Teach ECG
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have enough rich content from authoritative sources to deliver a comprehensive ECG teaching session. Let me compile everything.
ECG (Electrocardiogram) - Complete Guide
1. What is an ECG?
The ECG (electrocardiogram, also written EKG) records tiny electrical potential differences on the body surface that reflect the heart's electrical activity. These potentials arise because the myocardium does not depolarize all at once - atria before ventricles, with specific sequences in each - creating measurable voltage differences detectable by skin electrodes.
First introduced by Einthoven in the early 1900s, the standard ECG records 10 seconds of cardiac activity from 12 vantage points (leads) derived from 10 electrodes.
- Goldman-Cecil Medicine, p. 421
- Costanzo Physiology 7th Edition, p. 148
2. The Cardiac Conduction System (Foundation)
Before reading an ECG, you must understand what generates each waveform:
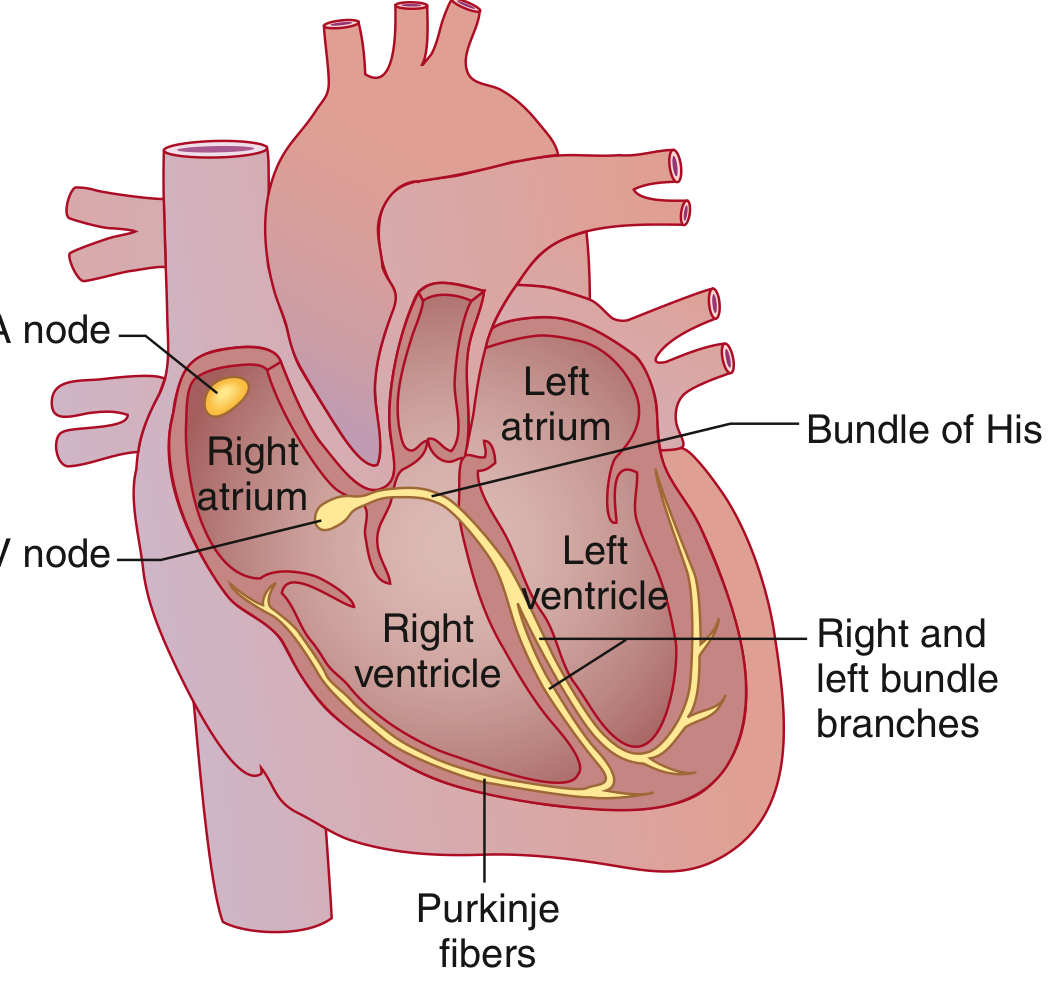
The conduction system has four components:
| Structure | Location | Function |
|---|---|---|
| SA node | High right atrium near SVC junction | Primary pacemaker - fires spontaneously at highest rate |
| AV node | Near coronary sinus opening, AV septum | Physiologic conduction delay (protects ventricles from rapid atrial rates) |
| Bundle of His + Bundle Branches | Interventricular septum | Rapid conduction to both ventricles |
| Purkinje fibers | Subendocardial network | Final delivery of impulse to ventricular myocardium |
The AV node is an area of relatively slow conduction - this delay between atrial and ventricular contraction is normal and reflected in the PR interval. Conduction velocity in the His-Purkinje system is much faster than in atrial tissue, which is why the QRS duration is similar to P wave duration despite the far larger ventricular mass.
- Gray's Anatomy for Students, p. 247
- Goldman-Cecil Medicine, p. 421
3. ECG Paper and Calibration
Standard ECG paper has two grid sizes:
| Small box (1 mm) | Big box (5 mm) | |
|---|---|---|
| Time (X-axis) | 0.04 sec (40 ms) | 0.2 sec (200 ms) |
| Voltage (Y-axis) | 0.1 mV | 0.5 mV |
Standard recording speed: 25 mm/sec
Standard calibration: 10 mm = 1 mV
A standard ECG = 10 seconds total, with leads grouped: I/II/III → aVR/aVL/aVF → V1/V2/V3 → V4/V5/V6 (each group 2.5 seconds), plus a full 10-second rhythm strip.
- Goldman-Cecil Medicine, p. 422
4. The ECG Waveforms

P Wave
- Represents atrial depolarization
- Duration reflects conduction time through the atria
- Atrial repolarization is not visible (buried within the QRS complex)
- Normal duration: < 120 ms (3 small boxes)
PR Interval
- From onset of P wave to onset of QRS complex
- Represents total conduction time: atria + AV node + His-Purkinje
- The PR segment (flat portion) = AV node conduction delay
- Normal: 120-200 ms (3-5 small boxes)
- Prolonged PR (>200 ms) = 1st-degree AV block (more accurately: delayed AV conduction)
- Short PR = preexcitation (WPW), junctional rhythm, or enhanced AV conduction
QRS Complex
- Represents ventricular depolarization
- Q = initial negative deflection
- R = positive deflection
- S = negative deflection following a positive deflection
- Capital letters (Q, R, S) = amplitude ≥5 mm; lowercase (q, r, s) = <5 mm
- Normal duration: 75-110 ms (just under 3 small boxes)
- Prolonged QRS (>120 ms) = bundle branch block or intraventricular conduction delay
ST Segment
- From end of QRS to beginning of T wave (at the J point)
- Represents the plateau phase of ventricular action potential
- Normally isoelectric (flat)
- Elevation or depression = ischemia, infarction, pericarditis, other
T Wave
- Represents ventricular repolarization
- Normally same direction as QRS in most leads
- Normally upright in I, II, V3-V6; inverted in aVR
QT Interval
- From onset of QRS to end of T wave
- Represents total ventricular electrical activity (depolarization + repolarization)
- Must be rate-corrected (QTc) using Bazett's formula:
QTc = QT / √RR (both in seconds)
- Normal QTc: men ≤450 ms; women ≤460 ms
- Prolonged QTc → risk of torsades de pointes
U Wave
-
Small deflection after T wave, same polarity
-
Not always visible; prominent U waves suggest hypokalemia
-
Costanzo Physiology 7th Edition, p. 149
-
Medical Physiology (Boron & Boulpaep), p. 733
-
Goldman-Cecil Medicine, p. 422-423
5. Normal Intervals - Quick Reference
| Parameter | Normal Range |
|---|---|
| Heart rate | 50-100 bpm |
| P wave duration | < 120 ms |
| PR interval | 120-200 ms |
| QRS duration | 75-110 ms |
| QTc (males) | 390-450 ms |
| QTc (females) | 390-460 ms |
| QRS axis | -30° to +90° |
- Goldman-Cecil Medicine (Table 42-1)
6. The 12 Leads - Where They Look
The 12 leads provide 12 different "camera angles" on the heart's electrical activity.
Limb Leads (Frontal Plane)
Bipolar leads measure voltage difference between two limb electrodes:
- Lead I: Right arm (-) vs. Left arm (+) → looks left
- Lead II: Right arm (-) vs. Left leg (+) → looks down-left
- Lead III: Left arm (-) vs. Left leg (+) → looks down-right
Augmented unipolar leads compare one limb to a combined reference:
- aVR: Right arm → looks toward right shoulder (normally negative P and QRS)
- aVL: Left arm → looks toward left shoulder
- aVF: Left foot → looks inferiorly (normally positive P and QRS)
Precordial Leads (Horizontal Plane)
Placed on specific chest wall positions:
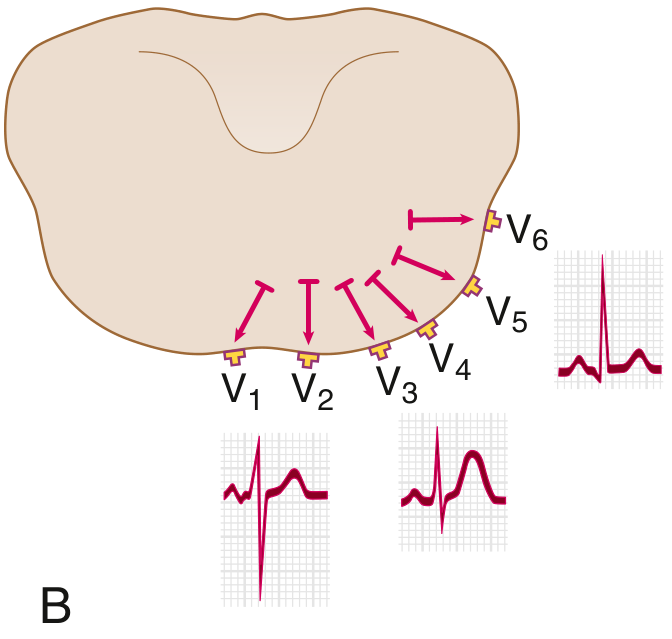
| Lead | Position | Looks at |
|---|---|---|
| V1 | 4th intercostal space, right sternal border | Right ventricle / septum |
| V2 | 4th intercostal space, left sternal border | Right ventricle / septum |
| V3 | Between V2 and V4 | Anterior wall |
| V4 | 5th intercostal space, midclavicular line | Anterior wall |
| V5 | Anterior axillary line, same level as V4 | Lateral wall |
| V6 | Midaxillary line, same level as V4 | Lateral wall |
Regional groupings for pathology:
- Inferior: II, III, aVF (RCA territory)
- Anterior: V1-V4 (LAD territory)
- Lateral: I, aVL, V5-V6 (LCx territory)
- Septal: V1-V2
Normal Precordial R-Wave Progression
-
V1: small r, deep S
-
Transition (R = S) at V3 or V4
-
V5-V6: large R, small s (septal q waves are normal here)
-
Goldman-Cecil Medicine, p. 423-424
7. Calculating Heart Rate
Regular rhythm: Count the number of big boxes between two consecutive R waves, then use:
| RR interval (big boxes) | Heart rate |
|---|---|
| 1 big box | 300 bpm |
| 2 big boxes | 150 bpm |
| 3 big boxes | 100 bpm |
| 4 big boxes | 75 bpm |
| 5 big boxes | 60 bpm |
| 6 big boxes | 50 bpm |
Irregular rhythm (e.g., AF): Count beats in 10-second strip × 6 = bpm
Formula: HR (bpm) = 60,000 / RR interval (ms)
8. QRS Axis
The QRS axis describes the mean direction of ventricular depolarization in the frontal plane.
| Axis | Range | Interpretation |
|---|---|---|
| Normal | -30° to +90° | Normal |
| Left axis deviation (LAD) | -30° to -90° | Left anterior fascicular block, inferior MI, etc. |
| Right axis deviation (RAD) | +90° to +180° | Right ventricular hypertrophy, left posterior fascicular block, etc. |
| Extreme RAD | -90° to ±180° | Severe pathology |
Quick estimation method:
- Find the lead where QRS is most isoelectric (equal positive and negative) - the axis is perpendicular to this lead
- Confirm direction using the adjacent leads
Shortcut:
-
If QRS is positive in both Lead I and aVF → normal axis
-
Positive I, negative aVF → possible LAD
-
Negative I, positive aVF → RAD
-
Goldman-Cecil Medicine, p. 424-425
9. A Systematic Approach to ECG Interpretation
Harrison's Principles of Internal Medicine lists 14 parameters to assess in every ECG:
- Standardization & technical quality - correct calibration (1 mV = 10 mm), lead placement, artifacts
- Rhythm - regular vs. irregular; sinus vs. non-sinus
- Heart rate - use RR interval method above
- PR interval / AV conduction - normal 120-200 ms
- QRS duration - normal 75-110 ms
- QT / QTc interval - calculate and correct for rate
- QRS axis - normal, LAD, or RAD
- P waves - morphology, duration, axis
- QRS voltages - high (hypertrophy) or low
- Precordial R-wave progression - normal transition V3-V4
- Abnormal Q waves - pathological Q = width >40 ms or depth >25% R wave
- ST segments - elevation or depression
- T waves - direction, morphology, inversions
- U waves - presence, size, polarity
Comparison with previous ECGs is invaluable.
- Harrison's Principles of Internal Medicine 22E, p. 1592
10. A Normal 12-Lead ECG - What to Expect
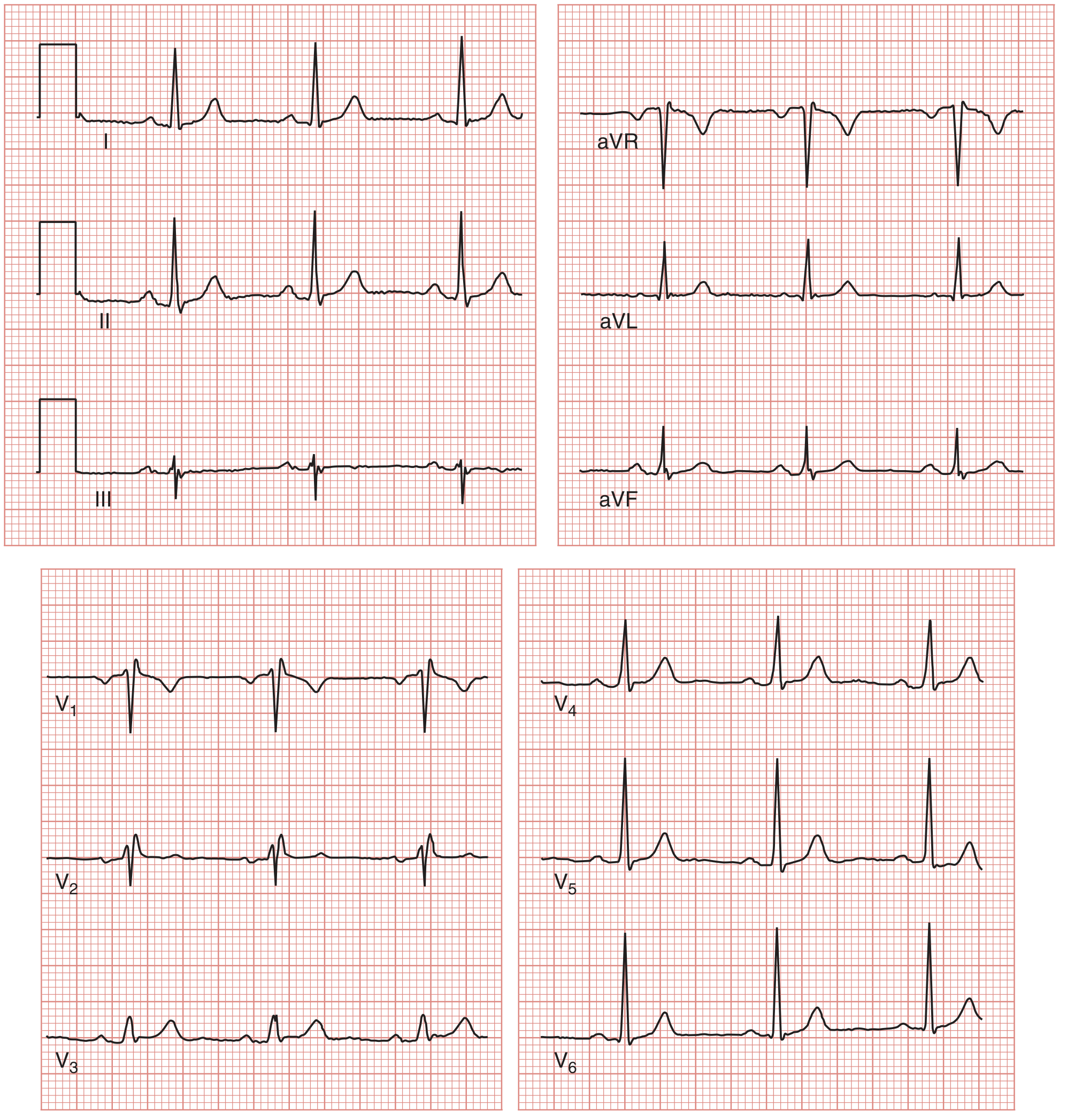
In a normal ECG:
- Sinus rhythm (P before every QRS, consistent PR interval)
- P waves upright in I, II, aVF; negative in aVR
- PR interval 120-200 ms
- QRS < 110 ms
- Axis between -30° and +90°
- R-wave transition at V3-V4
- Septal q waves in V5-V6 (normal - from early septal depolarization)
- T waves upright in I, II, V3-V6
11. Key Abnormal Patterns (Overview)
| Finding | Significance |
|---|---|
| PR > 200 ms | 1st-degree AV block |
| Progressively lengthening PR → dropped QRS | 2nd-degree AV block (Mobitz I / Wenckebach) |
| Fixed PR + dropped QRS | 2nd-degree AV block (Mobitz II) |
| No relationship between P and QRS | 3rd-degree (complete) AV block |
| Wide QRS (≥120 ms) with RBBB pattern | Right bundle branch block |
| Wide QRS with LBBB pattern | Left bundle branch block |
| Short PR + delta wave | WPW syndrome (preexcitation) |
| ST elevation (regional) | STEMI (until proven otherwise) |
| ST depression | Ischemia, NSTEMI, digoxin effect |
| Pathological Q waves | Prior myocardial infarction |
| Peaked T waves | Hyperkalemia |
| Prolonged QTc | Drug effects, hypokalemia, hypomagnesemia, congenital LQTS |
| J wave (Osborn wave) | Hypothermia |
Summary Flow for Reading Any ECG
Rate → Rhythm → Axis → Intervals (PR, QRS, QTc)
→ P waves → QRS morphology → ST segments → T waves → U waves
→ Compare with previous → Clinical correlation
The ECG is a powerful tool, but errors are common when interpretation is rushed or unsystematic. As Harrison's notes: "Many mistakes in ECG interpretation are errors of omission."
Sources: Goldman-Cecil Medicine 2-Volume Set (Ganz & Link); Harrison's Principles of Internal Medicine 22E; Costanzo Physiology 7th Ed; Medical Physiology (Boron & Boulpaep); Gray's Anatomy for Students; Miller's Anesthesia 10th Ed
This is a shared conversation. Sign in to Orris to start your own chat.