Which antibiotics are safe in pregnancy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"antibiotic" AND "pregnancy" AND "safety"
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive data from Rosen's Emergency Medicine. I have everything needed to give a thorough, well-structured answer.
Antibiotics in Pregnancy
Antibiotic selection in pregnancy requires balancing the risk of untreated infection (preterm labor, spontaneous abortion, low birth weight) against potential drug toxicity to the mother and fetus. Gestational age matters - many agents that are acceptable in the second or third trimester carry higher risk in the first trimester when organogenesis is occurring.
Generally SAFE Antibiotics
Penicillins ✅
First- to fourth-generation penicillins and derivatives (ampicillin, amoxicillin, piperacillin, clavulanate, sulbactam, tazobactam) are the drugs of first choice in pregnancy. They have long-standing safety data and are compatible with breast-feeding.
- Rosen's Emergency Medicine, 9e
Cephalosporins ✅
All generations (1st through 4th) are considered safe. First-generation cephalosporins have the most data; some conflicting evidence exists for first-trimester use of 1st generation specifically. Compatible with breast-feeding.
- Rosen's Emergency Medicine, 9e (Table 175.6)
Macrolides ✅ (with caveats)
- Azithromycin - preferred macrolide; safe in pregnancy
- Erythromycin - safe but the estolate salt (not the base or stearate) can cause hepatotoxicity in pregnant women; avoid that formulation
- Clarithromycin - more limited data; azithromycin is preferred
- Use of erythromycin in infancy has been associated with pyloric stenosis (note: this is a neonatal, not fetal, concern)
Clindamycin ✅
No reports of fetal toxicity or malformations. Compatible with breast-feeding. Useful for GBS prophylaxis in penicillin-allergic patients.
Nitrofurantoin ✅ (second and third trimester only)
Historically considered safe throughout pregnancy, but recent literature associates first-trimester use with congenital abnormalities. Avoid in the first trimester and near term (risk of hemolytic anemia in G6PD-deficient neonates). Useful for uncomplicated UTI in mid-pregnancy.
Metronidazole ✅ (with caution)
Generally compatible. Though it is an in vitro mutagen, clinical studies have not confirmed teratogenicity. Most guidelines consider it acceptable after the first trimester. The AAP recommends temporary cessation of breast-feeding during use.
Vancomycin ✅
Not linked to birth defects in humans or animals. Reports of neonatal auditory and renal abnormalities have not been confirmed on retesting. Used for serious gram-positive infections (e.g., MRSA) when alternatives are unavailable.
Aminoglycosides ⚠️ (with caution)
No proven structural teratogenicity, but streptomycin and kanamycin carry a low risk of ototoxicity. Gentamicin is nephrotoxic and ototoxic at high doses. Use only when clearly indicated and with careful dosing. Generally reserved for serious infections.
Antibiotics to AVOID
| Antibiotic | Reason |
|---|---|
| Tetracyclines (tetracycline, doxycycline) | Chelates calcium - causes bone growth abnormalities and permanent staining of deciduous teeth; tetracycline linked to fatal fatty liver in pregnant women; associated with GU anomalies and limb defects |
| Fluoroquinolones (ciprofloxacin, levofloxacin) | Arthrotoxicity (cartilage damage) concerns; risk of cardiac defects in first trimester; avoid especially in first trimester |
| Sulfonamides / TMP-SMX (Bactrim) | Trimethoprim is a folate antagonist - risk of neural tube defects, cleft palate, cardiovascular and urinary tract malformations; sulfonamides near term cause kernicterus |
| Chloramphenicol | Risk of grey baby syndrome; idiosyncratic bone marrow suppression |
| Linezolid | No pregnancy safety data; use with extreme caution |
Summary by Trimester
| Trimester | Preferred Agents |
|---|---|
| 1st (organogenesis) | Penicillins, cephalosporins, azithromycin, clindamycin |
| 2nd & 3rd | All of the above plus nitrofurantoin, metronidazole |
| Near term | Avoid sulfonamides (kernicterus), nitrofurantoin (hemolysis) |
Clinical rule: The penicillins, cephalosporins, and macrolides are the drugs of choice for infections during pregnancy. Alternative classes are prescribed only if these fail or there is severe maternal intolerance. - Rosen's Emergency Medicine: Concepts and Clinical Practice, 9e
Important note: No drug is absolutely risk-free in pregnancy. Always weigh the risk of untreated infection against drug risk, as untreated infections in pregnancy are themselves a major cause of preterm labor and low birth weight.
Treatment of fever
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"fever" AND "children" AND "antipyretic"
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, textbook-sourced information to deliver a thorough answer. Here it is:
Treatment of Fever in Children (Pediatric)
What is Fever?
Fever in children is defined as a rectal temperature ≥38.0°C (100.4°F). The goal of treatment is to relieve the discomfort associated with fever - not to normalize the temperature itself. The underlying cause must always be investigated.
Antipyretic Drugs
These are the two first-line agents. They work by inhibiting prostaglandin synthesis, lowering the hypothalamic set-point.
1. Paracetamol (Acetaminophen)
| Parameter | Details |
|---|---|
| Dose | 10-15 mg/kg/dose PO every 4-6 hours |
| Route | Oral preferred; rectal (10-20 mg/kg) if vomiting |
| Max single dose | 15 mg/kg |
| Max daily dose | Lesser of 75 mg/kg or 4,000 mg; no more than 5 doses/day |
| Age | All ages including neonates (with weight-based dosing) |
| IV form | Available (10 mg/mL); use when NPO - more expensive |
Key points:
- No anti-inflammatory effect
- Hepatotoxicity is the major concern - almost always from excessive dosing
- Many OTC formulations exist (160 mg/5 mL suspension, 80 mg chewables, etc.) - they are NOT interchangeable; always confirm formulation and concentration
2. Ibuprofen
| Parameter | Details |
|---|---|
| Dose | 5-10 mg/kg/dose PO every 6-8 hours |
| Age | Minimum age: 6 months (avoid in younger due to immature renal development) |
| Max single dose | 400 mg |
| Max daily dose | Up to 1,600 mg/day |
Key points:
- Has both antipyretic and anti-inflammatory effects
- Avoid in children with dehydration, renal disease, or known GI issues
- A 2024 systematic review found no significant risk of asthma exacerbation in children using ibuprofen (PMID: 39187775)
- Slightly longer duration of action than paracetamol; may be preferred for fever requiring less frequent dosing
Alternating Paracetamol and Ibuprofen?
Alternating the two agents is commonly practiced to avoid overdose and extend fever control. While it may offer slightly better temperature control, it increases caregiver complexity and the risk of dosing errors. Current guidance does not recommend it as routine.
What NOT to Use
| Drug | Reason |
|---|---|
| Aspirin (Salicylates) | Contraindicated under age 15 during viral illness - risk of Reye syndrome (rare but fatal liver/brain damage) |
| Codeine/opioids | Not indicated for fever; codeine is contraindicated in children due to unpredictable CYP2D6 metabolism |
Non-Pharmacological Measures
- Tepid sponging / cool baths: Not routinely recommended - they cause discomfort and shivering without proven benefit when added to antipyretics. Do not use cold water or alcohol rubs.
- Adequate fluids: Encourage oral hydration to prevent dehydration
- Light clothing: Avoid over-bundling
- Rest: Comfortable environment
Management by Age Group
Neonates (<28 days) and Young Infants (28-90 days)
Fever in this group is a medical emergency until proven otherwise. The immune system is immature and bacterial infections are hard to distinguish from viral clinically.
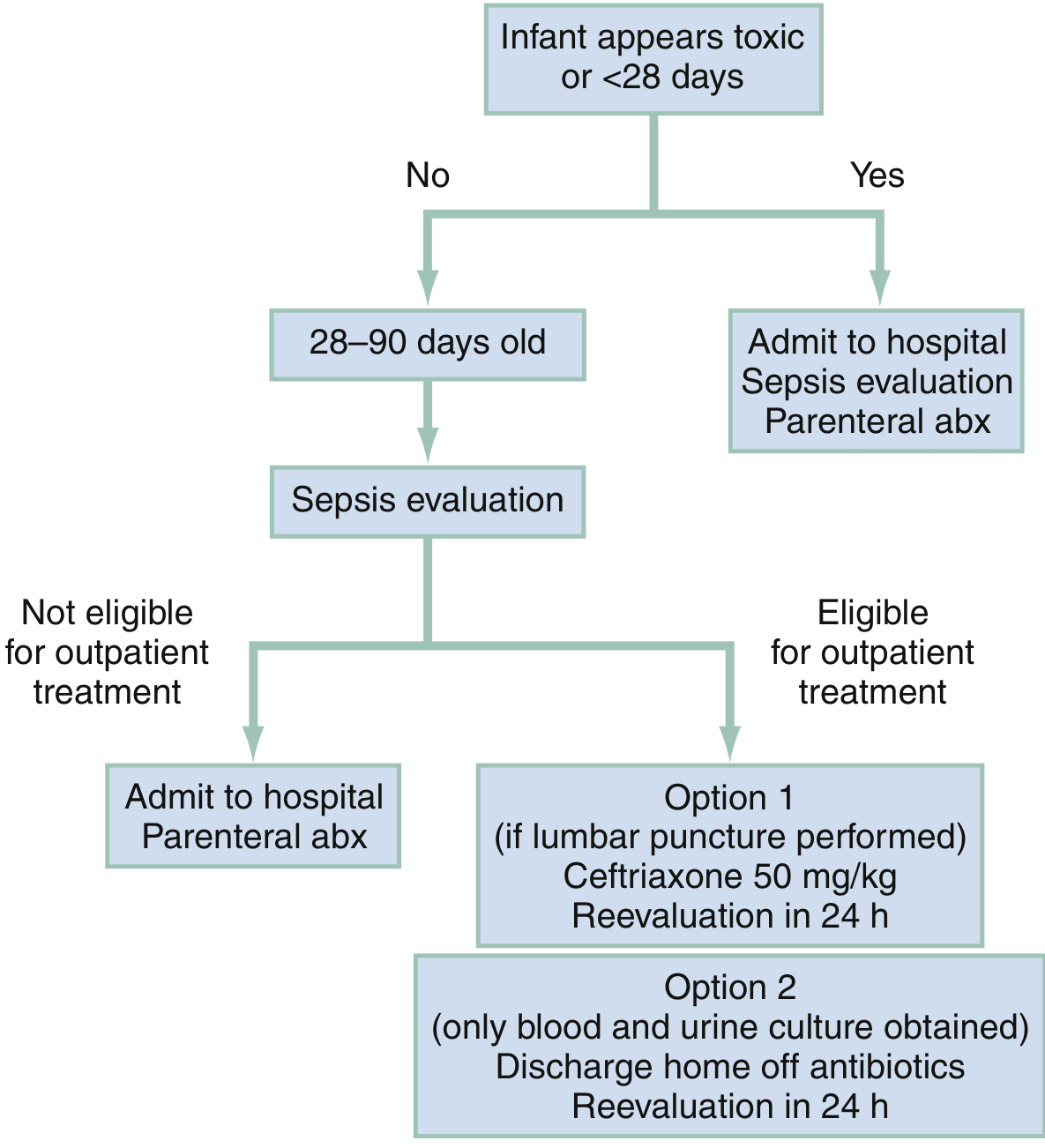
- Any infant <28 days with fever, or any infant appearing toxic: Admit + full sepsis evaluation + parenteral antibiotics
- 28-90 days, non-toxic: Full sepsis workup; if eligible for outpatient treatment, can discharge with ceftriaxone 50 mg/kg + reevaluation in 24 hours OR discharge home off antibiotics with reevaluation in 24 hours
Children 3-36 Months
- Most fever is due to self-limited viral illness (URI, roseola, gastroenteritis)
- Since widespread PCV13 immunization, occult bacteremia is now rare - blood cultures are no longer routine in all febrile children; clinical judgment guides selective testing
- Treat discomfort with antipyretics, identify source, and treat underlying cause
Children >36 Months
- Fever is usually localizable to a source by history and exam
- Antipyretics for comfort; investigations and antibiotics only if bacterial cause identified
Febrile Seizures
- Occur in children 6 months to 5 years, risk during rapid rise or fall of fever (not absolute height)
- Simple: <15 minutes, generalized, single episode - benign; no antiepileptics needed
- Complex: Prolonged (>15 minutes), focal, or recurrent within 24 hours - lumbar puncture should be considered
- Risk of epilepsy is only slightly elevated after a febrile seizure (1-2% vs 0.5-1% in general population)
- Routine EEG or neuroimaging is not indicated
- There is no role for prophylactic antipyretics in preventing febrile seizure recurrence
Red Flags - When to Escalate
| Sign | Concern |
|---|---|
| Fever + petechial rash | Meningococcemia (7-11% risk in hospitalized cases) - obtain CBC, CRP, blood culture immediately |
| Fever in <28 days | Admit all for sepsis workup |
| Inconsolable crying / lethargy | CNS infection (meningeal signs may be absent in infants) |
| Fever not responding to antipyretics | Consider bacterial infection |
| Temperature >40°C | Higher risk of serious bacterial infection |
"The penicillins, cephalosporins, and macrolide antibiotics are the drugs of choice for infections during pregnancy...The choice of antimicrobial therapy will depend on the gestational age of the pregnancy, severity of infection..." - Rosen's Emergency Medicine: Concepts and Clinical Practice, 9e
- Rosen's Emergency Medicine, 9e - Table 157.5 (Analgesic dosing), Chapter 161 (Pediatric Fever)
This is a shared conversation. Sign in to Orris to start your own chat.