Saccadic intrusions
Reading File
Finding Sources
Finding Sources
Searching PubMed
"saccadic intrusions"[MeSH Terms] OR "saccadic intrusions"[tiab]
Reading File
Reading File
Reading File
Reading File
Searching Images
saccadic intrusions square wave jerks opsoclonus ocular flutter eye movements
Reading File
I now have comprehensive content. Here is a structured synthesis:
Saccadic Intrusions
Definition
Saccadic intrusions are spontaneous, involuntary saccadic eye movements that interrupt steady fixation, distinct from nystagmus in which the initial disturbing movement is a slow drift (slow phase). In saccadic intrusions, an inappropriate fast saccade takes the eye off the fixation target — nystagmus begins with a slow phase, intrusions begin with a fast one.
Most types cause oscillopsia (the visual world appears to oscillate) and may require treatment. Square-wave jerks are a notable exception — usually asymptomatic.
Classification: The Key Distinction
The fundamental classification is based on whether an intersaccadic interval (pause) exists between the pair of back-to-back saccades:
| Feature | With Intersaccadic Interval | Without Intersaccadic Interval |
|---|---|---|
| Types | SWJs, SWPs, MSOs | Ocular flutter, opsoclonus, saccadic pulses |
| Mechanism | Supratentorial trigger (for SWJs) | Brainstem/cerebellar EBN disinhibition |
| Symptom | Usually asymptomatic (SWJs) | Oscillopsia |
Types With Intersaccadic Interval
1. Square-Wave Jerks (SWJs)
- Definition: Paired saccades of small amplitude (~2°) that move the eye off-target, pause for ~150–200 ms, then return; occur spontaneously.
- Normal variant in elderly, in darkness, and in carriers of blue-cone monochromatism.
- Prominent in: PSP, multiple system atrophy (MSA), Lewy body disease, olivopontocerebellar atrophy (OPCA), Parkinson disease, MS (cerebellar), Friedreich ataxia, Wernicke encephalopathy, schizophrenia, lithium toxicity.
- Clinically, increased frequency of SWJs in PSP, MSA, and OPCA may help distinguish these from idiopathic PD.
- The intersaccadic interval suggests supratentorial triggering (unlike flutter/opsoclonus which are brainstem/cerebellar in origin).
2. Square-Wave Pulses (SWPs) / Macro–Square-Wave Jerks
- Larger amplitude (10–40°), shorter latency (~80 ms) before return.
- Associated with MS and olivopontocerebellar degeneration; may accompany rubral tremor.
3. Macrosaccadic Oscillations (MSOs)
- Runs of horizontal saccades around the midline with crescendo-decrescendo amplitude pattern.
- Represent caudal fastigial nucleus disease — the extreme end of cerebellar saccadic hypermetria.
- Present in light (not darkness), unlike SWJs.
Types Without Intersaccadic Interval
4. Ocular Flutter
- Intermittent bursts of back-to-back conjugate saccades, limited to the horizontal plane.
- No intersaccadic pause (back-to-back saccades).
- Associated with cerebellar disease.
- Flutter dysmetria ("fish-tail nystagmus"): flutter occurring at the end of a saccade; differs from dysmetria in that consecutive saccades have no intersaccadic interval.
- Ocular microflutter (microsaccadic ocular flutter): small-amplitude variant requiring magnification; patients complain of "shimmering" vision; may be benign or herald cerebellar degeneration, MS, or occult neoplasm.
5. Opsoclonus ("Saccadomania")
- Rapid conjugate movements in horizontal, vertical, and torsional directions — chaotic, continuous bursts without an intersaccadic pause.
- Persist with eyes closed and often continue in sleep.
- Made worse by voluntary movement or attempted fixation.
- Frequently accompanied by myoclonus and ataxia (opsoclonus-myoclonus syndrome).
Causes of opsoclonus:
| Setting | Key Causes |
|---|---|
| Children | Neuroblastoma (evaluate with MIBG/urine catecholamines); responsive to ACTH |
| Adults | Paraneoplastic (lung, breast, testicular cancer); anti-Ri, anti-Hu, anti-Yo antibodies (often absent) |
| Infectious/parainfectious | Viral encephalitis, post-streptococcal, HIV, West Nile virus, rickettsial |
| Toxic/metabolic | Amitriptyline, cocaine, lithium, organophosphates, haloperidol, thallium, hyperosmolar coma |
| Other | Whipple disease (with oculomasticatory myorhythmia), Hashimoto encephalopathy, MS, sarcoid, pontine hemorrhage |
6. Saccadic Pulses / Double Saccadic Pulses
- Saccadic pulse: a stepless saccade interrupting fixation, followed by a slow drift back (glissade) — "pulse without step."
- Double saccadic pulse: two back-to-back saccades (fragment of flutter).
Pathophysiology
The unifying mechanism for flutter and opsoclonus is disinhibition of excitatory burst neurons (EBNs) in the brainstem paramedian pontine reticular formation (PPRF). EBNs have an inherent tendency to oscillate due to:
- Postinhibitory rebound firing (membrane properties)
- Reciprocal synaptic feedback loops
The normal brake on EBNs is provided by omnipause neurons (OPNs) in the nucleus raphe interpositus. Dysfunction of the cerebellum–inferior olive–EBN circuit (possibly via altered GABA-A receptor sensitivity) allows burst neurons to fire in an uncontrolled oscillatory fashion. Bilateral pretectal lesions in primates can reproduce similar movements experimentally.
For SWJs, the mechanism is distinct — they are thought to be triggered supratentorially, with the longer intersaccadic interval reflecting this different origin.
Clinical Assessment
Key points on exam:
- Observe fixation under direct illumination and with ophthalmoscope.
- Provoke by gaze shifts (saccadic intrusions are often precipitated by refixation movements).
- Determine whether oscillations are present in darkness (SWJs are not; flutter/opsoclonus may worsen).
- Assess for associated myoclonus, ataxia, torticollis (spasmus nutans triad).
- Evaluate for oscillopsia (symptom of flutter/opsoclonus, absent with SWJs).
EOG Recording Appearance
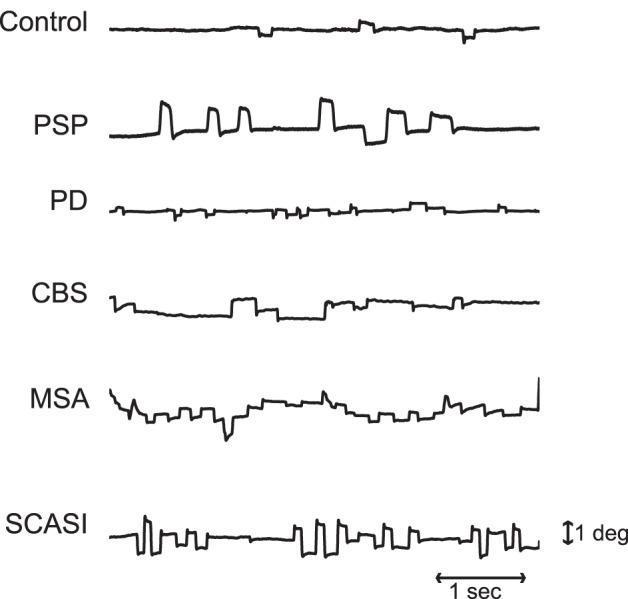
EOG recordings of horizontal eye position showing SWJs across conditions: healthy control (minimal), PSP (high-amplitude frequent SWJs), PD/CBS (lower amplitude), MSA (intrusions + drift), and SCASI (most frequent/high-amplitude oscillations).
Treatment Pearls
- SWJs: usually require no treatment.
- Opsoclonus in children (neuroblastoma): ACTH or corticosteroids; IVIg, rituximab.
- Paraneoplastic opsoclonus in adults: treat underlying malignancy; immunotherapy often disappointing.
- Square-wave oscillations (SWJ runs from cerebellar injury): may respond to memantine.
- Ocular flutter/opsoclonus (cerebellar): clonazepam, memantine, or gabapentin may reduce symptoms.
- Ocular neuromyotonia (post-radiation): carbamazepine.
Quick Reference: Differential by Pattern
| Pattern | Key Diagnosis |
|---|---|
| Frequent SWJs + supranuclear gaze palsy | PSP |
| Opsoclonus + myoclonus + ataxia in child | Neuroblastoma |
| Opsoclonus + ataxia + emotional lability in adult | Paraneoplastic (screen for lung/breast/testis) |
| Flutter after saccade endpoint | Flutter dysmetria (cerebellar) |
| Ocular microflutter + "shimmering" vision | Cerebellar degeneration, MS, or occult neoplasm |
| SWPs + rubral tremor | MS / olivopontocerebellar degeneration |
Sources: Bradley and Daroff's Neurology in Clinical Practice; Adams and Victor's Principles of Neurology, 12e; Localization in Clinical Neurology, 8e.
This is a shared conversation. Sign in to Orris to start your own chat.