What are the factors affecting the cardiac output? And the cardiac- ... the heart rate and the heart rate output of a person in rest, in exercise, and their graphs. Explain them in detail.
Reading File
Finding Sources
Finding Sources
Searching the Web
cardiac output factors affecting heart rate rest exercise graphs physiology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
I now have comprehensive information and graphs from authoritative textbooks. Let me compile a detailed, well-structured answer.
Cardiac Output: Factors, Heart Rate, and Exercise Physiology
1. What is Cardiac Output?
Cardiac output (CO) is the total volume of blood ejected by one ventricle per minute. It is calculated as:
CO = Stroke Volume (SV) × Heart Rate (HR)
Normal resting values (70-kg man):
- Stroke Volume: ~70 mL/beat
- Heart Rate: ~72 beats/min
- Cardiac Output: ~5,000 mL/min (5 L/min)
(Costanzo Physiology 7th Edition, p. 155)
2. Factors Affecting Cardiac Output
Since CO = SV × HR, anything that affects either stroke volume or heart rate will affect cardiac output.
A. Factors Affecting STROKE VOLUME
Stroke volume is controlled by three key determinants:
1. Preload (End-Diastolic Volume)
Preload is the volume of blood filling the ventricle at the end of diastole (EDV). It is governed by the Frank-Starling Law of the Heart:
"The volume of blood ejected by the ventricle depends on the volume present in the ventricle at the end of diastole."
The more blood that returns to the heart (venous return), the more the myocardial fibers are stretched before contraction. Greater stretch = greater force of contraction = greater stroke volume. This is the length-tension relationship applied to cardiac muscle.
Frank-Starling Relationship Graph:
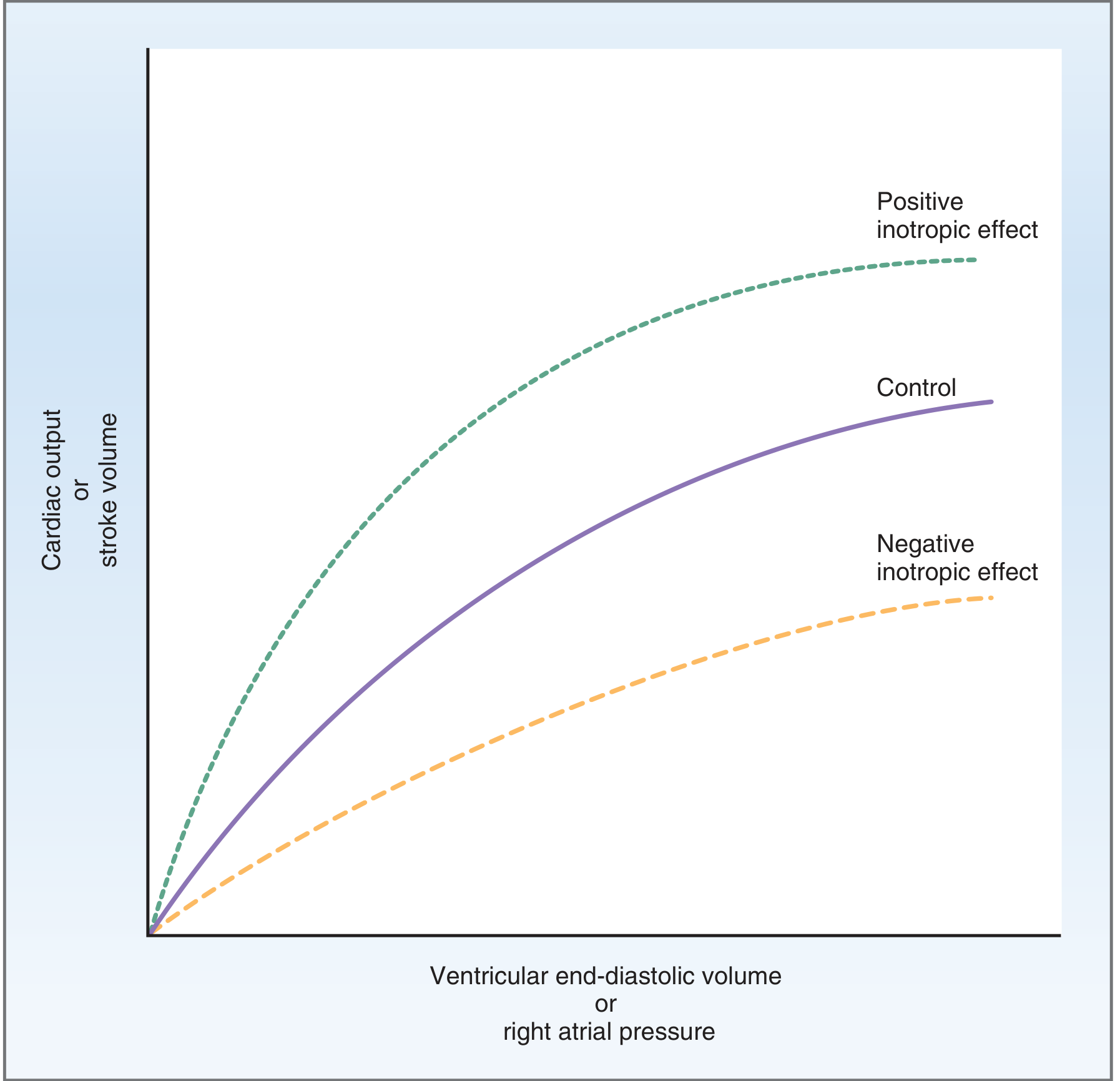
The three curves show: Control (normal), Positive inotropic effect (curve shifts upward - more stroke volume for same EDV), Negative inotropic effect (curve shifts downward). - Costanzo Physiology 7th Edition, Fig. 4.22
Factors that INCREASE preload (increase CO):
- Increased venous return (e.g., exercise, increased blood volume)
- Bradycardia (longer diastolic filling time)
- Lying down (increased venous return from legs)
Factors that DECREASE preload (decrease CO):
- Hemorrhage / dehydration
- Venodilators (e.g., nitroglycerin)
- Standing up suddenly (blood pools in lower extremities)
2. Afterload
Afterload is the resistance the ventricle must overcome to eject blood - primarily determined by aortic pressure (systemic vascular resistance). It is the "load" the heart must pump against.
- Increased afterload (e.g., hypertension, aortic stenosis): the ventricle cannot eject as much blood, so end-systolic volume increases and stroke volume falls.
- Decreased afterload (e.g., vasodilators like ACE inhibitors): the ventricle ejects more easily, stroke volume increases.
3. Myocardial Contractility (Inotropy)
Contractility is the intrinsic ability of the heart muscle to generate force at a given fiber length, independent of preload or afterload. It reflects how much Ca²+ is available to the contractile proteins (actin-myosin).
Positive inotropic factors (increase contractility):
- Sympathetic stimulation / catecholamines (norepinephrine, epinephrine) - act via β1 receptors → increased cAMP → increased intracellular Ca²+
- Digoxin (inhibits Na⁺/K⁺-ATPase → increases intracellular Ca²+)
- Increased heart rate (Bowditch/Treppe effect - more Ca²+ accumulates)
- Exercise
Negative inotropic factors (decrease contractility):
- Parasympathetic stimulation
- Acidosis
- Hypoxia
- Beta-blockers
- Calcium channel blockers
- Heart failure
As shown in the Frank-Starling graph above, positive inotropes shift the curve upward (more CO per given EDV), and negative inotropes shift it downward.
B. Factors Affecting HEART RATE
Heart rate is primarily controlled by the autonomic nervous system acting on the SA node:
| Factor | Effect on HR | Mechanism |
|---|---|---|
| Sympathetic stimulation | Increases HR (positive chronotropy) | Norepinephrine/Epinephrine → β1 receptors → increases slope of pacemaker potential |
| Parasympathetic stimulation (vagus) | Decreases HR (negative chronotropy) | Acetylcholine → M2 receptors → increases K+ conductance → hyperpolarizes SA node |
| Epinephrine (circulating) | Increases HR | β1 adrenergic |
| Fever/increased body temperature | Increases HR (~10 bpm per 1°C rise) | Direct effect on SA node spontaneous depolarization rate |
| Thyroid hormone | Increases HR | Increased sensitivity to catecholamines, direct effect |
| Hypoxia | Increases HR | Chemoreceptor-mediated sympathetic activation |
| Baroreceptor reflex | Modulates HR | Fall in BP → HR increases; rise in BP → HR decreases |
| Age | Decreases maximal HR | Max HR ≈ 220 - age |
| Athletic training | Decreases resting HR | Increased vagal tone (athlete's bradycardia) |
| Hypovolemia | Increases HR | Compensatory sympathetic activation |
3. Cardiac Output at Rest vs. Exercise
At Rest
- Heart rate: 60-80 beats/min (typically ~72 bpm)
- Stroke volume: ~70 mL
- Cardiac output: ~5 L/min
The resting heart is under predominant parasympathetic (vagal) tone which keeps HR relatively low. Trained athletes may have resting HR as low as 40-50 bpm due to enhanced vagal tone, but their stroke volumes are larger (larger chamber size due to cardiac hypertrophy), so CO is maintained normally at ~5 L/min.
During Exercise
Exercise dramatically increases metabolic demand for oxygen, and the cardiovascular system responds with large increases in CO.
Typical cardiac outputs at different exercise levels (Guyton & Hall):
| State | Cardiac Output |
|---|---|
| Young man at rest | 5.5 L/min |
| Maximal exercise - untrained young man | ~23 L/min |
| Maximal exercise - average male marathoner | ~30 L/min |
| Elite marathoners | 35-40 L/min |
The increase in CO during exercise results from both increased HR and increased SV, but not equally at all intensities.
The Two Phases of CO Increase During Exercise
Phase 1 - Up to 50-60% of maximal HR:
- Both HR and SV increase
- SV increases due to: (a) increased venous return via the muscle pump (Frank-Starling mechanism), (b) increased sympathetic contractility, (c) reduced peripheral resistance (vasodilation in active muscles)
Phase 2 - Above 60% of maximal HR:
- SV plateaus and no longer rises
- Further increases in CO are achieved solely by continued increases in HR
- The heart beats so fast at high intensities that diastolic filling time becomes too short to allow further increases in SV
(PT Direct / Medical Physiology - Boron & Boulpaep)
Graph: Cardiac Output vs. Work Output During Exercise
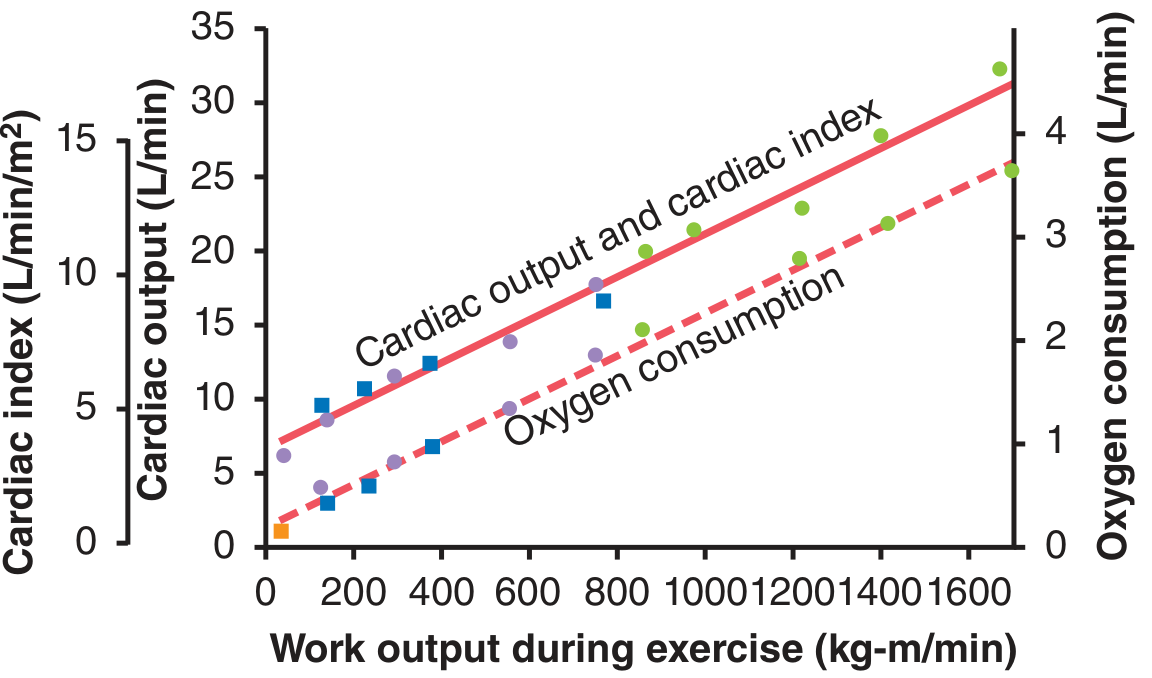
Guyton & Hall, Fig. 85.10 - Both cardiac output (solid red line) and oxygen consumption (dashed red line) increase in a linear fashion with increasing work output during exercise. CO starts at ~5.5 L/min at rest and can reach 23-30+ L/min at maximal exercise.
Graph: Venous Return and Cardiac Output Curves in Exercise
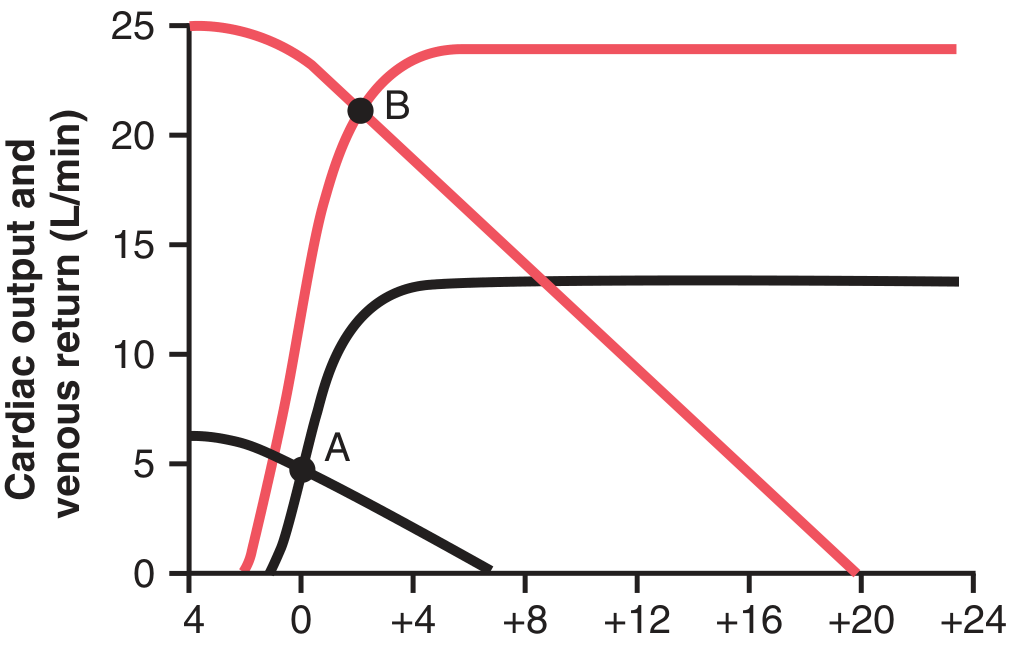
Guyton & Hall, Fig. 21.2 - Black curves = normal circulation (equilibrium at Point A, ~5 L/min). Red curves = heavy exercise (equilibrium at Point B, ~21 L/min). Both the cardiac output curve (upward shift from sympathetic stimulation) and the venous return curve (upward rotation from increased mean systemic filling pressure + decreased venous resistance) shift to achieve the new high-output equilibrium.
4. Mechanisms Driving CO Increase in Exercise
Three main pathways act simultaneously:
1. Central Command (Early/Anticipatory)
Higher brain centers (motor cortex) send signals to the cardiovascular control centers even before exercise starts, causing an immediate increase in sympathetic outflow and withdrawal of parasympathetic tone. This is why HR rises within the first breath of exercise - it is not driven by muscle chemicals, but by anticipation.
2. Mechanical Response from Muscle Pump (Delayed)
Contracting skeletal muscles compress veins, squeezing blood back to the heart. This increases venous return → raises EDV → Frank-Starling mechanism increases SV → CO rises. (Boron & Boulpaep, Medical Physiology)
3. Chemical/Metabolic Response (Delayed)
Active muscles release CO₂, lactic acid, K⁺, adenosine, and lower local O₂ and pH. These metabolites cause local arteriolar vasodilation in active muscle, reducing total peripheral resistance and allowing more blood flow. The fall in BP triggers baroreceptors → reflex sympathetic activation → HR and contractility increase.
Sympathetic changes at maximal exercise (Guyton & Hall):
- HR increases to 170-190 beats/min
- Contractility increases to ~2x normal
- Mean systemic filling pressure rises from 7 mmHg → up to 30 mmHg (sympathetic venoconstriction + muscle compression)
- Peripheral vascular resistance falls in active muscles (blood flow increases up to 25x)
5. Summary Comparison Table
| Parameter | Rest | Moderate Exercise | Maximal Exercise |
|---|---|---|---|
| Heart Rate | 60-80 bpm | ~120-140 bpm | 170-190+ bpm |
| Stroke Volume | ~70 mL | ~100-120 mL | ~110-130 mL (plateaus) |
| Cardiac Output | ~5 L/min | ~15-18 L/min | ~20-30 L/min |
| Dominant mechanism | Vagal tone maintains low HR | Both HR and SV rise | HR continues rising; SV plateaus |
| Sympathetic tone | Low | Moderate | Very high |
6. Key Formulas
- CO = SV × HR
- SV = EDV - ESV (EDV = end-diastolic volume; ESV = end-systolic volume)
- Ejection Fraction = SV / EDV (normal ≥55%)
- Cardiac Index = CO / Body Surface Area (normal ~2.5-4.0 L/min/m²)
- Max HR (approx) = 220 - age (in years)
Sources:
- Costanzo Physiology 7th Edition, pp. 155-156
- Guyton & Hall Textbook of Medical Physiology, Chs. 21 & 85
- Medical Physiology - Boron & Boulpaep, Ch. 25
This is a shared conversation. Sign in to Orris to start your own chat.