laser | Effective alternative |
| PVP (Photoselective Vaporization) | GreenLight laser vaporizes tissue | Outpatient; good for high-risk patients on anticoagulation |
| Simple open prostatectomy (Millin's/Freyer's) | For very large prostates (>80-100 g); enucleates adenoma | Most effective for large glands; higher morbidity |
| TUMT (Microwave Thermotherapy) | Office-based; less durable results | For patients unfit for surgery |
| Urolift (Prostatic Urethral Lift) | Implants hold lobes apart; preserves ejaculation | No tissue removal; best for smaller prostates |
| Rezum (Water Vapor Therapy) | Steam injection causes convective tissue destruction | Office-based; good ejaculatory preservation |
- Goldman-Cecil Medicine, International Edition (pp. 1316-1318)
- Sabiston Textbook of Surgery, 21st Edition (pp. 2824-2826)
- Campbell Walsh Wein Urology, 3-Volume Set
- Robbins & Kumar Basic Pathology (p. 659)
- Textbook of Family Medicine, 9th Edition
PART 2: Impotence / Erectile Dysfunction (ED)
1. Definition
- Loss of libido (decreased sexual desire - primarily hormonal/psychological)
- Ejaculatory disorders (premature ejaculation, anejaculation, retrograde ejaculation)
- Orgasmic dysfunction
2. Epidemiology
- 10-15% of all adult American men
- In one landmark study (MMAS - Massachusetts Male Aging Study): 52% of men aged 40-70 years experienced some degree of ED
- Prevalence increases dramatically with age: ~40% at age 40; ~70% at age 70
- Higher prevalence in: type 2 diabetes mellitus, post-radical prostatectomy, cardiovascular disease, hypertension, depression
3. Types / Classification
A. By Etiology
| Type | Description | Proportion |
|---|---|---|
| Vasculogenic | Most common organic cause; arterial insufficiency + venous leakage | ~40-50% |
| Neurogenic | Disrupted nerve supply | ~10-20% |
| Endocrine/Hormonal | Hormonal abnormalities | ~5-10% |
| Psychogenic | Psychological factors | ~10-20% |
| Drug-induced/Iatrogenic | Medications, surgery | ~25% |
| Mixed | More than one etiology (most common in practice) | Majority |
B. By Degree of Severity
- Mild: Occasional difficulty; erections usually adequate
- Moderate: Frequent but not always inadequate erections
- Severe (complete ED): Inability to achieve/maintain erection in virtually all attempts
C. By Origin
- Primary ED: Never able to achieve erection (rare; usually psychological or severe organic)
- Secondary ED: Acquired after a period of normal function (most common)
4. Causes
Vasculogenic (Most Common Organic Cause)
- Atherosclerosis of internal pudendal/cavernous arteries (shares pathophysiology with cardiovascular disease)
- Risk factors: hypertension, diabetes, hyperlipidemia, smoking, obesity
- Pelvic irradiation
- Inability of corporeal smooth muscle to relax adequately → failure of venous compression
- Associated with Peyronie's disease, aging, trauma
Neurogenic
- Central causes: Parkinson's disease, Alzheimer's, multiple sclerosis, cerebrovascular disease, spinal cord injury, epilepsy
- Peripheral causes: Diabetic autonomic neuropathy (most common), radical prostatectomy/cystectomy (nerve damage to neurovascular bundles), pelvic surgery, urethral trauma
- Nerve damage from surgery is particularly common: prostatectomy, TURP, rectal surgery, aortoiliac surgery
Endocrine/Hormonal
- Hypogonadism (primary or secondary): ↓ testosterone → ↓ libido + ED; caused by Klinefelter syndrome, orchitis, pituitary tumors, aging
- Hyperprolactinemia: Elevated prolactin suppresses GnRH → ↓ LH → ↓ testosterone → ED (occurs in <2% of ED cases)
- Hyperthyroidism / Hypothyroidism
- Diabetes mellitus: Multiple mechanisms - vasculopathy, neuropathy, endothelial dysfunction, psychological factors
Psychogenic
- Performance anxiety (most common psychogenic cause)
- Depression (strongly associated; also worsened by antidepressant therapy)
- Anxiety disorders
- Relationship problems / partner conflict
- Grief, stress, PTSD
- Sexual identity issues
- History of sexual abuse or trauma
- Psychogenic: Sudden onset, situational (ED with certain partners but not others), normal nocturnal/early morning erections, young age, identifiable psychosocial precipitant
- Organic: Gradual onset, consistent regardless of situation, absent nocturnal erections, older age, vascular/neurological risk factors
Drug-Induced (up to 25% of ED cases)
| Drug Category | Examples |
|---|---|
| Antihypertensives | Beta-blockers (most common), thiazides, clonidine, methyldopa |
| Antidepressants | SSRIs (most commonly), TCAs, MAOIs; bupropion is less likely to cause ED |
| Antipsychotics | Haloperidol, risperidone (via prolactin elevation) |
| Antiandrogens | Spironolactone, cimetidine, 5α-reductase inhibitors, GnRH analogues, ketoconazole |
| Alcohol (chronic) | Central and peripheral effects; liver disease → ↑ estrogen |
| Opioids | Suppress gonadotropin release → hypogonadism |
| Digoxin | Estrogen-like effect |
| Anticholinergics | Impair parasympathetic erectile reflex |
| Recreational drugs | Tobacco (vasoconstriction), cocaine, cannabis, heroin |
| Antiretrovirals (HAART) | Particularly PIs; metabolic effects; ↓ testosterone |
Systemic Disease
- Cardiovascular disease (endothelial dysfunction)
- CKD/uremia (elevated prolactin, hypogonadism)
- Liver cirrhosis (↑ estrogen, ↓ testosterone)
- Chronic pulmonary disease (hypoxia)
- HIV infection (50-53% prevalence of ED in HIV-positive men, even in young men; worsened by HAART)
Aging
5. Pathophysiology
Normal Physiology of Erection
- Sexual stimulation (tactile, visual, psychogenic) → activation of parasympathetic (S2-S4) and NANC nerve fibers in the neurovascular bundles of the cavernous nerve
- NANC nerve terminals and penile endothelium release nitric oxide (NO)
- NO activates soluble guanylate cyclase → converts GTP → cyclic GMP (cGMP)
- cGMP activates protein kinase G → phosphorylates K+ channels and Ca2+ channels → smooth muscle relaxation in corpora cavernosa and penile arterioles
- Relaxed smooth muscle → dilation of cavernous arteries and helicine arteries → increased blood inflow to lacunar spaces (sinusoids)
- Tumescence: Engorgement of cavernosa → passive venous compression of subtunica venules against the tunica albuginea (veno-occlusive mechanism) → erection maintained
- After ejaculation: sympathetic activation → norepinephrine → ↑ intracellular Ca2+ → smooth muscle contraction → detumescence. PDE5 degrades cGMP → also contributes to detumescence
Pathophysiologic Mechanisms of ED
- Risk factors (DM, HTN, smoking, dyslipidemia) → oxidative stress → ↓ NO bioavailability → impaired smooth muscle relaxation → failure to fill cavernosal sinusoids
- Penile vasculature is an early sentinel of systemic vascular disease (penile arteries are smaller, so atherosclerosis manifests earlier there than in coronary or cerebral vessels - explaining the lag between ED and symptomatic cardiac disease)
- Aging, pelvic nerve damage (surgery) → ↓ NO release → impaired erection initiation
- Failure of corporeal smooth muscle relaxation → sinusoids not fully engorged → subtunica veins not compressed → venous outflow continues → failure to maintain erection
- Testosterone has permissive role in NO synthase expression and penile tissue health; profound hypogonadism → decreased NO synthase → structural changes in cavernosa
- Hyperprolactinemia suppresses hypothalamic GnRH → ↓ LH/FSH → ↓ testosterone
- Loss of cavernous nerve input (from radical prostatectomy, diabetes, spinal cord disease) → no NO release initiated → no erection despite intact vascular mechanism
- Recovery after nerve-sparing prostatectomy takes 12-18 months; PDE5 inhibitors aid recovery
6. Diagnostic Approach
History
- Sexual history: Onset (sudden vs. gradual), duration, situational nature (with all partners/situations or selective?), presence of nocturnal erections, libido, ejaculatory function, relationship factors
- SHIM / IIEF-5 (Sexual Health Inventory for Men / International Index of Erectile Function): 5-question validated questionnaire; scores 5-7 = severe, 8-11 = moderate, 12-16 = mild-moderate, 17-21 = mild, 22-25 = no ED
- Medical history: DM, CVD, hypertension, hyperlipidemia, neurological disease, pelvic surgery/radiation, trauma
- Drug history: All medications, recreational drugs, alcohol, tobacco
- Psychosocial history: Stress, depression, anxiety, relationship status, past sexual experiences
Physical Examination
- Cardiovascular: BP, peripheral pulses, bruits (aortoiliac occlusive disease can present as ED + bilateral buttock claudication - Leriche syndrome)
- Genital exam: Penile abnormalities (Peyronie's plaques), testicular size (hypogonadism = small/soft testes), secondary sexual characteristics
- Neurological: Perianal sensation, bulbocavernosus reflex, lower extremity DTRs
- Endocrine: Signs of hypogonadism (gynecomastia, reduced body hair, small testes), thyroid examination
Laboratory Tests
| Test | Purpose |
|---|---|
| Serum testosterone (total, free) | Hypogonadism; obtain morning fasting levels (normal diurnal variation) |
| LH, FSH | Distinguish primary (↑ LH/FSH) from secondary hypogonadism (↓ or normal) |
| Prolactin | If testosterone low/signs of hypogonadism; <2% of ED cases |
| Fasting glucose / HbA1c | Diabetes (neuropathy + vasculopathy) |
| Lipid profile | Cardiovascular risk assessment |
| Thyroid function (TSH) | Hypo/hyperthyroidism |
| CBC, CMP | General health, renal/hepatic function |
| PSA | If testosterone therapy being considered (contraindicated in prostate cancer) |
Specialized Tests (Second-line, as needed)
| Test | Purpose |
|---|---|
| Nocturnal penile tumescence (NPT) testing (Rigiscan) | Gold standard to distinguish psychogenic from organic; normal NPT in psychogenic ED; absent/reduced in organic |
| Penile Doppler ultrasound (dynamic, after intracavernous injection) | Assess arterial flow (peak systolic velocity >25 cm/s = normal) and venous leakage; gold standard for vasculogenic ED |
| Intracavernosal injection test | Injection of alprostadil/papaverine/phentolamine; positive response (rigid erection) suggests adequate arterial supply |
| Cavernosometry / cavernosography | Assess venous leakage; seldom needed (reserve for surgical candidates) |
| Pudendal arteriography | Pre-surgical assessment in young men with arterial disease from trauma |
| Neurophysiologic tests | Bulbocavernosus reflex latency, sensory-evoked potentials; for neurogenic ED |
7. Management
Step 1: Lifestyle Modification and Risk Factor Management
- Weight loss (obesity: insulin resistance → ↓ testosterone, endothelial dysfunction; weight loss improves ED in obese patients)
- Smoking cessation
- Reduce alcohol intake
- Regular aerobic exercise (improves endothelial function)
- Optimize diabetes, hypertension, hyperlipidemia control
- Stop or switch offending medications where possible (e.g., switch from beta-blocker to amlodipine; switch from SSRI to bupropion)
- Psychosexual counseling (alone or combined with pharmacotherapy)
Step 2: Pharmacotherapy
First-line: PDE5 Inhibitors
| Drug | Dose | Onset | Duration | Key Features |
|---|---|---|---|---|
| Sildenafil (Viagra) | 25-100 mg prn (usual: 50 mg) | ~60 min | 4-6 hours | First approved (1998); affected by fatty meals (delay absorption); blue visual tint (cyanopsia) at higher doses |
| Tadalafil (Cialis) | 10-20 mg prn OR 5 mg daily | 30-45 min | 36 hours ("the weekend pill") | Longest duration; daily dosing approved; also approved for BPH/LUTS; less food interaction |
| Vardenafil (Levitra) | 5-20 mg prn | 30-60 min | 4-5 hours | Similar to sildenafil; slightly more potent |
| Avanafil (Stendra) | 50-200 mg prn | 15-30 min (fastest onset) | 4-6 hours | Most selective; faster onset; fewer visual side effects |
- Concurrent use of organic nitrates (nitroglycerin, isosorbide mono/dinitrate, amyl nitrite/poppers) - severe potentially fatal hypotension
- Severe cardiovascular disease where sexual activity is inadvisable
- Recent (<6 months) myocardial infarction, stroke, life-threatening arrhythmia, angina, severe hypotension/hypertension, cardiac failure
- Retinitis pigmentosa
Hormonal Therapy
- Testosterone replacement therapy (TRT):
- Intramuscular testosterone cypionate/enanthate: 150-200 mg IM every 2-3 weeks
- Testosterone gel (1-2%): 50-100 mg topically daily
- Testosterone patches: 5-10 mg/day
- Subcutaneous testosterone pellets
- Caution: Absolute contraindication in prostate cancer and breast cancer; use with caution in polycythemia, severe BPH, sleep apnea
- Treat concomitant conditions: hyperprolactinemia (bromocriptine/cabergoline), hypothyroidism (levothyroxine)
Step 3: Second-line - Local Therapies
Intracavernosal Injection (ICI) Therapy
| Agent | Mechanism | Dose | Efficacy |
|---|---|---|---|
| Alprostadil (prostaglandin E1; Caverject, Edex) | Direct smooth muscle relaxation + vasodilation | 2.5-40 μg IC | ~70-80% success |
| Trimix (alprostadil + papaverine + phentolamine) | Multiple mechanisms: PGE1, α-blocker, non-specific smooth muscle relaxant | Individualized | ~80-90% success; especially useful in neurogenic ED |
| Bimix (papaverine + phentolamine) | α-blocker + non-selective smooth muscle relaxant | Individualized | Used when alprostadil contraindicated |
Intraurethral Alprostadil (MUSE - Medicated Urethral System for Erection)
- Alprostadil pellet inserted into urethra via applicator
- Dose: 125-1000 μg
- Absorbed through urethral mucosa into corpus spongiosum → diffuses to corpora cavernosa
- Success rate ~40-65%
- Side effects: urethral burning/pain, hypotension, dizziness; priapism less common than ICI
- Advantage: Non-injectable; option for needle-phobic patients
Vacuum Erection Device (VED / Penile Pump)
- External vacuum device draws blood into corpora → constriction band applied at base to maintain erection
- Non-pharmacological; useful especially in post-prostatectomy, anticoagulated patients
- Success rate ~60-70%
- Side effects: Ecchymosis, petechiae, numbness, cold/dusky erection, pain, ejaculatory difficulties from constriction ring
Step 4: Surgical Treatment
Penile Prosthesis (Implant) - Gold Standard for Refractory ED
| Type | Description | Advantages |
|---|---|---|
| Inflatable (IPP) - 3-piece | Cylinders + reservoir + pump; most physiological | Most natural feel; concealable; most preferred |
| Inflatable (IPP) - 2-piece | Cylinders + pump (no reservoir) | Simpler; for patients with prior pelvic surgery/radiation |
| Semi-rigid (malleable) | Permanently semi-erect; bent for concealment | Simple; no mechanical failure; used in manual dexterity-impaired patients |
- Patient satisfaction: 85-90% for inflatable prostheses
- Complications: Infection (2-3%; devastating; requires removal), mechanical failure, erosion, migration
Penile Vascular Surgery
- Penile arterial revascularization: For young men (<55 yr) with focal arteriogenic ED from perineal/pelvic trauma (bicycle, straddle injury)
- Venous ligation: For venous leakage; poor long-term results; rarely performed
Psychological / Psychosexual Therapy
- Sex therapy and couples therapy: For psychogenic ED or psychogenic component
- Cognitive-behavioral therapy (CBT)
- Treatment of depression (note: many antidepressants worsen ED; bupropion + mirtazapine have least sexual side effects)
- Combination with PDE5 inhibitors improves outcomes vs. either alone
8. Pharmacology Summary
PDE5 Inhibitor Comparison Table
| Property | Sildenafil | Tadalafil | Vardenafil | Avanafil |
|---|---|---|---|---|
| Onset | 60 min | 30-45 min | 30-60 min | 15-30 min |
| Duration | 4-6 hrs | 36 hrs | 4-5 hrs | 4-6 hrs |
| Food effect | Affected (high fat delays) | None | Affected | None |
| PDE selectivity | PDE5 | PDE5 > PDE11 | PDE5 | PDE5 (most selective) |
| Special uses | Pulmonary HTN | BPH, daily use, pulmonary HTN | - | - |
| Dose adjustment | Lower with CYP3A4 inhibitors | Same | Same | Same |
ED Pharmacotherapy Algorithm
- First-line: PDE5 inhibitor (sildenafil 50 mg or tadalafil 10 mg prn) + lifestyle modification
- Hypogonadism confirmed: Add testosterone replacement
- PDE5 inhibitor failure: Check compliance, optimize dose, address contributing factors; try alternative PDE5 inhibitor
- Second-line: ICI (alprostadil or trimix) OR MUSE OR vacuum erection device
- Refractory: Penile prosthesis
- Goldman-Cecil Medicine, International Edition (pp. 2542-2543)
- Textbook of Family Medicine, 9th Edition (pp. 1193-1194)
- Campbell Walsh Wein Urology, 3-Volume Set (pp. 2130)
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry (pp. 6140-6141)
- Sabiston Textbook of Surgery, 21st Edition
provide defenition, types, causes, pathophysiology, diagnostic approach , management along with pharmacology for CONGENITAL HEART DISEASE, COR PULMONALE, IHD, CARDIAC FAILURES, CARDIOMYOPATHY, PERICARDITIS, ENDOCARDITIS, HYPERTENSION.
provide defenition, types, causes, pathophysiology, diagnostic approach , management along with pharmacology for CONGENITAL HEART DISEASE, COR PULMONALE, IHD, RHD- VALVULAR DISEASES, CARDIAC FAILURES, CARDIOMYOPATHY, PERICARDITIS, ENDOCARDITIS, HYPERTENSION.
CARDIOVASCULAR DISEASES: Comprehensive Reference
1. CONGENITAL HEART DISEASE (CHD)
Definition
Types / Classification
A. Acyanotic CHD (Left-to-Right Shunts / Obstruction)
| Defect | Key Features |
|---|---|
| VSD (Ventricular Septal Defect) | Most common CHD (~30%); 90% membranous type; 50% of small VSDs close spontaneously; large VSDs → pulmonary HTN |
| ASD (Atrial Septal Defect) | Most common CHD diagnosed in adults (since VSD often closes); fixed split S2; risk of paradoxical embolism |
| PDA (Patent Ductus Arteriosus) | Failure of ductus arteriosus to close postnatally; machine murmur; premature infants; treated with indomethacin (PG inhibitor) |
| AVSD (Atrioventricular Septal Defect) | Associated with Down syndrome |
| Aortic stenosis | Bicuspid aortic valve most common; obstruction of LV outflow |
| Pulmonary stenosis | Right ventricular outflow tract obstruction |
| Coarctation of aorta | Narrowing of aortic arch; upper limb HTN + weak femoral pulses; associated with Turner syndrome; radio-femoral delay |
B. Cyanotic CHD ("Five Ts" + more) - Right-to-Left Shunts
| Defect | Key Features |
|---|---|
| Tetralogy of Fallot (TOF) | Most common cyanotic CHD manifesting in post-infancy; 4 components: VSD + RVOT obstruction (pulmonary stenosis) + overriding aorta + RV hypertrophy; "tet spells" (hypercyanotic episodes); boot-shaped heart on CXR |
| Transposition of Great Arteries (TGA) | Aorta from RV, pulmonary artery from LV; most common cyanotic CHD presenting at birth; requires PDA or ASD for survival; prostaglandin E1 to maintain PDA |
| Tricuspid atresia | Absent tricuspid valve; requires ASD + VSD for survival |
| Truncus arteriosus | Single great vessel arising from heart |
| Total Anomalous Pulmonary Venous Return (TAPVR) | Pulmonary veins drain to right side of heart |
| Ebstein anomaly | Downward displacement of tricuspid valve into RV; associated with maternal lithium use |
Causes
- Genetic (10%): Trisomy 21 (Down - AVSD), Turner syndrome (coarctation, bicuspid aortic valve), Noonan syndrome (pulmonary stenosis), DiGeorge syndrome (22q11 deletion - truncus arteriosus, ToF), Marfan syndrome (aortic dilatation)
- VACTERL association: Vertebral anomalies, Anal atresia, Cardiac defects, Tracheoesophageal fistula, Esophageal atresia, Renal anomalies, Limb anomalies
- Teratogens: Rubella (PDA, pulmonary stenosis), thalidomide, alcohol (fetal alcohol syndrome), retinoic acid, phenytoin, lithium (Ebstein)
- Maternal DM: Transposition, VSD, hypertrophic cardiomyopathy
- Isolated embryological malformation (90%)
Pathophysiology
Left-to-Right Shunts (Acyanotic)
Right-to-Left Shunts (Cyanotic)
Diagnostic Approach
| Investigation | Findings |
|---|---|
| Pulse oximetry | SpO₂ <95% suggests cyanotic CHD; mandatory newborn screen |
| Chest X-ray | Boot-shaped heart (TOF); egg-on-string (TGA); rib notching (coarctation after age 8); cardiomegaly (large L→R shunts) |
| ECG | RVH (TOF, pulmonary stenosis), LVH (large VSD), right axis deviation |
| Echocardiography | Gold standard for anatomy, flow, gradients, ventricular function |
| Cardiac MRI/CT | Detailed anatomy, vascular anomalies, pre-surgical planning |
| Cardiac catheterization | Hemodynamics, pressures, oxygen saturations; pre-surgical assessment |
| Genetic testing | Karyotype, FISH for 22q11, chromosome microarray |
Management and Pharmacology
- Prostaglandin E1 (alprostadil): Maintains patent ductus arteriosus in duct-dependent lesions (TGA, pulmonary atresia, hypoplastic left heart syndrome) - 0.05-0.1 μg/kg/min IV infusion
- Indomethacin (COX inhibitor) or ibuprofen: Close PDA in premature infants (inhibit prostaglandin synthesis)
- Propranolol (oral): Reduces RVOT obstruction in TOF; reduces tet spell frequency
- Diuretics (furosemide): Manage heart failure from large shunts
- Digoxin: For heart failure in infants with large L→R shunts
- VSD/ASD: Surgical patch or device closure (catheter-based); ASD: often transvenous device closure (Amplatzer device)
- TOF: Complete repair (patch VSD + RVOT reconstruction) usually at 3-6 months
- TGA: Arterial switch operation (Jatene procedure) in first 2 weeks of life
- Coarctation: Balloon dilation ± stenting OR surgical resection
- Eisenmenger syndrome: Pulmonary vasodilators (bosentan, sildenafil), anticoagulation, avoid vasodilators that drop SVR; heart-lung transplantation is definitive
2. COR PULMONALE
Definition
Types
- Acute cor pulmonale: RV dilation with little or no hypertrophy; e.g., massive pulmonary embolism (sudden severe RV pressure overload; if embolism causes sudden death, heart may be normal-sized)
- Chronic cor pulmonale: RV hypertrophy + dilation from sustained pulmonary hypertension; e.g., COPD, pulmonary fibrosis; RV wall thickness may equal or exceed LV thickness
Causes
| Category | Examples |
|---|---|
| Parenchymal lung disease | COPD (most common), emphysema, interstitial fibrosis/ILD, bronchiectasis, cystic fibrosis |
| Pulmonary vascular disease | Primary pulmonary hypertension (PAH), recurrent pulmonary emboli, vasculitis, sickle cell disease |
| Neuromuscular/chest wall | Severe kyphoscoliosis, obesity hypoventilation syndrome, neuromuscular disease, severe OSA |
| Hypoxic states | Living at high altitude (chronic hypoxic vasoconstriction) |
| Toxic | Anorexigens (fenfluramine), HIV, cocaine |
Pathophysiology
- Primary lung disease → alveolar hypoxia (most important mechanism) + destruction of alveolar capillary bed + lung hyperinflation + polycythemia-related ↑ blood viscosity
- Hypoxic pulmonary vasoconstriction (HPV): Hypoxia → vasoconstriction of pulmonary arterioles (Euler-Liljestrand reflex) → ↑ pulmonary vascular resistance (PVR)
- Persistent HPV + structural remodeling (smooth muscle hypertrophy, intimal thickening of pulmonary arteries) → sustained pulmonary arterial hypertension (PAH)
- RV must overcome elevated PVR → RV pressure overload → concentric RV hypertrophy (Laplace's law: increased wall thickness normalizes wall stress)
- Eventually RV dilatation → tricuspid regurgitation → right-sided heart failure (raised JVP, peripheral edema, hepatomegaly, ascites)
- Distortion of LV shape by enlarged RV → interventricular septal shift → impaired LV filling → reduced cardiac output
Clinical Features / Diagnosis
- Elevated JVP with prominent 'a' and 'v' waves
- Right ventricular heave/parasternal lift
- Loud P2 (loud pulmonary component of S2)
- Tricuspid regurgitation murmur (pansystolic at LLSB, increases with inspiration)
- Peripheral edema, ascites, hepatomegaly
- Cyanosis (central, from hypoxemia)
| Test | Findings |
|---|---|
| ECG | P pulmonale (tall P in II, III, aVF >2.5mm), right axis deviation, RVH (dominant R in V1, S wave in V6), RBBB, S1Q3T3 (acute PE) |
| CXR | Enlarged PA, prominent hilar shadows, RV enlargement (filling of retrosternal space on lateral), oligemic peripheral lung fields |
| Echocardiography | RV hypertrophy/dilation, elevated RV systolic pressure (estimated from TR jet), paradoxical septal motion |
| Pulmonary function tests | Obstructive (COPD) or restrictive pattern; ↓ DLCO |
| ABG | Hypoxemia ± hypercapnia (COPD), ↑ bicarbonate (chronic) |
| CT Pulmonary Angiography | PE, lung disease, vessel remodeling |
| Right heart catheterization | Gold standard: elevated PAP (>25 mmHg at rest), elevated PVR, normal PCWP |
Management and Pharmacology
- COPD: Bronchodilators, pulmonary rehabilitation, smoking cessation
- PE: Anticoagulation (LMWH/DOAC), thrombolysis if hemodynamically unstable
- PaO₂ <55 mmHg at rest, or <60 mmHg with polycythemia or cor pulmonale
- ≥15 hours/day; reduces pulmonary vasoconstriction and mortality
- Phosphodiesterase-5 inhibitors: Sildenafil 20 mg TID, tadalafil 40 mg OD → ↑ cGMP → pulmonary vasodilation
- Endothelin receptor antagonists: Bosentan 62.5-125 mg BD, ambrisentan, macitentan → block ET-1 mediated vasoconstriction; liver toxicity monitoring required
- Prostacyclin analogues: Epoprostenol (IV continuous infusion - gold standard for severe PAH), treprostinil (SC/inhaled/oral), iloprost (inhaled); potent pulmonary vasodilators; prostacyclin analogs
- Riociguat: sGC stimulator; for PAH and chronic thromboembolic PH (CTEPH)
- Selexipag: Selective IP receptor agonist; oral; reduces PAH progression
3. ISCHEMIC HEART DISEASE (IHD) / CORONARY ARTERY DISEASE
Definition
Types
| Type | Definition |
|---|---|
| Stable angina | Predictable chest pain on exertion; relieved by rest/nitrates; fixed coronary stenosis |
| Unstable angina (UA) | New onset, rest angina, or rapidly worsening angina; plaque disruption without necrosis (no troponin rise) |
| NSTEMI | Plaque rupture with partial occlusion; subendocardial infarction; ↑ troponin; no ST elevation |
| STEMI | Complete occlusion; transmural infarction; ↑ troponin + ST elevation; emergency reperfusion needed |
| Silent ischemia | Asymptomatic ischemia; common in diabetics (neuropathy) |
| Sudden cardiac death | First manifestation in many patients; VF from ischemia |
Causes / Risk Factors
Pathophysiology
- Endothelial injury (from HTN, smoking, dyslipidemia, shear stress) → endothelial dysfunction
- LDL enters intima → oxidized LDL → monocyte recruitment → foam cell formation → fatty streak
- Smooth muscle cell migration + proliferation + extracellular matrix → fibrous plaque (atheroma)
- Vulnerable plaque = large lipid core + thin fibrous cap → prone to rupture
- Plaque rupture/erosion → exposure of thrombogenic material → platelet aggregation + thrombus formation → lumen occlusion → acute MI
- Seconds: ATP depletion
- <2 minutes: Loss of contractility
- 10 minutes: ATP reduced to 50%
- 20-40 minutes: Irreversible cell injury (point of no return)
- Ischemia progresses from subendocardium outward (wavefront phenomenon)
- LAD → anterior wall LV + anterior 2/3 septum + apex (most common; "widowmaker")
- RCA → inferior wall LV + posterior wall + right ventricle + SA/AV nodes
- LCx → lateral wall LV
- Contractile dysfunction → cardiogenic shock (>40% LV lost)
- Papillary muscle dysfunction → acute mitral regurgitation
- Free wall rupture → hemopericardium/tamponade (2-7 days)
- Ventricular septal rupture → acute VSD with shunt
- Ventricular aneurysm → mural thrombus, arrhythmias
- Post-MI pericarditis (fibrinous; 1-3 days) / Dressler syndrome (autoimmune; weeks later)
- Arrhythmias (VF in first hour, complete heart block with inferior MI)
Diagnostic Approach
| Test | Stable IHD | ACS |
|---|---|---|
| ECG | Normal or ST depression/T-wave changes during ischemia | STEMI: ST elevation + new LBBB; NSTEMI/UA: ST depression, T inversion |
| Troponin I/T | Normal | ↑ in NSTEMI/STEMI (appears 3-6 hrs, peaks 12-24 hrs, normalizes 7-10 days) |
| CK-MB | Normal | ↑ in MI; useful for re-infarction (normalizes in 48-72 hrs) |
| Echocardiography | Regional wall motion abnormalities, LVEF | Assess LVEF, complications (MR, VSD, effusion) |
| Exercise stress test | ST changes with exercise → ischemia | Contraindicated in acute phase |
| Stress echo/Nuclear (MPI) | Identify reversible ischemia, viability | Not in acute setting |
| CT Coronary Angiography | Non-invasive coronary anatomy; Ca++ score | Not in acute setting |
| Coronary angiography | Gold standard for anatomy/intervention planning | Emergency in STEMI; urgent in high-risk NSTEMI |
| CXR | May show pulmonary edema | Cardiomegaly, pulmonary edema |
Management and Pharmacology
Acute STEMI (Time = Muscle)
Antiplatelet/Anticoagulant Therapy
| Drug | Mechanism | Use |
|---|---|---|
| Aspirin | Irreversible COX-1 inhibition → ↓ TXA₂ → ↓ platelet aggregation | 300 mg loading, then 75-100 mg OD lifelong |
| Clopidogrel (Plavix) | ADP P2Y12 receptor antagonist; prodrug (CYP2C19) | DAPT with aspirin ≥12 months post-ACS/PCI |
| Ticagrelor (Brilinta) | Reversible P2Y12 antagonist; direct-acting; more potent | Preferred over clopidogrel in ACS; 90 mg BD |
| Prasugrel (Effient) | Irreversible P2Y12; faster onset; avoid in TIA/stroke, elderly, low weight | High-risk PCI patients |
| Heparin (UFH) | Activates antithrombin III; inhibits Xa + IIa | STEMI/NSTEMI anticoagulation; IV infusion |
| Enoxaparin (LMWH) | Mainly anti-Xa | NSTEMI management; SC BD |
| Bivalirudin | Direct thrombin inhibitor | PCI anticoagulation, HIT patients |
| GPIIb/IIIa inhibitors (abciximab, eptifibatide, tirofiban) | Block final common pathway of platelet aggregation | High-risk PCI, bailout situations |
Long-term Medications Post-MI
| Drug Class | Drug | Mechanism | Benefit |
|---|---|---|---|
| Beta-blockers | Metoprolol, carvedilol, bisoprolol | ↓ HR, ↓ O₂ demand, antiarrhythmic | ↓ mortality, ↓ reinfarction, ↓ sudden death |
| ACE inhibitors | Ramipril, lisinopril | ↓ Ang II → ↓ afterload, prevent remodeling | ↓ mortality especially with ↓ EF |
| ARBs | Valsartan, losartan | Ang II receptor blockade | Use if ACE-I intolerant |
| Statins (high-intensity) | Atorvastatin 40-80mg, rosuvastatin 20-40mg | HMG-CoA reductase inhibition → ↓ LDL | ↓ mortality, plaque stabilization |
| Nitrates | GTN (sublingual), isosorbide dinitrate/mononitrate | ↑ NO → venodilation + vasodilation → ↓ preload + afterload | Symptomatic angina relief |
| Eplerenone / Spironolactone | Aldosterone antagonist | Prevents cardiac remodeling | Post-MI with EF ≤40%, HF or DM |
| Ivabradine | HCN channel blocker → ↓ HR | Angina + HF with HR >70 despite beta-blockers |
- Calcium channel blockers (amlodipine, diltiazem): Vasodilation; for stable angina when beta-blockers contraindicated
- Ranolazine: Late Na+ channel blocker → ↓ intracellular Ca²⁺ → ↓ diastolic tension; for stable angina
- Nicorandil: K+ATP channel opener + nitrate-like; reduces angina frequency
- PCI + stenting: Drug-eluting stents (DES) preferred; dual antiplatelet therapy required ≥12 months
- CABG: For left main disease, 3-vessel disease, diabetes + multivessel disease, failed PCI, severely reduced EF
4. RHD - RHEUMATIC HEART DISEASE / VALVULAR DISEASES
Definition
Types of Valvular Lesions
Mitral Stenosis (MS)
- Most common cause: RHD (nearly all cases)
- Pathophysiology: Leaflet thickening/fusion → narrowed mitral orifice → ↑ left atrial pressure → pulmonary hypertension → RV failure; LA dilation → AF risk
- Normal valve area: 4-6 cm²; Mild MS: 1.5-2.0 cm²; Moderate: 1.0-1.5 cm²; Severe: <1.0 cm²
- Symptoms: Dyspnea, orthopnea, hemoptysis (from pulmonary HTN), palpitations (AF), systemic emboli
- Exam: Mid-diastolic rumble at apex (low-pitched with opening snap); loud S1; opening snap (OS) closer to S2 = more severe
- ECG: P-mitrale (bifid P in II), LA enlargement; RVH with AF
- CXR: "Double shadow" (LA enlargement), straightening of left heart border, upper lobe blood diversion
- Echo: Domed mitral leaflets, reduced valve area (pressure half-time method), LA enlargement
- Management: Rate control in AF (beta-blockers, digoxin, CCB); anticoagulation (warfarin) for AF/emboli; diuretics; Percutaneous Mitral Balloon Commissurotomy (PMBC) for pliable valves; Mitral valve repair/replacement (metallic or bioprosthetic)
Mitral Regurgitation (MR)
- Causes: RHD, mitral valve prolapse (most common in developed countries), ischemic (papillary muscle dysfunction), IE, connective tissue disorders, dilated cardiomyopathy, rupture of chordae tendineae
- Pathophysiology: Regurgitant volume into LA → LA dilation → ↑ LVEDV (volume overload) → eccentric LV hypertrophy → eventually LV dysfunction
- Acute MR (chordal rupture, papillary muscle rupture post-MI): Pulmonary edema, cardiogenic shock
- Exam: Holosystolic murmur at apex radiating to axilla; displaced apex; soft S1; S3 (volume overload)
- Management: Vasodilators (ACEi/ARBs, nifedipine) for chronic; Surgery (repair > replacement) when LVEF <60% or LVESD >40 mm
Aortic Stenosis (AS)
- Causes: Calcific/degenerative (most common in elderly), bicuspid aortic valve (young), RHD
- Pathophysiology: Obstruction of LV outflow → ↑ LV systolic pressure → concentric LV hypertrophy → eventually LV failure; fixed CO leads to the classic triad when severe
- Classic Triad of Severe AS: Syncope, angina, dyspnea/heart failure; average survival after each: 3 yr, 5 yr, 2 yr
- Exam: Harsh ejection systolic murmur at aortic area (2R ICS) radiating to carotids; soft/absent A2; slow-rising pulse (pulsus parvus et tardus); paradoxical splitting of S2; systolic thrill
- Echo: Valve area <1.0 cm² = severe; mean gradient >40 mmHg = severe
- Management: Symptomatic = surgical AVR or TAVI (Transcatheter Aortic Valve Implantation) - TAVI preferred for high-surgical-risk patients
Aortic Regurgitation (AR)
- Causes: RHD, bicuspid aortic valve, IE, aortic root dilation (Marfan syndrome, syphilitic aortitis, hypertension), ankylosing spondylitis
- Pathophysiology: Regurgitant volume into LV → ↑ LVEDV + LVESV → eccentric hypertrophy; wide pulse pressure (high SBP + low DBP = "water hammer" pulse)
- Exam: Early diastolic decrescendo murmur at right sternal border; wide pulse pressure; "pistol shot" femorals; de Musset's sign (head bobbing); Quincke's pulsations; Austin Flint murmur (functional MS from regurgitant jet)
- Management: Vasodilators (ACEi, nifedipine) for chronic symptomatic or LVEF reduction; AVR when symptomatic or LVEF <50% or LVESD >50 mm
Tricuspid / Pulmonary Valve Disease
- Tricuspid regurgitation: Most common secondary (from RHF, IE in IV drug users); management addresses underlying cause
- Pulmonary stenosis: Often congenital; balloon valvuloplasty if severe
Diagnostic Approach to Valvular Disease
| Test | Purpose |
|---|---|
| Echocardiography (TTE/TEE) | Gold standard; anatomy, function, hemodynamics, severity, LV function |
| Doppler ultrasound | Gradients, valve areas, regurgitant volumes |
| ECG | LA/LV/RV hypertrophy, AF, conduction defects |
| CXR | Cardiomegaly, LA/LV enlargement, pulmonary congestion |
| Cardiac catheterization | Coronary angiography pre-op; hemodynamics when echo discordant |
| Cardiac MRI | Quantify regurgitant volumes, assess myocardial viability |
Pharmacology
| Indication | Drug |
|---|---|
| Rheumatic fever prophylaxis | Benzathine penicillin G 1.2 MU IM every 3-4 weeks (secondary prophylaxis for 10 years or until age 40 if no carditis); or oral phenoxymethylpenicillin 250 mg BD |
| Acute rheumatic fever treatment | Penicillin V (strep eradication); Aspirin (anti-inflammatory for carditis/arthritis) |
| Mitral stenosis AF rate control | Beta-blockers (metoprolol), digoxin, diltiazem |
| Anticoagulation (AF/mechanical valves) | Warfarin (INR 2-3 for bioprosthetic/AF; INR 2.5-3.5 for mechanical mitral) |
| Heart failure in valvular disease | ACE inhibitors/ARBs, diuretics |
| IE prophylaxis (high-risk procedures) | Amoxicillin 2g oral 30-60 min before procedure; clindamycin if penicillin allergic |
5. CARDIAC FAILURE (HEART FAILURE)
Definition
Classification
By Ejection Fraction (EF)
| Type | EF | Key Features |
|---|---|---|
| HFrEF (Heart Failure with Reduced EF) | <40% | Systolic dysfunction; dilated LV; most RCT evidence |
| HFmrEF (Heart Failure with Mildly Reduced EF) | 41-49% | Intermediate; similar clinical features |
| HFpEF (Heart Failure with Preserved EF) | ≥50% | Diastolic dysfunction; stiff ventricle; mostly elderly women with HTN/AF |
By Side Affected
- Left heart failure: Pulmonary congestion; dyspnea, orthopnea, PND, pulmonary edema
- Right heart failure: Systemic venous congestion; raised JVP, peripheral edema, hepatomegaly
- Biventricular failure: Combined features; most common presentation
By Onset
- Acute: Sudden decompensation; pulmonary edema
- Chronic: Progressive; stable symptoms with exacerbations
NYHA Classification
| Class | Description |
|---|---|
| I | No symptoms with ordinary activity |
| II | Mild limitation; comfortable at rest; slight limitation with ordinary activity |
| III | Marked limitation; comfortable only at rest; less than ordinary activity causes symptoms |
| IV | Symptoms at rest or minimal activity |
Causes
- Ischemic heart disease (most common in developed countries; ~65%)
- Hypertension (chronic pressure overload → LVH → HFpEF; or acute → decompensation)
- Cardiomyopathy (dilated, hypertrophic, peripartum)
- Valvular heart disease (AS, MR, AR)
- Arrhythmias (rapid AF, tachycardia-mediated cardiomyopathy)
- Thyroid disease (hypo/hyperthyroidism)
- Anemia (high-output failure)
- Alcohol, drugs (anthracyclines, trastuzumab, cocaine)
- Infections (viral myocarditis, Chagas disease)
- Infiltrative disease (amyloidosis, sarcoidosis, hemochromatosis)
- Genetic/familial cardiomyopathies (mutations in cytoskeletal/nuclear proteins; autosomal dominant)
- Congenital heart disease
Pathophysiology
Neurohormonal Activation (Core Mechanism)
- Sympathetic nervous system: ↑ norepinephrine → ↑ HR, ↑ contractility (short-term beneficial); chronic → receptor downregulation, cardiotoxicity, arrhythmias
- RAAS: ↓ renal perfusion → ↑ renin → ↑ Ang II → vasoconstriction + aldosterone → Na⁺ and water retention → ↑ preload/afterload → worsens overload
- ADH/Vasopressin: ↑ water retention → hyponatremia; vasoconstriction
- Natriuretic peptides (BNP, ANP): Compensatory; ↑ natriuresis, vasodilation, inhibit RAAS; become overwhelmed
Ventricular Remodeling
HFpEF Pathophysiology
Clinical Manifestations
- Dyspnea on exertion, orthopnea, PND, bendopnea
- Basal crackles (pulmonary edema), pleural effusion (right-sided > left)
- S3 gallop (volume overload), S4 (stiff ventricle)
- Displaced apex (cardiomegaly)
- Elevated JVP (>3 cm above sternal angle + 5 = >8 cm H₂O)
- Pitting peripheral edema (bilateral), ascites
- Hepatomegaly (tender), hepatojugular reflux
- Pulsatile liver (TR), jaundice (hepatic congestion)
- Fatigue, exercise intolerance (>90% of patients)
- Cardiac cachexia (advanced HF; poor prognosis)
- Atrial fibrillation (~30%)
- Pulsus alternans (advanced HF; alternating pulse volume)
- Cognitive dysfunction
Diagnostic Approach
| Test | Findings |
|---|---|
| BNP/NT-proBNP | ↑ in HF; supports diagnosis, guides prognosis; BNP <100 makes HF unlikely |
| ECG | Arrhythmias, LVH, prior MI (Q waves), LBBB (indicates CRT eligibility), right axis (RHF) |
| CXR | Cardiomegaly (CTR >50%), upper lobe blood diversion, Kerley B lines, perihilar "bat-wing" edema, pleural effusion |
| Echocardiography | LVEF, LV dimensions, valvular function, diastolic function, wall motion; essential for diagnosis |
| Cardiac MRI | Detailed myocardial function, viability, infiltrative disease |
| Labs | CBC (anemia), renal function, electrolytes, LFTs, TSH, glucose, BNP |
| Coronary angiography | If ischemic etiology suspected or new HF without clear cause |
Management and Pharmacology
HFrEF (Evidence-Based "Quadruple Therapy")
| Drug Class | Drug | Mechanism | Benefit |
|---|---|---|---|
| ACE inhibitors | Enalapril, ramipril, lisinopril | ↓ Ang II → ↓ preload+afterload, prevent remodeling | ↓ mortality ~23%, ↓ hospitalizations |
| ARBs | Valsartan, losartan, candesartan | Ang II receptor blockade | Use if ACEi-intolerant (cough/angioedema) |
| ARNI (ACEi+neprilysin inhibitor) | Sacubitril/Valsartan (Entresto) | ↑ natriuretic peptides + ↓ Ang II | Superior to enalapril (PARADIGM-HF); first-line where available |
| Beta-blockers | Carvedilol, bisoprolol, metoprolol succinate | ↓ HR, ↓ catecholamine cardiotoxicity, ↓ remodeling | ↓ mortality ~34%; start at low dose when euvolemic |
| MRA (Aldosterone antagonist) | Spironolactone, eplerenone | Block aldosterone → ↓ fibrosis, ↓ K+ loss | ↓ mortality; monitor K+ and renal function |
| SGLT2 inhibitors | Dapagliflozin, empagliflozin | ↑ glucosuria, natriuresis, osmotic diuresis; reduce cardiac fibrosis | ↓ hospitalization and CV death; now core HFrEF treatment regardless of DM status |
- Loop diuretics: Furosemide 40-80 mg OD/BD (IV in acute decompensation); torsemide, bumetanide
- Thiazides: Metolazone (combined with furosemide for diuretic resistance)
- Spironolactone: Dual role (MRA + K-sparing diuretic)
- Hydralazine + Isosorbide dinitrate: For ACEi/ARB-intolerant patients; particularly beneficial in Black patients
- Digoxin: ↑ contractility (Na/K-ATPase inhibitor), rate control in AF; reduces hospitalizations but no mortality benefit; narrow TI
- Ivabradine: ↓ HR via HCN channel block; for sinus rhythm + HR >70 despite maximized beta-blocker
- Vericiguat: Soluble guanylate cyclase stimulator; high-risk HFrEF; ↑ cGMP → vasodilation + anti-remodeling
HFpEF
- Diuretics for congestion
- Control underlying hypertension aggressively
- Rate control for AF
- SGLT2 inhibitors (empagliflozin, dapagliflozin): Recently shown to reduce hospitalizations in HFpEF (EMPEROR-Preserved, DELIVER trials)
- Treat underlying cause (revascularization for ischemia, thyroid treatment)
Acute Decompensated Heart Failure
- IV loop diuretics: Furosemide 40-200 mg IV; adjust to clinical response
- Vasodilators: IV nitroglycerin (preload reduction), nitroprusside (preload + afterload); for hypertensive acute HF
- Inotropes (cardiogenic shock): Dobutamine (β1 agonist), milrinone (PDE3 inhibitor); bridge to device/transplant
- Non-invasive ventilation (CPAP/BiPAP): For acute pulmonary edema
- Vasopressors: Norepinephrine for cardiogenic shock with hypotension
Devices and Surgical
- ICD (Implantable Cardioverter Defibrillator): EF ≤35% on optimal medical therapy ≥3 months; reduce SCD
- CRT (Cardiac Resynchronization Therapy): EF ≤35% + LBBB + QRS ≥150 ms; improves symptoms and mortality
- LVAD (Left Ventricular Assist Device): Bridge to transplant or destination therapy
- Cardiac transplantation: End-stage HF; EF <25%; refractory to maximal therapy
6. CARDIOMYOPATHY
Definition
Types
A. Dilated Cardiomyopathy (DCM)
- Most common type (~60% of cardiomyopathies)
- Definition: Ventricular dilation + systolic dysfunction (↓ EF) without known cause
- Causes: Idiopathic (most common), genetic (mutations in titin TTN, lamin LMNA, dystrophin DMD), alcohol, viral myocarditis (Coxsackie B, adenovirus, HIV), peripartum, anthracyclines (doxorubicin), trastuzumab, cocaine, selenium deficiency, thyroid disease, tachycardia-mediated
- Gross pathology: Dilated, flabby, globular heart; all 4 chambers enlarged; mural thrombi common
- Features: Systolic HF symptoms (dyspnea, fatigue, edema); LBBB; regurgitant murmurs (MR, TR); embolic events
- Management: Standard HFrEF quadruple therapy (ARNI/ACEi/ARB, beta-blocker, MRA, SGLT2i); anticoagulation if EF <35% + AF/thrombus; ICD/CRT; transplant for end-stage
B. Hypertrophic Cardiomyopathy (HCM)
- Definition: LV hypertrophy (usually asymmetric septal hypertrophy) without identifiable cause
- Genetics: Autosomal dominant; mutations in sarcomere proteins (β-myosin heavy chain MYH7, myosin binding protein C MYBPC3 - most common); familial in 40-60%
- Pathophysiology:
- Systolic anterior motion (SAM) of mitral valve → dynamic LVOT obstruction (in ~25%) → HCM with obstruction (HOCM)
- LV hypertrophy → diastolic dysfunction → ↑ filling pressures
- Myocyte disarray + fibrosis → arrhythmic substrate → sudden cardiac death
- Features: Most commonly asymptomatic; exertional dyspnea, angina, syncope (especially with Valsalva/exertion); sudden cardiac death (most common cause of SCD in young athletes); harsh systolic murmur at LLSB that increases with Valsalva/standing and decreases with squatting/passive leg raise
- Diagnosis: Echo = LV wall thickness ≥15 mm (or ≥13 mm with family history); cardiac MRI; genetic testing
- Management:
- Avoid dehydration, vasodilators, diuretics, digoxin, nitrates (worsen obstruction)
- Beta-blockers (first-line): ↓ HR → ↑ diastolic filling time → ↓ obstruction
- Disopyramide: Negative inotrope, reduces SAM/obstruction; combined with beta-blocker
- Verapamil/diltiazem: For beta-blocker intolerant
- Mavacamten (novel myosin inhibitor): FDA-approved for symptomatic obstructive HCM; reduces LVOT gradient
- Septal reduction: Surgical myectomy (gold standard) or alcohol septal ablation (catheter-based)
- ICD: SCD prevention for high-risk patients (prior arrest, family history of SCD, severe hypertrophy ≥30 mm, unexplained syncope, LVOT gradient ≥50, NSVT)
C. Restrictive Cardiomyopathy (RCM)
- Definition: Normal/near-normal LV size + function (EF preserved) but severely impaired filling (rigid walls) → ↑ filling pressures; resembles constrictive pericarditis
- Causes: Amyloidosis (most common; cardiac amyloid → thickened, sparkling walls on echo; ↓ voltage on ECG despite LVH), sarcoidosis, hemochromatosis, Fabry disease, glycogen storage diseases, eosinophilic endomyocardial disease (Loeffler), radiation-induced fibrosis
- Features: Dyspnea, fatigue, RHF signs (edema, ascites); normal or small LV; biatrial enlargement; normal or near-normal EF
- Diagnosis: Echo (biatrial enlargement, diastolic dysfunction, preserved EF); cardiac MRI (late gadolinium enhancement characterizes infiltrative patterns); biomarkers (BNP, troponin); biopsy if diagnosis unclear
- Management: Largely supportive; diuretics (cautiously); treat underlying cause; transthyretin amyloidosis: tafamidis (TTR stabilizer) - reduces mortality in ATTR amyloidosis (ATTR-ACT trial); patisiran (siRNA) or inotersen (antisense oligonucleotide) for hATTR; transplant for end-stage
D. Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC)
- Replacement of RV myocardium with fibrofatty tissue → RV dilation + dysfunction + arrhythmias
- Genetics: Desmosome mutations (plakophilin-2 PKP2, desmoglein, desmocollin)
- SCD risk in young athletes; epsilon wave on ECG; "stack of coins" sign on imaging; cardiac MRI diagnostic
- ICD + beta-blockers; avoid competitive sports
E. Other Cardiomyopathies
- Peripartum cardiomyopathy (PPCM): Develops in last month of pregnancy to 5 months postpartum; EF <45%; bromocriptine may accelerate recovery (blocks prolactin); high chance of recovery
- Stress cardiomyopathy (Takotsubo): Transient LV apical ballooning after emotional/physical stress; catecholamine surge; post-menopausal women; full recovery usual
- Tachycardia-induced cardiomyopathy: Reversible with rate control
7. PERICARDITIS
Definition
- Characteristic chest pain (sharp, pleuritic, positional - worse supine, better sitting forward)
- Pericardial friction rub
- Characteristic ECG changes
- New/worsening pericardial effusion
Types
- Acute pericarditis: <4-6 weeks
- Incessant pericarditis: >4-6 weeks but <3 months
- Recurrent pericarditis: Documented recurrence after symptom-free interval ≥4-6 weeks
- Chronic pericarditis: >3 months
- Pericardial effusion: Fluid accumulation in pericardial space
- Cardiac tamponade: Life-threatening compression of heart from pericardial effusion
- Constrictive pericarditis: Fibrotic/calcified pericardium → impaired cardiac filling
Causes
| Category | Examples |
|---|---|
| Idiopathic/Viral (most common) | ~80-90% in developed countries; enterovirus, coxsackie, echo, EBV, CMV, HIV |
| Bacterial | TB (most common worldwide cause of constrictive pericarditis), pneumococcus, staphylococcus, purulent pericarditis (severe) |
| Autoimmune | SLE, RA, systemic sclerosis, Dressler syndrome (post-MI), post-cardiac injury syndrome |
| Metabolic | Uremia (uremic pericarditis), hypothyroidism |
| Neoplastic | Malignant effusions: breast, lung, lymphoma, melanoma (most common cause of pericardial effusion) |
| Iatrogenic | Post-cardiac surgery, radiation therapy, cardiac procedures |
| Drug-induced | Hydralazine, procainamide (lupus-like), isoniazid, phenytoin |
Pathophysiology
- Intrapericardial pressure rises above intracardiac pressure
- Cardiac chambers compressed → ↓ ventricular filling → ↓ cardiac output → tamponade
Diagnostic Approach
| Test | Findings |
|---|---|
| ECG | Stage 1: Diffuse concave ST elevation + PR depression (saddle-shaped); Stage 2: ST normalizes; Stage 3: T-wave inversion; Stage 4: Normalization; absence of reciprocal ST depression (distinguishes from MI, except aVR and V1) |
| Echocardiography | Pericardial effusion; RV diastolic collapse (tamponade); respirophasic variation in mitral/tricuspid inflows |
| CXR | Enlarged cardiac silhouette if large effusion (>250 mL); "flask-shaped" heart on CXR |
| Cardiac MRI | Pericardial inflammation (gadolinium enhancement); constrictive pericarditis |
| Labs | ESR, CRP ↑; cardiac troponin ↑ (myopericarditis); CBC; TSH; ANA/RF (autoimmune screen); cultures; tuberculin test (TB) |
| Pericardiocentesis | Diagnostic + therapeutic; indicated for large effusion/tamponade; fluid analysis (LDH, protein, glucose, cytology, culture, ADA for TB) |
Management and Pharmacology
| Drug | Dose | Notes |
|---|---|---|
| Aspirin (first-line) | 750-1000 mg every 8 hrs × 2 weeks | With gastroprotection; evidence-based first choice |
| NSAIDs (ibuprofen preferred) | 600 mg every 8 hrs × 2 weeks | Alternative to aspirin; also celecoxib; avoid after MI (impair healing) |
| Colchicine | 0.5 mg BD (0.5 mg OD if <70 kg) × 3 months | COPPS and ICAP trials: ↓ recurrence by 50%; added to NSAID/aspirin |
| Corticosteroids | Prednisone 0.2-0.5 mg/kg/day then taper | Last resort (not first-line - ↑ recurrence risk); use in autoimmune, uremic, refractory pericarditis |
| Anakinra | IL-1 receptor antagonist | Recurrent/refractory pericarditis; especially with IL-1 mediated autoinflammatory disorders |
| Rilonacept | IL-1α/β blocker | FDA-approved for recurrent pericarditis (RHAPSODY trial) |
8. INFECTIVE ENDOCARDITIS (IE)
Definition
Types
By Clinical Course
- Acute IE: Rapid, fulminant course over days-weeks; S. aureus most common; previously normal valves can be affected
- Subacute IE (SBE): Indolent course over weeks-months; viridans streptococci most common; typically on previously damaged valves
By Valve Type
- Native valve endocarditis (NVE): Affects native heart valves
- Prosthetic valve endocarditis (PVE): Early (<60 days of surgery) - S. epidermidis, S. aureus; Late (>60 days) - similar to NVE
- IVDU-associated IE: Right-sided; tricuspid valve most common; S. aureus dominant; septic pulmonary emboli
Causes / Organisms
| Organism | Setting | Notes |
|---|---|---|
| Streptococcus viridans | Subacute NVE; dental procedures | Most common overall; oral flora |
| Staphylococcus aureus | Acute NVE/PVE; IVDU; healthcare-associated | Most virulent; leading cause in developed countries/hospitals |
| Staphylococcus epidermidis | PVE; nosocomial | Coagulase-negative staph |
| Enterococcus | GI/GU tract origin; elderly; healthcare | Difficult to treat; high-level aminoglycoside resistance |
| Streptococcus bovis (S. gallolyticus) | Associated with colonic polyps/cancer (must colonoscope) | |
| HACEK organisms | Subacute NVE; culture-negative initially | Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella |
| Candida/Aspergillus | PVE; immunocompromised; IVDU | Culture-negative; large friable vegetations |
| Coxiella burnetii (Q fever) | Serologic diagnosis; culture-negative |
Pathophysiology
- Bacteremia (from dental/GI/GU procedures, IV drug use, intravascular devices, skin infections) → bacteria seed damaged endothelium or normal endothelium (S. aureus)
- Endothelial injury (from turbulent flow in valvular disease, congenital defects) → fibrin-platelet thrombus formation (non-bacterial thrombotic endocarditis - NBTE) → colonization by bacteria during bacteremia
- Vegetation formation: Bacteria + fibrin + platelets accumulate → friable vegetations → progressive valve destruction
- Consequences:
- Local: Valve perforation, rupture, abscess formation, fistulae, conduction abnormalities (AV block from septal abscess)
- Embolic: Systemic emboli (stroke, renal/splenic infarcts, Janeway lesions) from left-sided IE; pulmonary emboli from right-sided IE
- Immunologic: Osler's nodes, Roth spots, glomerulonephritis (immune complex deposition)
Diagnostic Approach (Duke Criteria)
- Positive blood cultures: Typical organism in 2 separate cultures (S. viridans, S. bovis, HACEK, S. aureus, Enterococcus without primary focus); OR persistently positive cultures ≥12 hours apart; OR single positive culture for Coxiella
- Evidence of endocardial involvement: Positive echocardiography (vegetation, abscess, new valvular regurgitation) OR positive 18F-FDG PET/CT
- Predisposing heart condition or IVDU
- Fever >38°C
- Vascular phenomena: Arterial emboli, septic pulmonary infarcts, Janeway lesions, intracranial hemorrhage, conjunctival hemorrhage
- Immunologic phenomena: Glomerulonephritis, Osler's nodes, Roth spots, positive rheumatoid factor
- Microbiological evidence: Positive blood culture not meeting major criteria
| Sign | Description |
|---|---|
| Osler's nodes | Painful, raised, reddish nodules on finger/toe pads (immunologic - immune complex deposits) |
| Janeway lesions | Painless, flat, erythematous spots on palms/soles (embolic - septic emboli) |
| Roth spots | Oval retinal hemorrhages with pale center (immunologic) |
| Splinter hemorrhages | Linear hemorrhages under nails (embolic, also trauma) |
| Clubbing | In chronic IE |
| Petechiae | Conjunctival, oral mucosa |
| Test | Purpose |
|---|---|
| Blood cultures | 3 sets from 3 different sites before antibiotics; essential; aerobic + anaerobic |
| Echocardiography (TTE/TEE) | Vegetation (>2mm), abscess, valve perforation; TEE more sensitive than TTE (especially PVE) |
| CBC | Leukocytosis, anemia (of chronic disease) |
| ESR, CRP | Elevated |
| Urinalysis | Hematuria, proteinuria (glomerulonephritis) |
| Complement levels | Low C3, C4 (immune complex deposition) |
| Rheumatoid factor | Positive in 50% subacute IE |
| CT/MRI brain | Silent cerebral emboli (30-40% of IE) |
| 18F-FDG PET/CT | For PVE and device-related IE (newer major Duke criterion) |
Management and Pharmacology
Antibiotic Therapy (Empirical, then targeted)
- Native valve: Ampicillin + flucloxacillin + gentamicin (covers streptococci, staph, enterococci)
- Penicillin allergy: Vancomycin + gentamicin
- PVE/healthcare-associated: Vancomycin + gentamicin ± rifampicin
| Organism | Preferred Regimen | Duration |
|---|---|---|
| S. viridans, S. bovis (sensitive) | Benzylpenicillin 12-18 MU/day IV | 4 weeks (NVE); 6 weeks (PVE) |
| S. viridans (short course) | Benzylpenicillin + gentamicin | 2 weeks (uncomplicated NVE) |
| S. aureus MSSA | Flucloxacillin 2g IV every 4 hrs | 4-6 weeks |
| S. aureus MRSA | Vancomycin 15-20 mg/kg IV every 12 hrs (AUC-guided) | 6 weeks; add daptomycin (right-sided) |
| Enterococcus | Ampicillin + gentamicin (synergistic) | 4-6 weeks; 6 weeks PVE |
| PVE (empirical) | Vancomycin + gentamicin + rifampicin | ≥6 weeks |
| Culture-negative | Ceftriaxone + ampicillin; treat empirically for atypicals | |
| Candida | Amphotericin B or echinocandin (caspofungin) + flucytosine | ≥6 weeks; often indefinite suppression |
Surgical Indications for IE
- Urgent (emergency): Acute severe aortic or mitral regurgitation with hemodynamic instability; perivalvular abscess with fistula/septic pericarditis; uncontrolled infection
- Urgent (within days): Persisting bacteremia/fever >7-10 days despite appropriate antibiotics; large mobile vegetation with embolic events; S. aureus PVE
- Elective: PVE with significant valve dysfunction after completing antibiotics
IE Prophylaxis
- Prosthetic heart valves
- Previous IE
- Unrepaired cyanotic CHD
- Repaired CHD with prosthetic material (first 6 months)
- Cardiac transplant recipients with valvulopathy
- Amoxicillin 2g oral 30-60 min before procedure
- Clindamycin 600mg oral (if penicillin allergy)
- Ampicillin 2g IV/IM (if unable to take orally)
9. HYPERTENSION (HTN)
Definition
Classification
| Category | Systolic (mmHg) | Diastolic (mmHg) |
|---|---|---|
| Normal | <120 | <80 |
| Elevated (Prehypertension) | 120-129 | <80 |
| Stage 1 HTN | 130-139 | 80-89 |
| Stage 2 HTN | ≥140 | ≥90 |
| Hypertensive urgency | >180 | >120 (no end-organ damage) |
| Hypertensive emergency | >180 | >120 (WITH end-organ damage) |
Causes
Primary/Essential Hypertension
- Genetic predisposition + environmental factors
- High sodium intake, obesity (↑ RAAS + sympathetic activation), sedentary lifestyle, alcohol, stress
- Pathophysiology: ↑ CO + ↑ SVR; complex interplay of RAAS, SNS, endothelial dysfunction, renal Na+ handling
Secondary Hypertension
| Cause | Clues | Screening Test |
|---|---|---|
| Renovascular HTN (renal artery stenosis) | Young woman (FMD), atherosclerotic elderly, renal bruit, flash pulmonary edema, renal function deterioration with ACEi | Renal Doppler US, CT/MR angiography |
| Renal parenchymal disease (CKD) | Proteinuria, elevated creatinine | Urinalysis, serum creatinine, eGFR |
| Primary hyperaldosteronism (Conn's) | Hypokalemia, resistant HTN, adrenal adenoma | Aldosterone:renin ratio |
| Pheochromocytoma | Paroxysmal HTN, headache, sweating, palpitations | Plasma/urine catecholamines, metanephrines |
| Cushing's syndrome | Centripetal obesity, striae, proximal myopathy | 24-hr urinary free cortisol, overnight dexamethasone suppression |
| Coarctation of aorta | Upper limb HTN + weak femoral pulses; systolic murmur; rib notching on CXR | Echo, CT aortogram |
| Obstructive sleep apnea (OSA) | Obese, snoring, resistant HTN, morning headaches | Polysomnography |
| Thyroid/Parathyroid | Hypothyroidism, hyperthyroidism, hyperparathyroidism | TSH, Ca²⁺, PTH |
| Drugs | OCP, NSAIDs, decongestants, cocaine, steroids, ciclosporin, erythropoietin | Drug history |
Pathophysiology
Primary HTN
- Increased cardiac output: Sympathetic overactivity (↑ HR, ↑ contractility) + volume expansion (↑ Na retention)
- Increased peripheral vascular resistance: Endothelial dysfunction → ↓ NO → vasoconstriction; RAAS activation → Ang II → vasoconstriction + aldosterone → Na retention; structural vascular remodeling (smooth muscle hypertrophy of arterioles)
- RAAS overactivation: Key pathogenic pathway; Ang II causes vasoconstriction, Na retention, aldosterone release, cardiac and vascular remodeling
- Renal pressure-natriuresis curve: Shift to the right in essential HTN - kidney requires higher BP to excrete normal Na load
Target Organ Damage
| Organ | Pathology |
|---|---|
| Heart | LV hypertrophy (concentric) → diastolic dysfunction (HFpEF) → eventual systolic failure; ↑ IHD risk; AF |
| Brain | Hypertensive encephalopathy; lacunar infarcts (small vessel disease); ICH; hypertensive retinopathy (AV nipping, flame hemorrhages, papilledema) |
| Kidney | Nephrosclerosis → arteriolar thickening → glomerular ischemia → CKD; proteinuria |
| Aorta | Aortic dissection; aortic aneurysm |
| Eyes | Hypertensive retinopathy (Keith-Wagener-Barker classification Grade I-IV) |
| Peripheral vessels | PAD; accelerated atherosclerosis |
Diagnostic Approach
| Test | Purpose |
|---|---|
| BP measurement | Properly done; seated, both arms, average of 2 readings; ABPM for white coat HTN confirmation |
| Urinalysis + urine ACR | Proteinuria (renal damage, glomerulonephritis) |
| Serum creatinine + eGFR | CKD |
| Serum electrolytes | K+ (low = Conn's, diuretics; high = ACEi+CKD); Na+ |
| Fasting glucose + HbA1c | DM (major CV risk factor) |
| Lipid profile | CVD risk assessment |
| ECG | LVH (voltage criteria: Sokolow-Lyon > 35 mm), strain pattern |
| CXR | Cardiomegaly, pulmonary congestion, coarctation (rib notching) |
| Echocardiography | LV mass/hypertrophy, diastolic function, LVEF |
| Fundoscopy | Hypertensive retinopathy staging |
| Secondary screening (when suspected) | ARC ratio (Conn's), metanephrines (pheo), TSH, renal US, overnight dexamethasone test |
Management
Non-Pharmacological (All stages)
- Weight loss: Each 1 kg → ~1 mmHg ↓ SBP
- DASH diet (Dietary Approaches to Stop Hypertension): Rich in fruits, vegetables, low-fat dairy, limited sodium → ↓ SBP 8-14 mmHg
- Sodium restriction: <2 g/day → ↓ SBP 2-8 mmHg
- Physical activity: ≥150 min/week moderate aerobic exercise → ↓ SBP 4-9 mmHg
- Alcohol reduction: ≤2 drinks/day men, ≤1 women → ↓ SBP 2-4 mmHg
- Smoking cessation: Reduces overall CV risk (not directly BP)
Pharmacological Treatment
- General: <130/80 mmHg (ACC/AHA); <140/90 mmHg (ESC/NICE)
- CKD + proteinuria: <130/80 mmHg
- Diabetes: <130/80 mmHg
- Elderly (>65-80 yr): <130/80 mmHg if tolerated; avoid symptomatic hypotension
First-Line Drug Classes
| Class | Examples | Mechanism | Compelling Indications |
|---|---|---|---|
| ACE inhibitors | Ramipril, lisinopril, enalapril, perindopril | ↓ Ang II → vasodilation + ↓ aldosterone → natriuresis; ↑ bradykinin | DM/CKD with proteinuria, post-MI, HFrEF, LVH, CAD |
| ARBs | Losartan, valsartan, olmesartan, telmisartan | Ang II type 1 receptor blockade | Same as ACEi; better tolerated (no cough/angioedema) |
| Calcium Channel Blockers (CCB) - Dihydropyridines | Amlodipine, felodipine, nifedipine | Block L-type Ca²⁺ channels in vascular smooth muscle → vasodilation | Elderly, isolated systolic HTN, Black patients, angina, Raynaud's |
| CCB - Non-dihydropyridines | Diltiazem, verapamil | Ca²⁺ block + rate control | Angina, AF rate control; avoid in HFrEF |
| Thiazide diuretics | Hydrochlorothiazide (HCTZ), chlorthalidone, indapamide | ↑ Na+/Cl- excretion → ↓ plasma volume → ↓ CO; long-term: vasodilation | Elderly, isolated systolic, Black patients, osteoporosis, HF |
| Beta-blockers | Atenolol, bisoprolol, metoprolol, carvedilol, nebivolol | ↓ HR, ↓ CO, ↓ renin release | Post-MI, angina, HFrEF, tachyarrhythmias; NOT first-line for uncomplicated HTN (more strokes vs. other agents in elderly) |
Second/Third-Line Agents
| Drug | Class | Notes |
|---|---|---|
| Spironolactone | Aldosterone antagonist | Excellent for resistant HTN (4th agent); Conn's syndrome |
| Doxazosin | α1-blocker | Resistant HTN; BPH co-existing |
| Hydralazine | Direct arteriolar vasodilator | Pregnancy HTN; IV in hypertensive emergencies |
| Methyldopa | Central α2 agonist | Drug of choice in pregnancy HTN |
| Clonidine | Central α2 agonist + imidazoline receptor | Resistant HTN; caution: rebound HTN on withdrawal |
| Moxonidine | Imidazoline I1 receptor agonist | Resistant HTN, metabolic syndrome |
| Minoxidil | K+ATP channel opener → arteriolar dilation | Severe resistant HTN; reflex tachycardia + hirsutism |
| Aliskiren | Direct renin inhibitor | Rarely used; contraindicated with ACEi/ARB |
Special Situations
| Condition | Preferred Agent |
|---|---|
| Hypertensive emergency | IV labetalol, nicardipine, hydralazine, sodium nitroprusside; aim for 20-25% SBP reduction in 1st hour |
| Hypertensive encephalopathy | IV labetalol or nicardipine |
| Aortic dissection | IV esmolol (beta-blocker first) + vasodilator; target SBP <120 mmHg, HR <60 |
| Acute pulmonary edema | IV nitrates (GTN) + loop diuretics + CPAP |
| Eclampsia/Pre-eclampsia | IV hydralazine, IV labetalol, oral nifedipine; MgSO₄ for seizures |
| STEMI with HTN | IV nitroglycerin; beta-blockers (if not in shock) |
| CKD with proteinuria | ACEi or ARB (renoprotective) |
| Diabetes mellitus | ACEi or ARB (reduce proteinuria) |
| Pregnancy | Methyldopa (first choice), labetalol, nifedipine; AVOID ACEi/ARB (teratogenic) |
| Primary aldosteronism | Spironolactone or eplerenone; surgery (adrenalectomy for unilateral adenoma) |
| Pheochromocytoma | Alpha-blocker first (phenoxybenzamine), THEN beta-blocker; NEVER beta-blocker alone (hypertensive crisis) |
| Renovascular | ACEi/ARB (caution in bilateral RAS); revascularization (stenting/surgery) |
Resistant Hypertension
- Non-adherence (most common)
- White coat effect → ABPM
- Secondary causes (especially primary aldosteronism)
- Interfering medications (NSAIDs, OCP, decongestants)
- Robbins, Cotran & Kumar - Pathologic Basis of Disease (pp. 496-530)
- Goldman-Cecil Medicine, International Edition (Chapters 45, 64, 114)
- Tintinalli's Emergency Medicine (pp. 862-870, 3183-3192)
- Textbook of Family Medicine, 9th Edition (p. 698)
- Fuster and Hurst's The Heart, 15th Edition
- Robbins & Kumar Basic Pathology (pp. 363, 659)
- Lippincott Illustrated Reviews: Pharmacology
- Braunwald's Heart Disease, 2-Volume Set
provide defenition, types, causes, pathology, diagnostic approach , management along with pharmacology for anaemias
What Was Covered
| Section | Types Covered |
|---|---|
| Definition | WHO thresholds by sex/age; severity grading |
| Classification | By MCV (micro/normo/macrocytic) AND by pathophysiology (underproduction / haemolysis / blood loss) |
| 1. Iron Deficiency Anaemia | Causes (blood loss, diet, malabsorption, demand), hepcidin pathway, stages, morphology, Plummer-Vinson, Pica, diagnostic labs table |
| 2. Megaloblastic Anaemia | B12 vs folate: physiology, causes (pernicious anaemia, gastrectomy, vegans, Crohn's, drugs), methyl-folate trap, subacute combined degeneration, hypersegmented neutrophils, MMA vs homocysteine distinction |
| 3. Anaemia of Chronic Disease | Hepcidin-central model, IL-6 pathway, differentiation from IDA (ferritin key) |
| 4. Aplastic Anaemia | Causes (chloramphenicol, benzene, Fanconi), T-cell mechanism, Camitta criteria, bone marrow biopsy, hATG + cyclosporin + eltrombopag protocol |
| 5a-5g. Haemolytic Anaemias | HS (spectrin/ankyrin, osmotic fragility, EMA test), G6PD (Heinz bodies, triggers, favism), SCD (vaso-occlusion, acute chest syndrome, hydroxyurea/voxelotor/crizanlizumab), Thalassaemias (α and β; luspatercept; deferasirox), Warm/Cold AIHA (Coombs test, rituximab), PNH (eculizumab), MAHA/TTP/HUS (plasma exchange, caplacizumab) |
| Diagnostic Algorithm | Step-by-step MCV → reticulocyte → targeted workup |
| Summary Table | All types side-by-side: MCV, reticulocytes, ferritin, smear findings, DAT |
| Pharmacology Table | 20+ drugs with mechanism, route, key notes |