Loose stools x 30 episodes since yesterday evening with foul smell ,history of umbilical hernia repair on 13 may , no fever no vomiting.pt is very dehydrated
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
post-operative diarrhea Clostridioides difficile hernia repair
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information to provide a complete clinical answer. Let me compile the full response.
Clinical Assessment: Post-Operative Diarrhea with Severe Dehydration
Key clinical context: 30 loose, foul-smelling stools since yesterday evening, umbilical hernia repair on 13 May (19 days ago), no fever, no vomiting, severely dehydrated.
Differential Diagnosis
1. Clostridioides difficile Infection (CDI) - Top Priority
This is the leading concern given the post-surgical context. Surgery patients are at high risk because they are typically:
- Recently hospitalized
- Exposed to perioperative antibiotics
- Relatively immunosuppressed post-operatively
Per Sabiston's Surgery: "Most patients develop watery diarrhea during antibiotic therapy or shortly after a course of antibiotics but can also present weeks later." The 19-day window fits perfectly. The foul odor is classic for CDI.
CDI stool testing criteria are met: 3+ loose stools in 24 hours. The organism produces Toxin A and Toxin B causing colitis ranging from mild watery diarrhea to fulminant pseudomembranous colitis.
2. Acute Infectious Gastroenteritis
- Viral (norovirus, rotavirus) or bacterial (Salmonella, Campylobacter, E. coli) causes
- Can occur independent of the surgical history
- Foul smell may suggest bacterial etiology
3. Post-Operative Gut Dysmotility / Altered Microbiome
- Surgery disrupts normal gut flora and motility
- Bowel preparation or enteral feeding changes can contribute
4. Less likely (no fever, no blood in stool)
- Mesenteric ischemia (no fever but monitor closely given recent surgery)
- Inflammatory bowel disease flare
Immediate Assessment and Red Flags to Check
Severity markers for CDI to assess NOW:
- Leukocytosis (WBC >15,000) - marker of severe CDI
- Creatinine elevation - >1.5x baseline suggests severe disease
- Hypotension / shock - indicates fulminant CDI
- Abdominal distension / tenderness - suggests toxic megacolon
- Temperature (no fever now, but monitor)
Dehydration assessment:
| Parameter | Mild | Severe |
|---|---|---|
| Appearance | Thirsty, restless | Lethargic, floppy |
| Skin turgor | Reduced | Very reduced |
| Eyes | Slightly sunken | Deeply sunken |
| Mucous membranes | Dry | Very dry |
| BP | Normal | Hypotension |
| Urine output | Reduced | Oliguria/anuria |
Immediate Management
Step 1: IV Fluid Resuscitation (PRIORITY - patient is "very dehydrated")
Since the patient is severely dehydrated with 30 episodes of fluid loss, oral rehydration is insufficient at this stage.
- IV normal saline (0.9% NaCl) or Ringer's Lactate - start immediately
- Give 20 mL/kg bolus and reassess; repeat as needed
- Add potassium supplementation (significant K+ loss with diarrhea)
- Check serum electrolytes, BUN/creatinine, CBC
- Target: urine output >0.5 mL/kg/hr
Per Yamada's Gastroenterology: "The most important part of the clinical assessment of such patients is their fluid status followed by treatment of hypovolemia and electrolyte disturbances. Severely dehydrated patients require intravenous fluid."
Step 2: Send Stool Investigations
- C. difficile stool test - NAAT/PCR (most sensitive) + Toxin EIA (confirms active disease)
- A two-step approach (GDH + Toxin EIA, arbitrated by NAAT) is preferred
- Stool culture and sensitivity - for bacterial pathogens
- Stool microscopy - ova, cysts, parasites (if indicated)
- Stool for fecal leukocytes/lactoferrin
- Do NOT delay treatment if clinical suspicion for CDI is high
Step 3: Bloods
- CBC (look for leukocytosis), CMP (electrolytes, creatinine, albumin)
- Blood cultures if systemic signs develop
- Lactate if hemodynamically unstable
Step 4: Empirical CDI Treatment (start if strong suspicion)
Per Harrison's (2025) and IDSA/SHEA 2021 guidelines:
Do NOT use antiperistaltic agents (loperamide, etc.) if CDI is suspected - they can mask worsening disease.
Discontinue any ongoing antibiotics if possible (this alone resolves 15-23% of mild CDI cases).
First-line drugs (IDSA 2021 guidelines):
- Fidaxomicin 200 mg orally twice daily x 10 days - preferred (lower recurrence rate vs vancomycin)
- Vancomycin 125 mg orally four times daily x 10 days - acceptable alternative (oral only; IV vancomycin is ineffective for CDI)
- Metronidazole 500 mg orally three times daily x 10 days - only if fidaxomicin and vancomycin unavailable; not recommended as first-line
If fulminant CDI (hypotension, shock, toxic megacolon, ileus):
- Vancomycin 500 mg orally/NG four times daily PLUS IV metronidazole 500 mg three times daily
- Consider vancomycin enemas (500 mg in 100 mL NS per rectum)
- Surgical consult
Monitoring and Red Flags for Deterioration
Watch closely for:
- Abdominal distension (toxic megacolon - cecal diameter >12 cm on imaging)
- Hemodynamic instability - escalate to ICU
- Worsening acidosis, rising lactate
- Peritonitis signs - may require emergency surgery
- Ileus (no bowel sounds + distension)
Imaging if deteriorating:
- Abdominal X-ray - rule out toxic megacolon
- CT abdomen with contrast - colonic wall thickening, accordion sign in severe CDI
Infection Control (if CDI confirmed or suspected)
- Isolate in single room with contact precautions
- Gloves + gown for all healthcare providers
- Soap and water handwashing (NOT alcohol gel - CDI spores are alcohol-resistant)
- Sporicidal disinfectant for room cleaning
- Separate toilet
Summary Table
| Action | Priority |
|---|---|
| IV fluid resuscitation (NS or RL) | IMMEDIATE |
| Bloods: CBC, CMP, lactate | Urgent |
| Stool: CDI toxin + culture | Urgent |
| Empirical CDI treatment (Vancomycin or Fidaxomicin) | Start if strong suspicion |
| Avoid antiperistaltics, opiates | Mandatory |
| Contact isolation | Now |
| Surgical consult if fulminant signs | If deteriorating |
Sources:
- Sabiston Textbook of Surgery, CDI section
- Harrison's Principles of Internal Medicine 22E (2025), IDSA/SHEA 2021 CDI guidelines
- Sleisenger & Fordtran's GI and Liver Disease, Ch. 112
- Yamada's Textbook of Gastroenterology, Acute Diarrhea Treatment
- Rosen's Emergency Medicine, Diarrhea chapter
Female 35 year old complaining of chest pain, ecg tall t waves in v1 to v6 ,bp 140/90 pr normal ,hb 9 ,history of gastritis 2d echo done which is normal
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information to give a detailed, well-structured clinical response. Let me synthesize everything.
Clinical Assessment: 35F - Chest Pain + Tall T Waves V1-V6
Summary of findings: 35-year-old female, chest pain, tall T waves across precordial leads V1-V6, BP 140/90, PR normal, Hb 9 g/dL (anemia), history of gastritis, normal 2D echo.
ECG Interpretation: Tall T Waves V1-V6 - Differential Diagnosis
The finding of tall T waves across all precordial leads (V1-V6) is a red flag pattern that must be worked through systematically. Per Rosen's Emergency Medicine, the differential for tall T waves includes:
"Hyperacute T waves of acute ischemia, hyperkalemia, benign early repolarization (BER), LVH, LBBB, and acute pericarditis."
And per Harrison's 2025:
"Tall T waves do not invariably represent hyperacute ischemic changes but may also be caused by normal variants, hyperkalemia, or cerebrovascular injury."
1. Hyperacute T Waves of Anterior STEMI / LAD Occlusion - MUST RULE OUT FIRST
This is the most dangerous cause and must be excluded urgently. The hyperacute T wave:
- Appears within minutes of coronary occlusion - it is the earliest ECG sign of STEMI
- Tall, broad-based, asymmetrical T waves with ST elevation beginning at J-point
- Typically progresses to frank ST elevation over 30-60 minutes
- V1-V6 involvement = anterior wall territory = proximal LAD occlusion
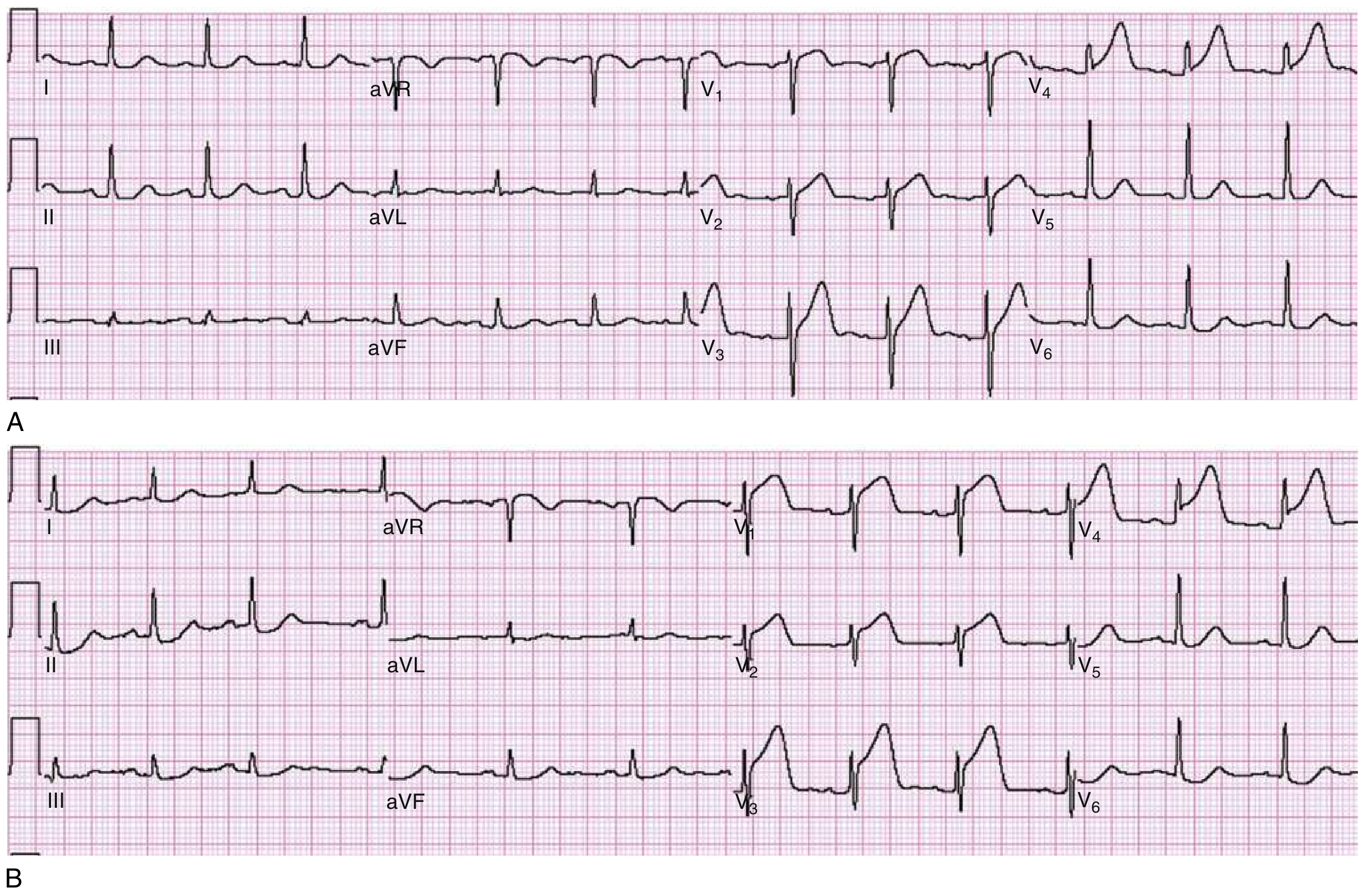
Panel A shows hyperacute broad tall T waves in V3-V4 with early ST rise. Panel B (same patient 30 min later) shows frank ST elevation in V1-V4 - classic STEMI evolution.
Normal echo does NOT rule out STEMI - wall motion abnormalities may not yet be detectable in the very early phase, and the echo may have been done before ischemic changes fully developed.
2. Type 2 MI due to Demand Ischemia - Highly Relevant Here
This patient has two compounding factors that can cause myocardial ischemia WITHOUT a ruptured plaque (Type 2 MI):
Per Harrison's 2025 (Table on troponin elevation causes):
- Severe anemia (Hb 9) - reduces oxygen delivery to myocardium
- Hypertension (BP 140/90) - increases myocardial oxygen demand / afterload
"Unstable ischemic symptoms may also occur predominantly because of increased myocardial oxygen demand or because of decreased oxygen delivery due to anemia, hypoxia, or hypotension."
Hb of 9 g/dL constitutes moderate anemia. Combined with hypertension and a normal heart rate (no compensatory tachycardia noted), the myocardium may be facing significant oxygen supply-demand mismatch, particularly in the subendocardium of the anterior wall.
3. Hyperkalemia - Must Rule Out Urgently
Classic ECG progression per Harrison's:
- K+ 5.5-6.5 mEq/L: tall peaked T waves (first ECG change)
- K+ 6.5-7.5 mEq/L: loss of P waves, widened QRS
- K+ >7.5 mEq/L: sine wave pattern, VF risk
Tall T waves from hyperkalemia tend to be narrow, symmetric, and "tented" (tent-peaked) - diffuse across all leads. If P waves are normal and QRS is normal, hyperkalemia is still possible at early stages.
Check serum potassium immediately - this is life-threatening and easily missed.
4. Benign Early Repolarization (BER)
- Common in younger patients, but more common in males
- Concave ST elevation with tall T waves, typically in precordial leads
- Not a diagnosis of exclusion in a symptomatic patient with chest pain - always rule out ischemia first
5. Other Causes to Consider
- Acute myocarditis - chest pain, ECG changes, normal echo early on; associated with elevated troponins; viral illness history?
- Pericarditis - usually sharp pleuritic pain; diffuse saddle-shaped ST elevation more typical
- Cerebrovascular injury (subarachnoid hemorrhage) - can cause massive diffuse T wave changes; check for headache
- LBBB - causes tall T waves in V1-V2; but changes morphology of QRS too
- Takotsubo (Stress) Cardiomyopathy - more common in postmenopausal women under stress; echo usually shows apical ballooning (not expected to be normal)
Management Plan
IMMEDIATE - Do NOW (treat as ACS until proven otherwise)
1. Serial ECGs - every 15-30 minutes
The hyperacute T wave is transient - it progresses to ST elevation within minutes to hours. A dynamic change is the key distinguishing feature of STEMI vs other causes. Static unchanged ECG over 1-2 hours reduces likelihood of acute coronary occlusion.
2. High-sensitivity Troponin (hsTnI or hsTnT)
- Draw at presentation (T=0) and repeat at 1 hour (1-hour algorithm) or 3 hours
- A rise and fall pattern (dynamic change) = myocardial injury/NSTEMI
- Elevated troponin + tall T waves = treat as ACS until proven otherwise
- Elevation can also occur in Type 2 MI (anemia + HTN driven)
3. Serum Electrolytes - STAT
- Potassium (hyperkalemia)
- Sodium, calcium, magnesium
- Renal function (creatinine, BUN) - renal failure causes hyperkalemia
4. CBC Confirmation
- Confirm Hb 9, look at MCV (type of anemia), RDW
- Anemia workup if not already done (iron studies, B12, folate)
5. Other Bloods
- ABG (if respiratory compromise)
- Blood glucose
- CXR (cardiomegaly, pulmonary edema, mediastinal widening)
If STEMI Is Confirmed (ST elevation develops):
- Activate catheterization lab immediately - door-to-balloon time <90 min
- Aspirin 300 mg loading dose + P2Y12 inhibitor (ticagrelor or clopidogrel)
- Anticoagulation (heparin)
- Avoid NSAIDs (history of gastritis - use PPI cover)
For the Anemia (Hb 9):
- Do NOT transfuse empirically without understanding cause
- If active ischemia confirmed, a threshold of Hb <8-9 may warrant transfusion to improve oxygen delivery
- Investigate: Iron studies, peripheral smear, reticulocyte count
- If iron deficiency anemia - IV iron therapy once cardiac cause addressed
For Hypertension (BP 140/90):
- Do not aggressively lower BP acutely until ischemia is ruled out
- If STEMI confirmed - standard ACS protocol
- If non-ischemic: investigate secondary causes (given young age, female, anemia)
For Gastritis History:
- If antiplatelet therapy is needed (ACS) - add PPI (omeprazole/pantoprazole) to prevent GI bleed
- Investigate if gastric blood loss is contributing to anemia (H. pylori testing, endoscopy)
Diagnostic Algorithm Summary
Tall T waves V1-V6 + Chest pain
↓
Serial ECGs (q 15-30 min)
↓
Dynamic change (ST elevation evolves)?
YES → STEMI protocol, activate cath lab
NO ↓
Check serum K+ → If elevated → treat hyperkalemia
Check hsTroponin (0h, 1h)
RISE/FALL → Type 1 or Type 2 MI
NORMAL × 2 → Lower risk, further workup
↓
Consider: myocarditis, pericarditis, BER, Takotsubo
Investigate: anemia cause, ECHO (serial if needed)
Key Concern Summary
| Priority | Finding | Action |
|---|---|---|
| URGENT | Tall T waves V1-V6 | Serial ECGs, dynamic change = STEMI |
| URGENT | Hyperkalemia exclusion | Serum K+ STAT |
| URGENT | Troponin | hsTn at 0h and 1h |
| Important | Hb 9 + HTN | Type 2 MI mechanism, investigate anemia cause |
| Important | Gastritis Hx | PPI if antiplatelet needed; H. pylori / endoscopy |
| Monitor | Normal echo | Does NOT exclude early ischemia |
Sources:
- Rosen's Emergency Medicine - ECG Abnormalities in Acute Coronary Syndromes
- Harrison's Principles of Internal Medicine 22E (2025) - Myocardial Ischemia/Injury, Table on Troponin Elevation Causes, NSTE-ACS Risk Stratification
- Miller's Anesthesia - Myocardial Oxygen Supply and Demand
This is a shared conversation. Sign in to Orris to start your own chat.