Renal stones surgery mbbs topic
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive MBBS-level answer. Here is the full compiled topic:
Renal Stones (Urolithiasis) - Surgery MBBS
Sources: Bailey & Love's Short Practice of Surgery 28th Ed., Schwartz's Principles of Surgery 11th Ed., Campbell-Walsh-Wein Urology
1. Introduction & Epidemiology
Urolithiasis is as old as mankind - the first documented cystolithotomy was performed by Sushruta (~600 BCE). It remains a major surgical problem with increasing incidence of renal calculi in the modern world (though bladder stones have declined due to improved nutrition).
- Lifetime prevalence: 1-20% (varies by geography)
- Recurrence: ~50% within the first decade of diagnosis
- Sex: Men are twice as likely as women to form stones
- Peak age: Men - 4th to 6th decade; Women - bimodal (3rd decade + postmenopausal)
- Ethnicity: White > other groups (though diet/environment may matter more)
- Family history: 2.5x increased risk
2. Pathogenesis
Stone formation is a cascade of events:
- Concentration of culprit salts (Ca²⁺, oxalate) overwhelms inhibitors (citrate, Tamm-Horsfall mucoprotein, magnesium, K⁺)
- Crystals precipitate and nucleate
- Crystal nuclei either wash away or anchor at Randall's plaques on renal papillae
- Urine pH matters: acidic urine → uric acid stones; alkaline urine → calcium phosphate stones
- Stasis promotes formation of smooth, round "milk of calcium stones"
3. Types of Renal Stones
| Stone Type | Frequency | Key Features |
|---|---|---|
| Calcium oxalate | 60-85% | Most common; associated with hypercalciuria, hyperoxaluria, hypocitraturia |
| Calcium phosphate | Rare (pure) | Apatite (infection), Brushite (distal RTA) |
| Struvite (infection) | ~15% | Urease-producing bacteria (Proteus, Klebsiella, Serratia); forms staghorn calculi |
| Uric acid | ~5-10% | Acidic urine; associated with gout, myeloproliferative disorders |
| Cystine | ~1% | Autosomal recessive cystinuria; very hard, resistant to SWL |
Staghorn Calculi
Infection stones growing in a branching pattern that fills the entire pelvicalyceal system. They can grow very large before detection, causing significant morbidity including loss of renal function from chronic infection and obstructive uropathy. Complete clearance is mandatory - residual fragments cause rapid recurrence. Long-term chemoprophylaxis is required after removal.
4. Clinical Presentation
- Ureteric/renal colic: Most common acute presentation - sudden onset excruciating flank pain radiating to groin, scrotum, or labia; caused by hyperperistalsis against the obstructing stone
- Haematuria: Gross or microscopic (especially during colic episodes)
- Calculuria: Passage of sand or gravel in urine
- Lower ureteric stones: Urinary urgency and frequency (near vesico-ureteric junction)
- Asymptomatic: Increasingly common with widespread imaging
- Sepsis: High-grade fever with chills = urological emergency requiring immediate decompression
5. Investigations
| Investigation | Role |
|---|---|
| NCCT (Non-contrast CT) | Investigation of choice - detects both radio-opaque AND radiolucent stones (exception: indinavir stones) |
| KUB X-ray + USG | Good first-line tests |
| Urinalysis | Microscopic haematuria, pyuria, crystals, pH |
| Urine culture | Before definitive surgery; if sepsis suspected |
| Serum Ca²⁺, phosphate, uric acid | Rule out hypercalcaemia, hypophosphataemia, hyperuricaemia |
| Serum electrolytes, creatinine | Renal function baseline |
6. Management Algorithm
Step 1 - Conservative / Medical
Watchful waiting: Small (<5 mm), non-obstructive, asymptomatic stones may be followed up.
- Up to 90% of 4-mm stones pass spontaneously
- Up to 50% of 6-10 mm stones pass spontaneously
- Observation period: 4-6 weeks for ureteral stones ≤10 mm
Medical Expulsive Therapy (MET):
- Tamsulosin (α1-blocker) - relaxes distal ureteric smooth muscle; used for distal ureteric stones >5 mm and to assist passage after SWL
- α-blockers improve stone passage rate from 54% → 77% for distal ureteral stones ≤10 mm (per meta-analyses)
- Calcium channel blockers - reduce dysmotile ureteric contractions
Analgesia: NSAIDs first-line; opioids if required
Emergency Decompression (if sepsis, obstruction, or refractory pain):
- Ureteric stenting (JJ stent) OR
- Percutaneous nephrostomy (PCN)
7. Surgical Management
Key principle: Choose the least invasive method appropriate for that particular stone.
Open surgery is now of historic interest only - <1% of stone surgery requires open access with modern endourology.
A. Extracorporeal Shockwave Lithotripsy (ESWL / SWL)
- Introduced in 1980 by Christian Chaussy - first non-invasive stone treatment
- Completely non-invasive outpatient procedure
Mechanism: Stone localised by fluoroscopy/USG → acoustic pulse waves focused on stone → fragmentation by mechanical stress from shockwave + cavitation bubble collapse
Indications:
- Proximal ureteral stones (especially <10 mm)
- Non-lower-pole renal stones <2 cm
Contraindications:
- Pregnancy
- Bleeding diathesis/anticoagulation
- Untreated UTI
- Aortic/renal artery aneurysm
- Uncorrected obstruction distal to stone
- Morbid obesity (stone unreachable)
- Pacemaker (relative)
Complications:
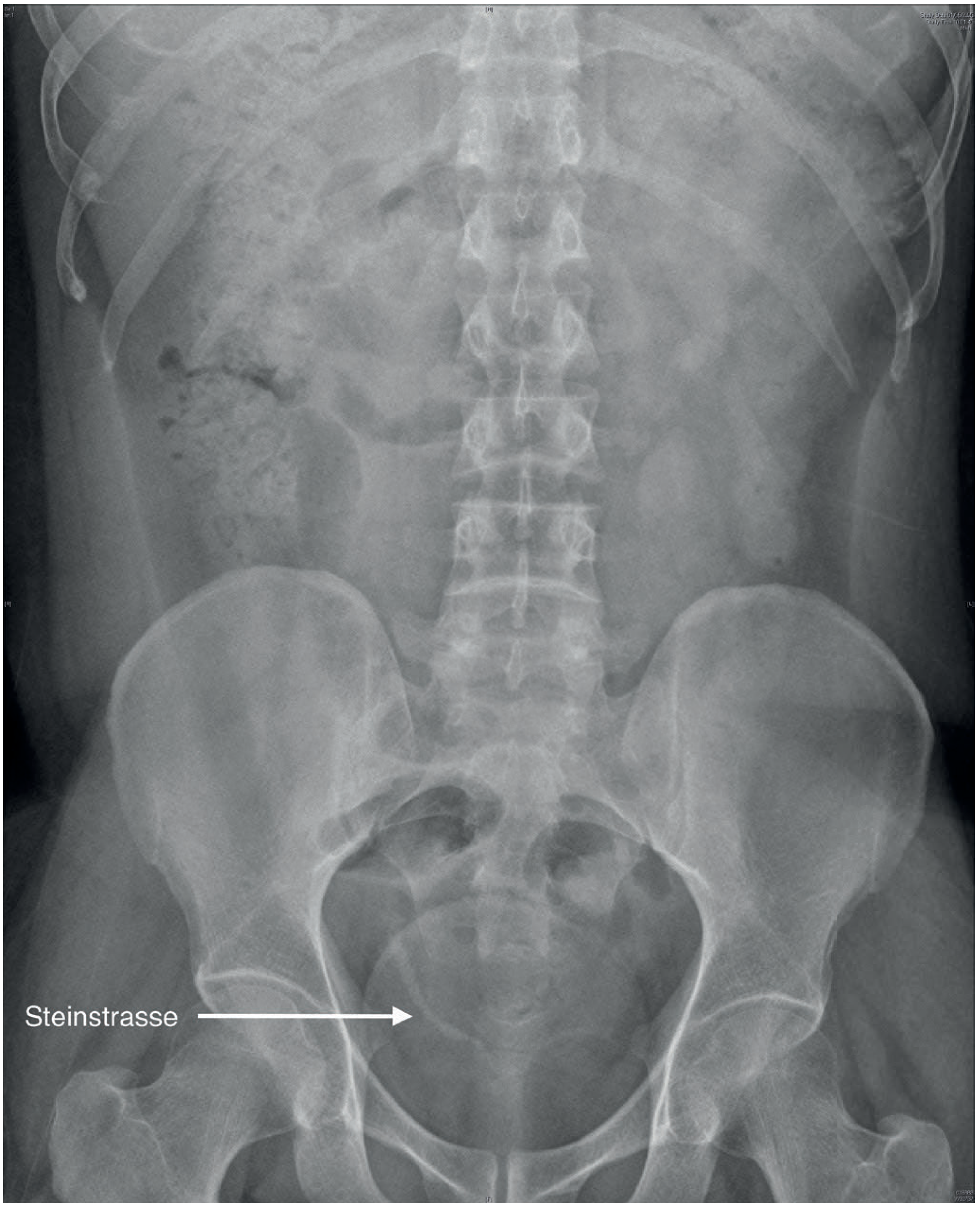
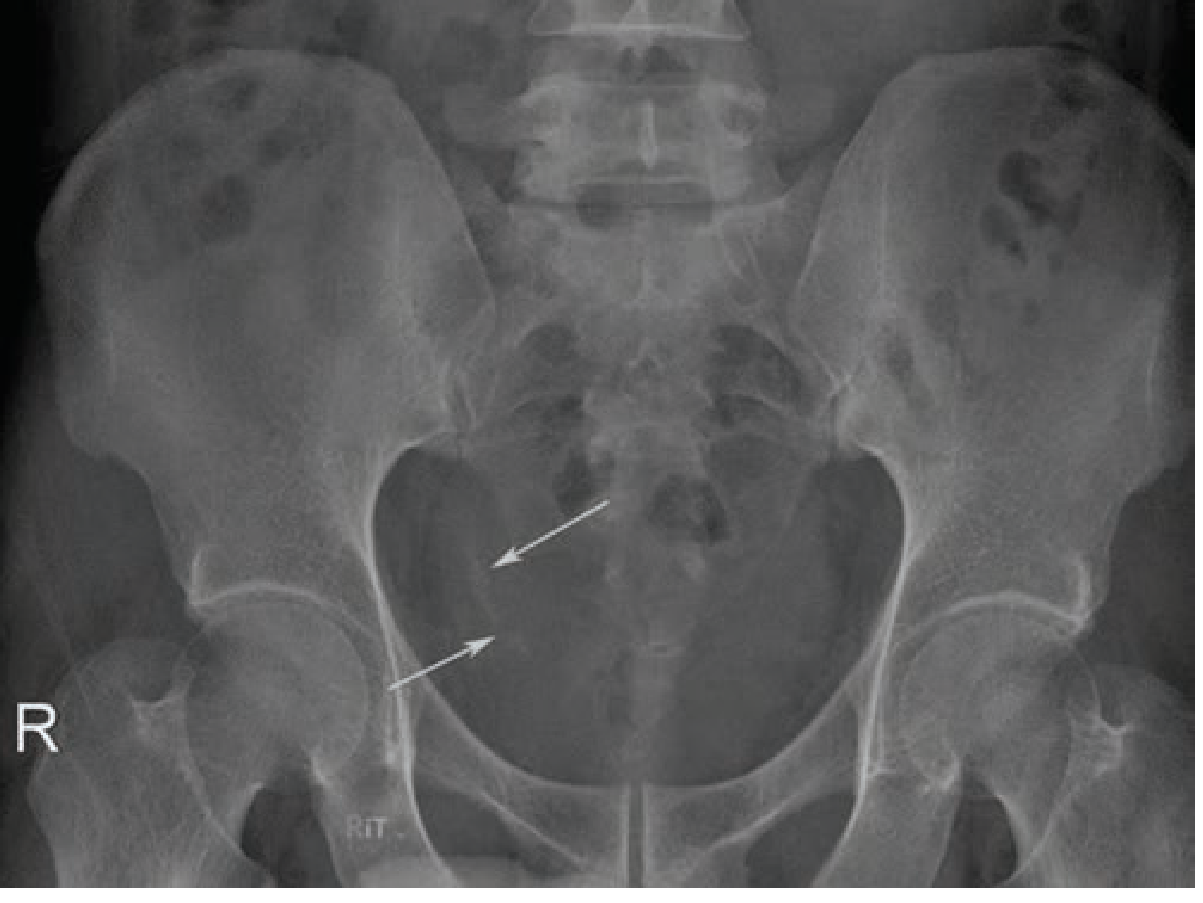
- Steinstrasse ("street of stones") - row of stone fragments lining the distal ureter, may cause obstruction; usually pass spontaneously, but may need intervention
- Subcapsular/perinephric hematoma
- "Clinically insignificant residual fragments" (≤4 mm) - expected to pass but 20-40% do not and can become a nidus for regrowth
B. Ureteroscopy (URS) / Ureterorenoscopy
Ureterorenoscopes (semirigid or flexible) are long thin scopes with working channels for energy sources, graspers, and baskets.
Indications:
- Middle and distal ureteral stones (procedure of choice)
- Proximal ureteral stones >10 mm (higher success than SWL)
- Renal stones (flexible URS)
Energy sources used for lithotripsy:
- Pneumatic lithotripter (semirigid URS)
- Holmium:YAG laser - most widely used, can be delivered via flexible instruments
Steps: Ureteroscope advanced to stone → fragmented under direct vision → fragments removed with nitinol basket OR left to pass
Post-procedure: JJ ureteric stent usually placed (major source of patient morbidity, though temporary)
Complications:
- Ureteric perforation
- Ureteric avulsion (avoided by careful basket use under vision)
- Ureteric stricture (long-term)
- Retropulsion of stone
Advantage over SWL: Surgeon can visualise fragmentation and control fragment size; active stone removal possible
C. Retrograde Intrarenal Surgery (RIRS)
A slimmer, flexible URS with active tip deflection + laser technology provides retrograde access to kidney via the ureteric orifice. Avoids morbidity of PCNL.
Indications:
- Renal stones <2 cm
- Lower pole calculi
- Obesity
- Musculoskeletal deformities (kyphoscoliosis)
- Renal anomalies (horseshoe kidney, pelvic kidney)
- Bleeding diathesis
D. Percutaneous Nephrolithotomy (PCNL)
PCNL involves creating a tract between the skin and the pelvicalyceal system for direct access to large renal stones.
Position: Prone (standard); supine (modified - Valdivia position)
Access: Fluoroscopy or USG guidance; posterolateral calyx is the preferred entry point
Steps:
- Needle access into selected calyx under imaging guidance
- Guidewire insertion
- Serial dilatation to create a working tract (typically 24-30Fr)
- Nephroscope introduced
- Stone fragmented using pneumatic + ultrasound lithotripter or laser
- Fragments removed with graspers
- Nephrostomy tube left in situ (or "tubeless PCNL" in selected cases)
Energy sources: Pneumatic, ultrasound (most common combination for PCNL), laser
Indications for PCNL:
- Renal stones >2 cm
- Staghorn calculi
- Lower pole renal stones with anatomy unfavourable for SWL
- Failed SWL or RIRS
- ESWL-refractory stones <2 cm
Contraindications to PCNL:
- Pregnancy
- Untreated UTI
- Bleeding diathesis
- Current anticoagulation
Complications:
- Bleeding (may require selective angioembolisation for pseudoaneurysm/AVF)
- Infection/urosepsis
- Pleural violation (supracostal puncture → pneumothorax/hydrothorax)
- Injury to adjacent organs (colon, spleen, liver)
- Residual stones
Mini-PCNL (miniaturised PCNL): Uses smaller instruments (mini-perc); equivalent stone-free rates with less bleeding; useful for smaller complex stones
Steinstrasse (post-ESWL complication)
8. Choice of Procedure - Decision Matrix
| Stone Size & Location | Preferred Procedure |
|---|---|
| ≤5 mm, asymptomatic | Watchful waiting + MET |
| 5-10 mm, distal ureter | MET (tamsulosin), then URS if fails |
| ≤10 mm, proximal ureter | SWL first; URS if fails |
| >10 mm, proximal ureter | URS (higher success than SWL) |
| <2 cm, non-lower-pole renal | SWL or RIRS |
| <2 cm, lower pole renal | RIRS or PCNL (SWL has poor clearance due to gravity) |
| >2 cm, renal | PCNL |
| Staghorn calculi | PCNL |
| Cystine stones | PCNL or URS (resistant to SWL) |
9. Indications for Urgent/Emergency Surgical Intervention
- Failure of medical management
- Sepsis with obstruction (emergency decompression - JJ stent or PCN)
- Impaired renal function (obstructive uropathy)
- Chronic infection - staghorn calculi, matrix calculi
- Solitary kidney with obstruction
- High-risk occupation (pilots, locomotive drivers, sailors)
- Patient's preference
10. Prevention of Recurrence
| Stone Type | Prevention |
|---|---|
| All types | High fluid intake (2-2.5 L/day), reduce animal protein, reduce salt intake |
| Calcium oxalate | Reduce oxalate-rich foods, potassium citrate, thiazide diuretics (↓ urinary Ca²⁺) |
| Uric acid | Allopurinol, alkalinise urine (potassium citrate) |
| Struvite/infection | Complete stone removal + long-term antibiotics (mandatory) |
| Cystine | Alkalinise urine, D-penicillamine, tiopronin |
11. Summary Box (High-Yield MBBS Points)
- Most common stone: Calcium oxalate (60-85%)
- Most common metabolic abnormality: Hypercalciuria
- Investigation of choice: NCCT abdomen
- Most common acute presentation: Ureteric colic
- SWL introduced by: Christian Chaussy, 1980
- Steinstrasse: Complication of SWL; stone fragments lining distal ureter
- PCNL for: Stones >2 cm, staghorn calculi, failed SWL
- URS for: Mid/distal ureteral stones (procedure of choice)
- Staghorn calculi: Infection stones; must be completely cleared; long-term antibiotics after removal
- Cystine stones: SWL-resistant (very hard due to disulfide bonds)
- Open surgery: <1% of cases in modern era
- Emergency decompression: JJ stent or PCN for sepsis with obstruction
Bailey and Love's Short Practice of Surgery, 28th Ed., pp. 1495-1499 | Schwartz's Principles of Surgery, 11th Ed., pp. 1789-1791 | Campbell-Walsh-Wein Urology
This is a shared conversation. Sign in to Orris to start your own chat.