What is rutf
RUTF ready-to-use therapeutic food severe acute malnutrition
"ready-to-use therapeutic food" AND "severe acute malnutrition"
RUTF - Ready-to-Use Therapeutic Food
What is it?
Composition
- Energy: ~500 kcal
- Protein: ~13g (largely from milk powder and peanut paste)
- Fat: ~26-31g (mainly peanut oil and palm oil)
- Vitamins & minerals: Full spectrum including zinc, iron, vitamin A, vitamin C, vitamin D, B-complex
- Water activity is very low - this means it does not require refrigeration and has a long shelf life (~2 years), which is critical for use in resource-limited settings
Why RUTF Changed Treatment
- Only children with medical complications (infection, edema, poor appetite) now need hospitalization
- Caregivers can administer treatment at home
- Far more children can be reached at lower cost
Effectiveness
- ~90% recovery rate in children with uncomplicated SAM
- Full nutritional recovery typically in 4-8 weeks
- Endorsed by the WHO, UNICEF, WFP, and UNHCR as the standard of care for outpatient SAM treatment
- UNICEF procures and distributes RUTF globally; in 2023 alone, Action Against Hunger treated 355,000 children with SAM using RUTF
How It Is Used
- Child is screened for SAM using mid-upper arm circumference (MUAC) or weight-for-height Z-score
- If no medical complications, child is enrolled in outpatient therapeutic program (OTP)
- Caregiver receives weekly or bi-weekly supply of RUTF sachets
- Child eats directly from the sachet - no water or cooking required
- Child is monitored weekly for weight gain and appetite
Ongoing Research
Key Facts at a Glance
| Feature | Detail |
|---|---|
| Target population | Children 6 months - 5 years with SAM |
| Basis | Peanut paste + milk powder + oil + vitamins/minerals |
| WHO standard | Yes - endorsed for outpatient SAM treatment |
| Shelf life | ~2 years, no refrigeration needed |
| Recovery rate | ~90% within 4-8 weeks |
| Main brand | Plumpy'Nut (Nutriset, France) |
What is resomal
ReSoMal rehydration solution malnutrition composition WHO
https://medicalguidelines.msf.org/en/viewport/EssDr/english/…
ReSoMal - Rehydration Solution for Malnutrition
What is it?
Why Standard ORS is Dangerous in SAM
- Depleted intracellular potassium - cells have lost potassium and filled with sodium
- Impaired kidney function - cannot handle sodium loads normally
- Compromised cardiac function - at risk of heart failure with fluid overload
- Hyponatraemia on admission is actually a risk factor for poor outcome in SAM with diarrhoea (paradoxically, despite body sodium excess)
Composition (per litre)
| Electrolyte | ReSoMal | Standard WHO-ORS |
|---|---|---|
| Sodium | 45 mmol/L | 75 mmol/L |
| Potassium | 40 mmol/L | 20 mmol/L |
| Chloride | 76 mmol/L | 65 mmol/L |
| Glucose | 125 mmol/L | 75 mmol/L |
| Osmolarity | ~300 mOsm/L | 245 mOsm/L |
| + Magnesium, Zinc, Copper | Yes | No |
Dosing Protocol (WHO)
- 5 ml/kg after each loose stool
- 5 ml/kg every 30 minutes for 2 hours
- Then 5-10 ml/kg/hour, alternating ReSoMal with F-75 therapeutic milk for 4-10 hours
- Oral or nasogastric route at 5 ml/kg every 30 minutes for 2 hours, then alternate with F-75
Important Precautions
- Never use in circulatory shock - requires IV fluids first
- Monitor closely for signs of fluid overload: rising respiratory rate, increasing oedema, puffy eyelids
- Hyponatraemia can paradoxically occur with ReSoMal use - reported in studies, with some children developing severe hyponatraemia and convulsions
- Do not use standard ORS as a substitute in SAM
- Prepared solution must be used within 24 hours
Clinical Context
- F-75 (starter therapeutic milk, low protein/energy) in the stabilization phase
- F-100 or RUTF in the rehabilitation phase
Key Facts
| Feature | Detail |
|---|---|
| Full name | REhydration SOlution for MALnutrition |
| Target | Children with SAM + diarrhoea + dehydration |
| WHO endorsed | Yes |
| Sodium content | 45 mmol/L (low) |
| Potassium content | 40 mmol/L (high) |
| Given with | Alternated with F-75 therapeutic milk |
| Risk to watch | Fluid overload, hyponatraemia |
What nutrition recovery syndrome
nutrition recovery syndrome refeeding syndrome malnutrition pathophysiology management
Nutrition Recovery Syndrome (Refeeding Syndrome)
Pathophysiology
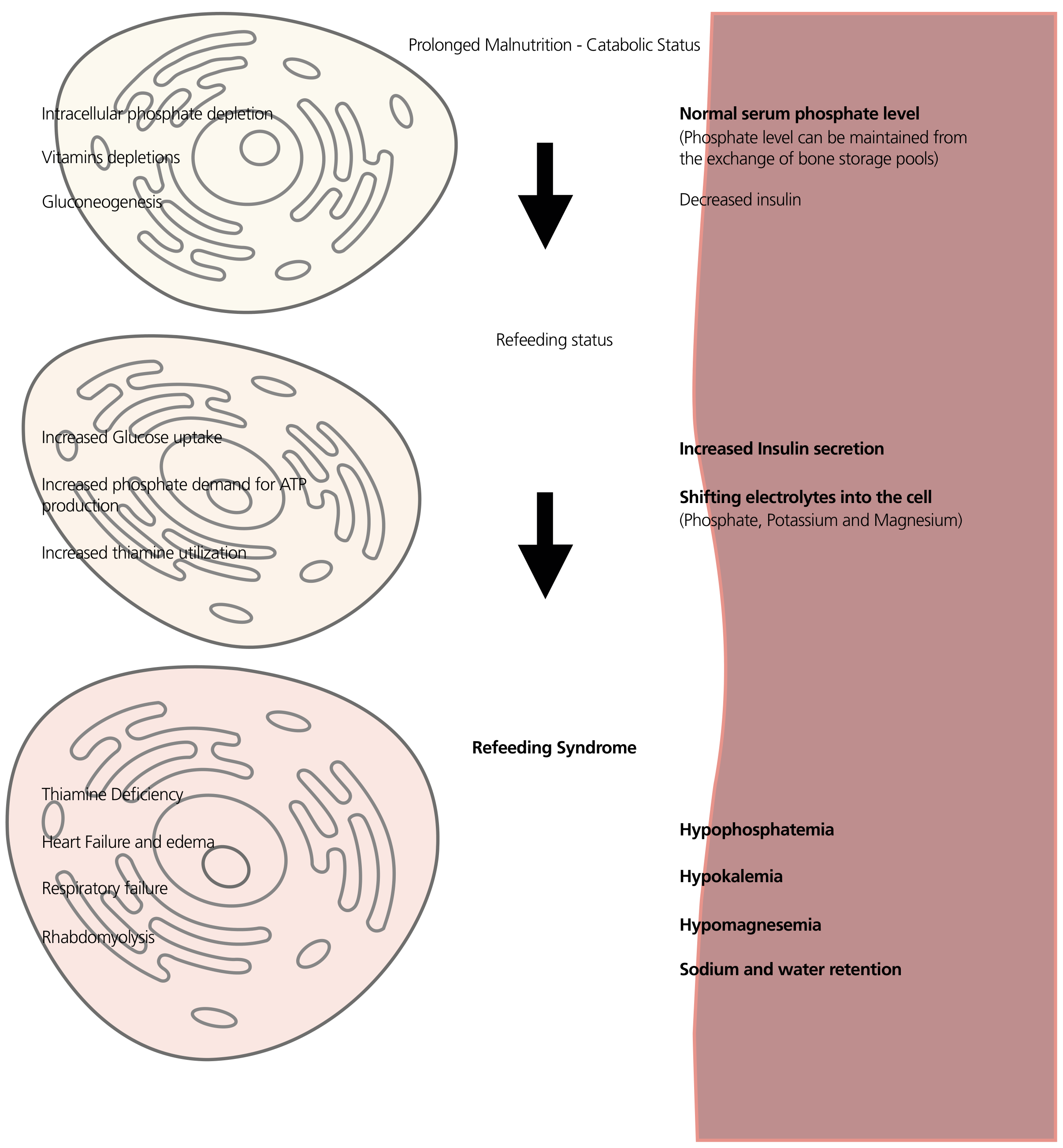
- The body switches to fat and amino acids as fuel (gluconeogenesis)
- Intracellular phosphate, potassium, magnesium, and vitamins are depleted
- But serum levels can appear normal - the body borrows from bone and other stores to maintain blood levels
- Insulin secretion is low
- Carbohydrates become the main fuel again
- This triggers a surge in insulin secretion
- Insulin activates Na-K ATPase pumps, driving potassium, phosphate, and magnesium from the blood into cells
- Phosphate is also consumed in glycolysis (needed for ATP production)
- Thiamine demand increases sharply (it is a cofactor for pyruvate dehydrogenase - without it, pyruvate cannot enter the Krebs cycle)
- Sudden, severe hypophosphatemia, hypokalemia, hypomagnesemia
- Sodium and water retention
- Thiamine deficiency
Clinical Features / Complications
| System | Manifestation |
|---|---|
| Cardiac | Arrhythmias, heart failure, edema |
| Respiratory | Respiratory failure (diaphragm weakness) |
| Neurological | Confusion, Wernicke's encephalopathy (thiamine deficiency), seizures |
| Muscular | Rhabdomyolysis, weakness |
| Haematological | Haemolytic anaemia |
| Metabolic | Hyperglycaemia (blunted insulin in severe cases) |
Who is at Risk?
- Prolonged starvation or fasting
- Severe acute malnutrition (SAM) in children
- Anorexia nervosa
- Chronic alcoholism
- Delayed or absent nutritional support in ICU patients
- Massive weight loss
- Patients with chronic diarrhoea or fistulas (electrolyte losses)
- Patients on diuretics or insulin
ASPEN Diagnostic Criteria
- Mild: decrease of 10-20%
- Moderate: decrease of 20-30%
- Severe: decrease of >30% and/or organ dysfunction, or thiamine deficiency
Prevention and Management
- Correct electrolyte deficits before starting feeding - replete potassium, phosphate, and magnesium first
- Give thiamine before feeding begins - to prevent Wernicke's encephalopathy
- Start feeding slowly - begin at 50% of caloric target (or <10 kcal/kg/day in very high-risk patients)
- Gradually increase over 5-7 days up to full target
- Monitor closely - daily electrolytes (phosphate, potassium, magnesium), fluid balance, vital signs, blood glucose
- Correct deficits aggressively as they appear
Key Takeaway
| Feature | Detail |
|---|---|
| Trigger | Rapid refeeding after starvation/malnutrition |
| Hallmark | Hypophosphatemia (+ hypokalemia, hypomagnesemia) |
| Mechanism | Insulin surge → electrolytes shift into cells |
| Key danger | Cardiac arrhythmia, respiratory failure, death |
| Prevention | Slow refeeding + thiamine + electrolyte correction first |
| First described | Post-WWII Japanese POW camps |
- Yamada's Textbook of Gastroenterology, p. 548
- Schwartz's Principles of Surgery, 11th ed., p. 126
What is appetite test
appetite test severe acute malnutrition RUTF procedure pass fail criteria WHO CMAM
https://www.open.edu/openlearncreate/mod/oucontent/view.php?…
appetite test SAM children RUTF grams per kg body weight pass criteria table
https://www.researchgate.net/publication/337910105_Critical_…
The Appetite Test
What is it?
- Treated as an outpatient (OTP - Outpatient Therapeutic Programme) - if they pass
- Admitted for inpatient care - if they fail
Why Appetite Matters in SAM
How to Conduct the Appetite Test
- Find a quiet, comfortable area - the mother/caregiver should be present and seated comfortably with the child on their lap
- Explain the procedure to the caregiver
- Wash hands - both health worker and caregiver
- Offer a known amount of RUTF to the child (see table below)
- Allow up to 30 minutes for the child to eat
- Encourage gently - do NOT force-feed
- Offer clean drinking water alongside the RUTF
- Observe and measure how much the child eats
Pass/Fail Criteria
| Body weight (kg) | Minimum to PASS (approx.) |
|---|---|
| 3-3.9 kg | 15-20 g |
| 4-4.9 kg | 20-25 g |
| 5-6.9 kg | 25-35 g |
| 7-8.9 kg | 35-45 g |
| 9-10.9 kg | 45-55 g |
| ≥ 11 kg | ≥ 55 g |
Outcome of the Test
| Result | Meaning | Action |
|---|---|---|
| PASS - eats required amount willingly | Good appetite, no severe complications | Enroll in outpatient OTP with RUTF at home |
| FAIL - refuses or cannot eat enough | Poor appetite, likely complicated SAM | Admit for inpatient care (stabilisation with F-75) |
Who Should NOT be Sent Outpatient Even if They Pass?
- Severe bilateral oedema (grade +++)
- Any general danger sign (unconscious, unable to drink, convulsions, vomiting everything)
- Medical complication: severe anaemia, respiratory distress, severe dehydration, high fever, hypoglycaemia
- Age < 6 months
Clinical Significance
"Children who have an appetite (pass the appetite test) and are clinically well and alert should be treated as outpatients for uncomplicated severe acute malnutrition."
Summary
| Feature | Detail |
|---|---|
| Purpose | Triage SAM children for inpatient vs. outpatient care |
| Tool used | RUTF (peanut paste sachet) |
| Duration | Up to 30 minutes |
| Pass threshold | ~5 g RUTF/kg body weight eaten willingly |
| Pass = | Outpatient OTP |
| Fail = | Inpatient stabilisation (F-75) |
| Done by | Health worker or trained community worker |
What is f75 and f100diet
F-75 F-100 therapeutic milk diet severe acute malnutrition composition WHO stabilisation rehabilitation phase
F-75 and F-100 Therapeutic Milk Diets
Nutritional Composition (per 100 mL)
| Nutrient | F-75 | F-100 | RUTF (per 100g) |
|---|---|---|---|
| Energy (kcal) | 75 | 100 | 543 |
| Protein (g) | 0.9 | 2.9 | 13.6 |
| Lactose (g) | 1.3 | 4.2 | - |
| Potassium (mg) | 156 | 246 | 1111 |
| Sodium (mg) | 14 | 44 | 189 |
| Magnesium (mg) | 10.5 | 17.7 | 92 |
| Zinc (mg) | 2.0 | 2.3 | 14 |
| Copper (mg) | 0.25 | 0.25 | 1.78 |
| Osmolarity | 413 mOsm/L | 419 mOsm/L | - |
| % energy from protein | 5% | 12% | 10-12% |
| % energy from fat | 36% | 53% | 45-60% |
- Goldman-Cecil Medicine, International Edition, Table 197-1
F-75 - The Stabilisation Diet
Purpose
When Used
- Phase 1: Stabilisation - typically the first 1-7 days of inpatient care
- Used in children who:
- Failed the appetite test
- Have medical complications (infection, severe oedema, hypoglycaemia)
- Are too ill or weak to tolerate full nutrition
Why Low Protein?
Key Features
- 75 kcal / 100 mL - deliberately restricted energy
- Very low sodium (14 mg/100 mL) - prevents fluid overload in a child with abnormal sodium metabolism
- Low lactose - reduces risk of lactose intolerance (common in SAM)
- Given in small frequent feeds (every 2-3 hours, day and night) at 100 mL/kg/day
- Can be given by nasogastric (NG) tube if child cannot drink
Goal
F-100 - The Rehabilitation Diet
Purpose
When Used
- Phase 2: Rehabilitation - after the child passes the transition criteria
- Transition from F-75 to F-100 is made when:
- Oedema is resolving
- Appetite has returned
- Medical complications are resolving
- Child is alert and active
Key Features
- 100 kcal / 100 mL - higher energy density
- 2.9 g protein / 100 mL - much higher protein to rebuild muscle mass
- Higher fat content (53% of energy from fat)
- Given at approximately 150-220 kcal/kg/day to achieve catch-up growth
- Target weight gain: >5 g/kg/day (ideally 10-15 g/kg/day)
Goal
The Treatment Phases in SAM
ADMISSION
↓
Phase 1: STABILISATION (F-75)
- Duration: ~1-7 days
- Goal: Correct hypoglycaemia, hypothermia, dehydration, electrolytes
- Diet: F-75 every 2-3 hours
↓
TRANSITION (F-75 → F-100 or RUTF)
- Child passes appetite test
- Oedema improving
↓
Phase 2: REHABILITATION (F-100 or RUTF)
- Duration: ~2-6 weeks (inpatient or outpatient)
- Goal: Rapid catch-up weight gain
- Diet: F-100 or RUTF
↓
DISCHARGE when weight-for-height ≥ -2 SD (or MUAC ≥ 125mm)
F-75 vs F-100 - Key Differences at a Glance
| Feature | F-75 | F-100 |
|---|---|---|
| Phase | Stabilisation (Phase 1) | Rehabilitation (Phase 2) |
| Calories | 75 kcal/100 mL | 100 kcal/100 mL |
| Protein | 0.9 g/100 mL (low) | 2.9 g/100 mL (high) |
| Goal | Metabolic stability, NOT weight gain | Rapid weight gain |
| Volume/day | ~100 mL/kg/day | ~150-220 kcal/kg/day |
| Risk prevented | Refeeding syndrome, fluid overload | Used once risk has passed |
| Frequency | Every 2-3 hours (8-12 feeds/day) | Every 3-4 hours |
Important Notes
-
Never start with F-100 in a newly admitted SAM child - this risks fatal refeeding syndrome
-
Iron is withheld during the stabilisation phase and only introduced in rehabilitation (iron promotes bacterial growth and is dangerous in acute illness)
-
If RUTF is available and the child has appetite, F-100 can be replaced with RUTF in the rehabilitation phase for outpatient treatment
-
Both F-75 and F-100 can be prepared locally from basic ingredients (dried skim milk, sugar, vegetable oil, mineral/vitamin mix) or purchased as commercial powder (e.g. Nutriset's products)
-
Goldman-Cecil Medicine, International Edition, Table 197-1
-
Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 2158