Pulmonary mechanics full details for md exam answer 10 marks give point to fetch more marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a complete, mark-scoring 10-mark answer. Here is the full structured answer:
PULMONARY MECHANICS - Complete 10-Mark Answer
DEFINITION
Pulmonary mechanics refers to the physical forces that govern the movement of air into and out of the lungs, including the pressures generated, the elastic properties of lung tissue, airway resistance, and the work performed by respiratory muscles.
1. MUSCLES OF VENTILATION
(Source: Guyton and Hall Textbook of Medical Physiology)
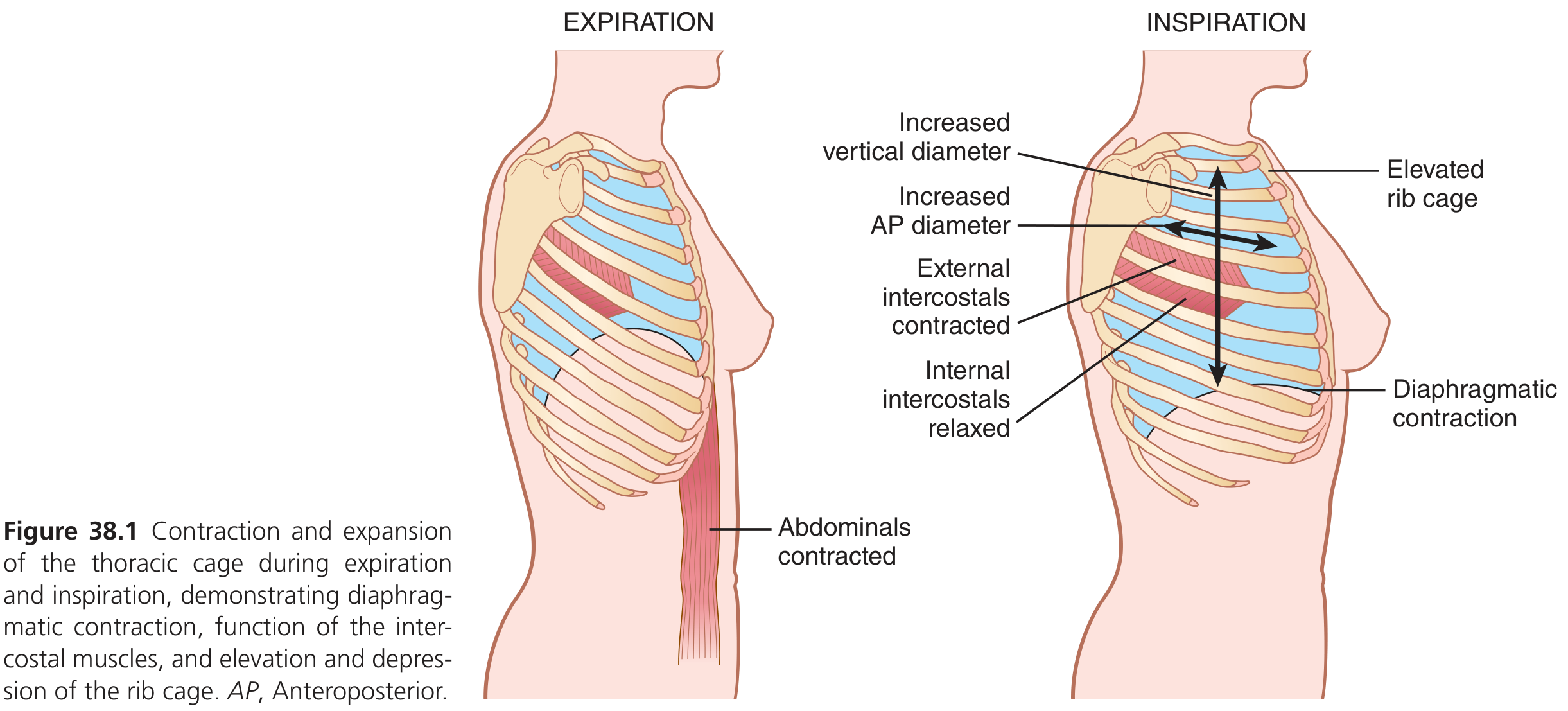
Inspiration muscles (active):
- Diaphragm - principal muscle; contracts and moves downward, increasing vertical chest diameter (accounts for ~75% of quiet breathing)
- External intercostals - elevate the ribs, increasing anteroposterior (AP) diameter by ~20%
- Accessory muscles (recruited during heavy breathing): sternocleidomastoids (lift sternum), anterior serrati (lift ribs), scaleni (lift first two ribs)
Expiration muscles:
- Quiet expiration is passive - driven by elastic recoil of lungs and chest wall
- Forced expiration: internal intercostals + abdominal recti (compress abdominal contents upward, push diaphragm up)
Exam tip: "Inspiration is always active; quiet expiration is passive; forced expiration is active."
2. PRESSURES GOVERNING AIR FLOW
(Source: Guyton and Hall Textbook of Medical Physiology)
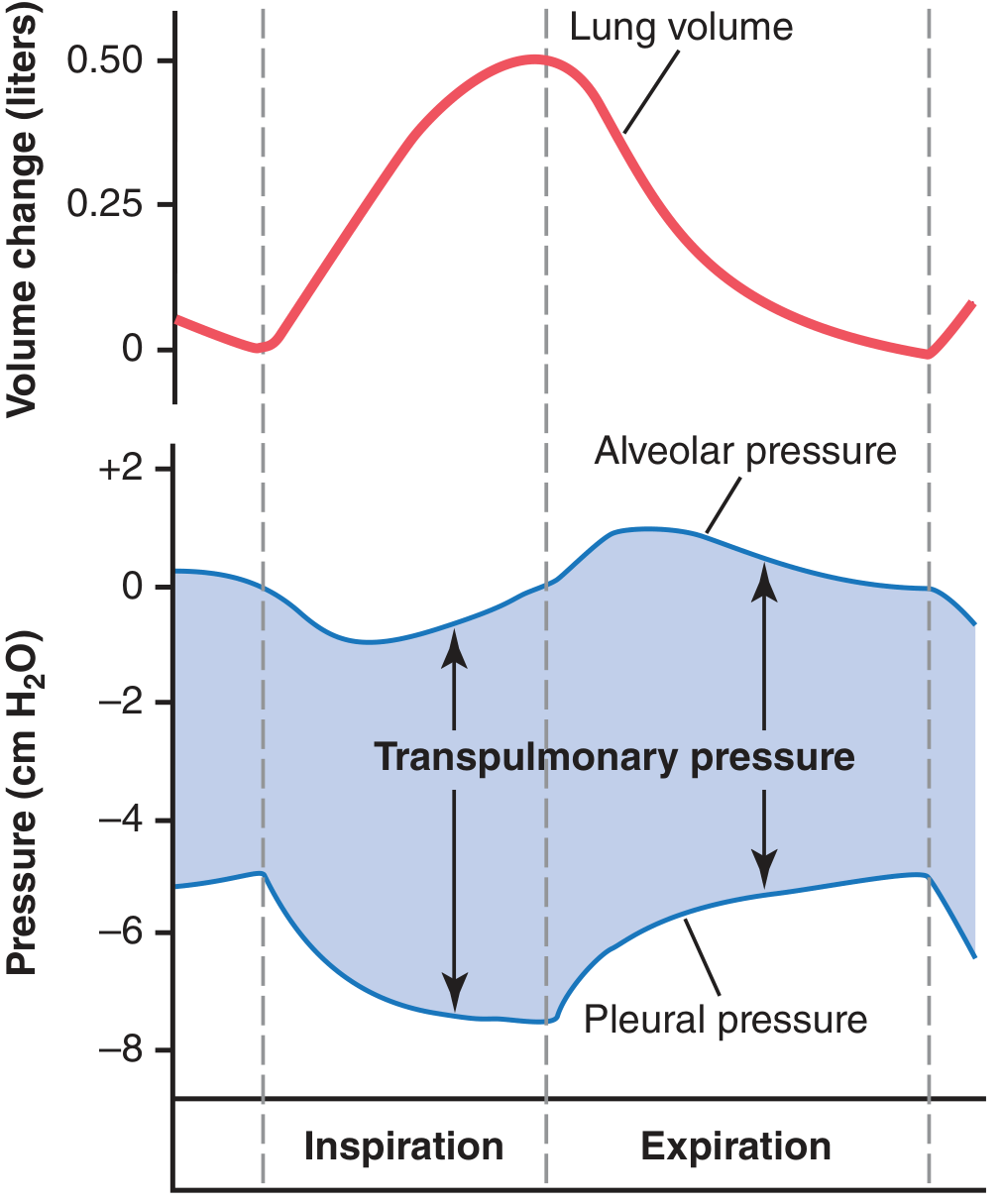
A. Pleural (Intrapleural) Pressure
- Normally slightly negative (-5 cm H₂O at rest) - acts as suction holding lungs against the chest wall
- During inspiration: becomes more negative, reaching -7.5 cm H₂O
- During expiration: returns toward -5 cm H₂O
- The negativity is maintained by continuous lymphatic drainage of pleural fluid
B. Alveolar Pressure
- At rest (no airflow): equals atmospheric = 0 cm H₂O
- During inspiration: drops to -1 cm H₂O (below atmospheric) → drives air in
- During expiration: rises to +1 cm H₂O → drives air out
- Governed by Boyle's Law: as lung volume increases, alveolar pressure falls
C. Transpulmonary Pressure
- = Alveolar pressure - Pleural pressure
- Represents the elastic recoil force (recoil pressure) tending to collapse the lung
- Normal at FRC: approximately +5 cm H₂O
- Greater transpulmonary pressure = larger lung volume
3. LUNG COMPLIANCE
(Source: Ganong's Review of Medical Physiology; Guyton and Hall)
Definition: Compliance = Change in lung volume per unit change in transpulmonary pressure.
$$C = \frac{\Delta V}{\Delta P}$$
Normal values:
| Parameter | Value |
|---|---|
| Lung compliance alone | 200 mL/cm H₂O |
| Chest wall compliance | ~200 mL/cm H₂O |
| Combined (lung + thorax) | ~110 mL/cm H₂O |
The combined compliance is half that of the lungs alone because the chest wall opposes expansion.
Pressure-Volume (P-V) Loop / Hysteresis:
- The inflation and deflation curves do not coincide - this is called hysteresis
- During deflation the lung recoils at a higher pressure for a given volume
- Hysteresis is partly due to surfactant behavior
- When lungs are inflated with saline (eliminating surface tension), hysteresis disappears - confirming that surface tension contributes significantly
Factors decreasing compliance (stiffer lungs):
- Pulmonary fibrosis, pulmonary edema, atelectasis, ARDS
- Higher lung volumes (reduced compliance at extremes)
Factors increasing compliance (more floppy):
- Emphysema (destruction of elastic tissue)
- Normal aging
4. SURFACE TENSION AND SURFACTANT
(Source: Guyton and Hall; Ganong's Review; Murray & Nadel's)
Law of Laplace
For a spherical alveolus:
$$P = \frac{2T}{r}$$
Where P = collapsing pressure, T = surface tension, r = radius.
Key implication: Smaller alveoli develop higher collapsing pressure → tendency to collapse (atelectasis).
Role of Surfactant
- Secreted by Type II pneumocytes (alveolar epithelial cells)
- Composition: primarily dipalmitoylphosphatidylcholine (DPPC) + other lipids + proteins (SP-A, SP-B, SP-C, SP-D)
- Reduces alveolar surface tension from 50 dynes/cm (no surfactant) to 5-30 dynes/cm
- Prevents alveolar collapse on expiration (when radius is small, surfactant concentrates and lowers T further)
- Prevents pulmonary edema (without surfactant, ~20 mmHg unopposed surface tension would pull fluid into alveoli)
- SP-A and SP-D are collectins involved in innate immunity
Clinical significance - Respiratory Distress Syndrome (RDS)
- Surfactant production begins at 26-28 weeks gestation; adequate amounts by 34-36 weeks
- Premature infants lack surfactant → Infant Respiratory Distress Syndrome (IRDS) / Hyaline Membrane Disease
- Alveolar surface tension can be 6-8× normal
- Treatment: exogenous surfactant replacement + CPAP
5. ELASTIC RECOIL
- Lungs have a natural tendency to collapse (recoil inward) and chest wall tends to spring outward
- At FRC (Functional Residual Capacity), inward recoil of lungs = outward recoil of chest wall → equilibrium
- Elastic recoil has two components:
- Tissue elasticity (~33%): from elastic and collagen fibers in lung parenchyma
- Surface tension forces (~67%): from alveolar fluid interface
6. AIRWAY RESISTANCE
(Source: Costanzo Physiology; Guyton and Hall)
Poiseuille's Law for Airway Resistance
$$R = \frac{8\eta l}{\pi r^4}$$
Where: R = resistance, η = viscosity of gas, l = airway length, r = airway radius
Critical relationship: Resistance is inversely proportional to the 4th power of radius
- If radius halves → resistance increases 16-fold (2⁴)
- If radius doubles → resistance decreases 16-fold
Site of Greatest Resistance
- Medium-sized bronchi have the highest individual airway resistance
- Although terminal bronchioles are narrow, they are in parallel → total peripheral resistance is low
- Applying the parallel resistance rule: adding airways in parallel reduces total resistance
Laminar vs. Turbulent Flow
- Laminar flow (low velocity, smooth): obeys Poiseuille's law; R depends on viscosity
- Turbulent flow (high velocity, branching points): R depends on gas density (not viscosity)
- Relevant in: upper airway obstruction, exercise, helium use (low density → reduces turbulent resistance)
- Reynolds number (Re): turbulence when Re >2000
- Re = (velocity × diameter × density) / viscosity
Factors Altering Airway Resistance
| Factor | Effect on Resistance |
|---|---|
| Parasympathetic (ACh → M3 receptors) | Bronchoconstriction → ↑ R |
| Sympathetic (β₂ agonists) | Bronchodilation → ↓ R |
| Histamine, leukotrienes | Bronchoconstriction → ↑ R |
| ↑ Lung volume | Radial traction → ↓ R |
| ↓ Lung volume | Airway collapse → ↑ R |
| Breathing helium | ↓ Gas density → ↓ turbulent R |
| Emphysema | Loss of tethering → dynamic collapse → ↑ R |
7. WORK OF BREATHING
(Source: Ganong's Review of Medical Physiology)
Work of breathing = Pressure × Volume
Components during quiet breathing:
| Component | % of Total Work |
|---|---|
| Elastic work (stretching lungs + chest wall) | ~65% |
| Viscous/tissue resistance | ~7% |
| Airway resistance (moving air) | ~28% |
Normal value: 0.3-0.8 kg·m/min at rest; <3% of total body energy expenditure during exercise
Clinical significance:
- In emphysema: compliance is high but airway resistance increases (dynamic collapse) → increased airway resistance work
- In fibrosis/ARDS: compliance is low → increased elastic work
- In asthma: bronchoconstriction → increased airway resistance work; patients breathe at higher lung volumes to exploit radial traction
Oxygen cost of breathing:
- Normal: <5% of total VO₂
- Severe lung disease: up to 30-40% → respiratory muscle fatigue → ventilatory failure (pump failure)
8. DYNAMIC AIRWAY COMPRESSION (Equal Pressure Point)
- During forced expiration, as pleural pressure becomes highly positive, it can compress intrathoracic airways
- At the Equal Pressure Point (EPP), airway pressure = pleural pressure → dynamic compression begins
- Downstream from EPP, airways are compressed → flow-limited ("effort-independent" zone of MEFV curve)
- In emphysema: loss of elastic recoil moves EPP proximally → earlier collapse → air trapping
9. COMPLIANCE OF THORAX AND LUNGS TOGETHER
- Combined lung-thorax compliance = 110 mL/cm H₂O (approximately half of lung alone)
- At extremes of lung volume, combined compliance can fall to <20% of lungs alone
- In a paralyzed patient, the effort to inflate the combined system requires almost twice the pressure compared to excised lungs alone
10. CLINICAL APPLICATIONS (High-Yield Exam Points)
| Disease | Compliance | Airway Resistance | Mechanics Defect |
|---|---|---|---|
| Emphysema | ↑ (destroyed elastin) | ↑ (dynamic collapse) | Obstructive; air trapping |
| Pulmonary Fibrosis | ↓ (stiff lungs) | Normal/↑ | Restrictive; small tidal volumes |
| Asthma | Normal/↑ | ↑↑ (bronchoconstriction) | Obstructive; reversible |
| IRDS (Neonatal) | ↓ (no surfactant) | ↑ | Atelectasis; ↑ surface tension |
| Pulmonary Edema | ↓ | ↑ | Restrictive + obstructive |
| Pneumothorax | Loss of pleural suction | - | Lung collapse |
SUMMARY TABLE FOR QUICK REVISION
| Parameter | Normal Value | Clinical Relevance |
|---|---|---|
| Pleural pressure (rest) | -5 cm H₂O | More negative in inspiration (-7.5) |
| Alveolar pressure (inspiration) | -1 cm H₂O | Drives air inward |
| Alveolar pressure (expiration) | +1 cm H₂O | Drives air outward |
| Transpulmonary pressure | +5 cm H₂O at FRC | Keeps lungs open |
| Lung compliance | 200 mL/cm H₂O | ↓ in fibrosis; ↑ in emphysema |
| Combined compliance | 110 mL/cm H₂O | Half of lung alone |
| Surfactant surface tension | 5-30 dynes/cm | vs. 50 without surfactant |
| Airway resistance (medium bronchi) | Highest site | 4th power of radius |
EXAM STRATEGY - HOW TO SCORE FULL MARKS
- Start with a definition and classification (static vs. dynamic mechanics)
- Muscles section - name specific muscles with their actions
- Pressures section - give exact values with directions of change; draw the pressure diagram
- Compliance - define with formula, give numbers, explain hysteresis, clinical conditions
- Surface tension/surfactant - Law of Laplace formula, DPPC composition, IRDS
- Airway resistance - Poiseuille's law formula, 4th-power relationship, sites, laminar/turbulent
- Work of breathing - three components with percentages
- Clinical correlations - table format maximizes marks per line
- Draw diagrams - P-V loop (compliance), P-time/Volume-time curves for pressures
Sources: Guyton and Hall Textbook of Medical Physiology | Ganong's Review of Medical Physiology | Costanzo Physiology 7th Ed. | Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.