Describe bilirubin pathaway and classification of jaundice
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-illustrated answer. Let me compile it.
Bilirubin Pathway and Classification of Jaundice
1. Bilirubin: Overview
Bilirubin is the orange-yellow pigment derived from heme, primarily a product of red blood cell (RBC) turnover. Normal adults produce approximately 4 mg/kg/day (~250-350 mg/day total). It is extracted by the liver, biotransformed, and excreted in bile and urine. Beyond its role as a degradation byproduct, bilirubin has recognized antioxidant and immune-modulating properties and acts as a ligand for cellular receptors.
- Goldman-Cecil Medicine, International Edition
- Henry's Clinical Diagnosis and Management by Laboratory Methods
2. The Bilirubin Pathway (Step by Step)
The following diagram from Lippincott's Biochemistry shows the complete pathway:
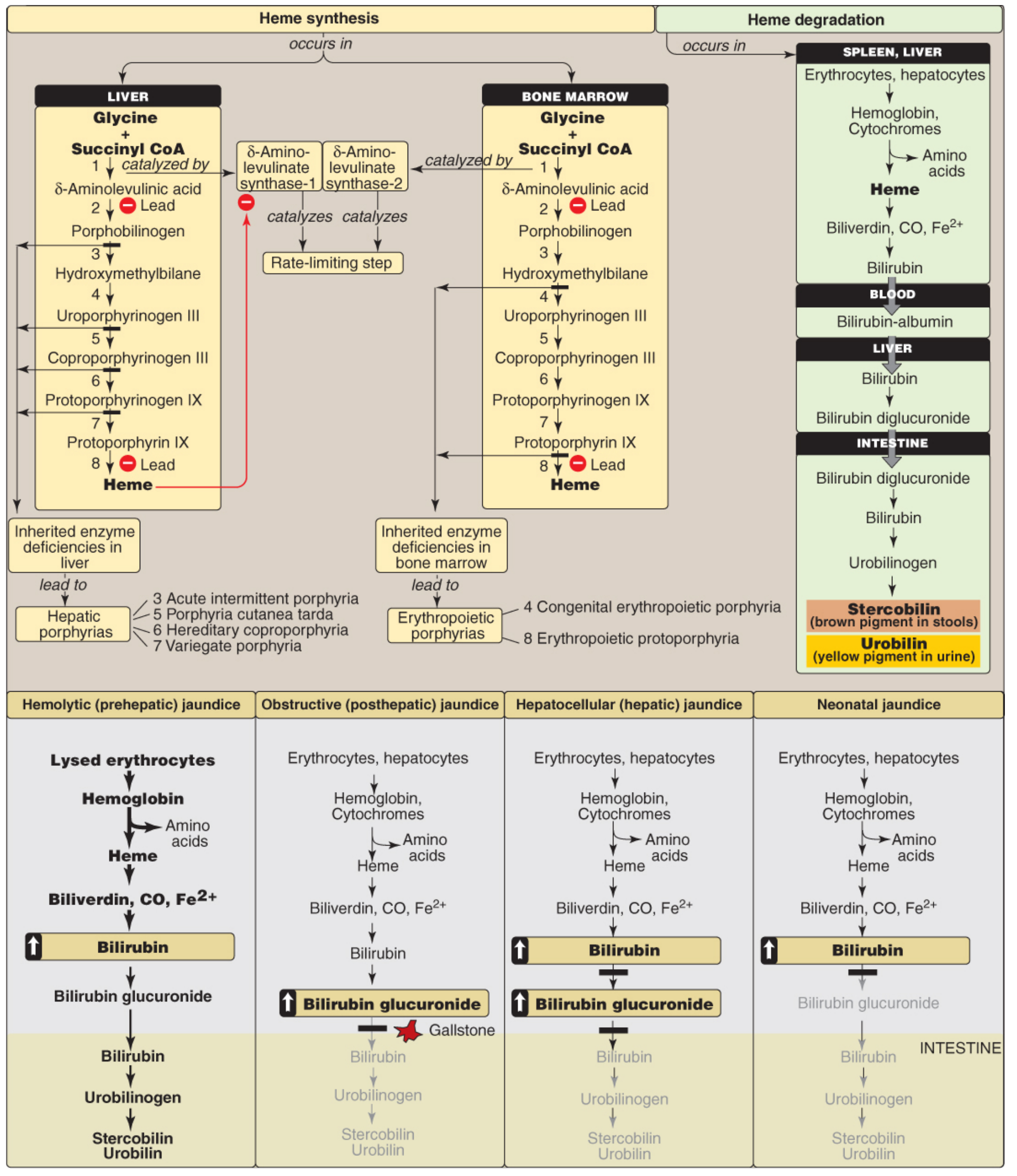
Figure 21.20 - Key concept map for heme metabolism and the types of jaundice (Lippincott's Biochemistry, 8th ed.)
Step 1: Heme Production and Breakdown (Reticuloendothelial System - Spleen/Liver/Bone Marrow)
- 70-90% of bilirubin comes from senescent RBC hemoglobin; the remainder from turnover of non-hemoglobin hemoproteins (myoglobin, cytochrome P-450, catalase, peroxidase), mainly in the liver. A minor fraction comes from ineffective erythropoiesis.
- In macrophages of the spleen (primarily), hemoglobin is split into globin chains and heme.
- Heme is oxidized by microsomal heme oxygenase at the α-bridge carbon, opening the porphyrin ring and producing:
- Biliverdin (green, water-soluble tetrapyrrole)
- Carbon monoxide (CO) (1 mole per mole of heme - transported as carboxyhemoglobin; serum levels help diagnose hemolytic anemia)
- Fe²⁺ (iron, recycled)
- Biliverdin is then reduced to unconjugated bilirubin by NADPH-dependent biliverdin reductase.
Why does biliverdin get reduced to bilirubin in mammals? Because unconjugated bilirubin (unlike biliverdin) can cross the placenta, allowing fetal bilirubin to be excreted by the maternal liver. This is the evolutionary rationale.
Step 2: Transport in Blood
- Unconjugated bilirubin (UCB) is water-insoluble due to its ridge-tile configuration with six intramolecular hydrogen bonds that mask polar groups.
- It is kept in solution by tight but reversible binding to albumin and transported via the portal system to the liver.
- Drugs such as salicylates, sulfonamides, furosemide, and radiographic contrast agents can competitively displace bilirubin from albumin - of little clinical significance in adults, but in neonates this raises the risk of kernicterus.
Step 3: Hepatic Uptake
The following diagram shows the intracellular bilirubin pathway within the hepatocyte:
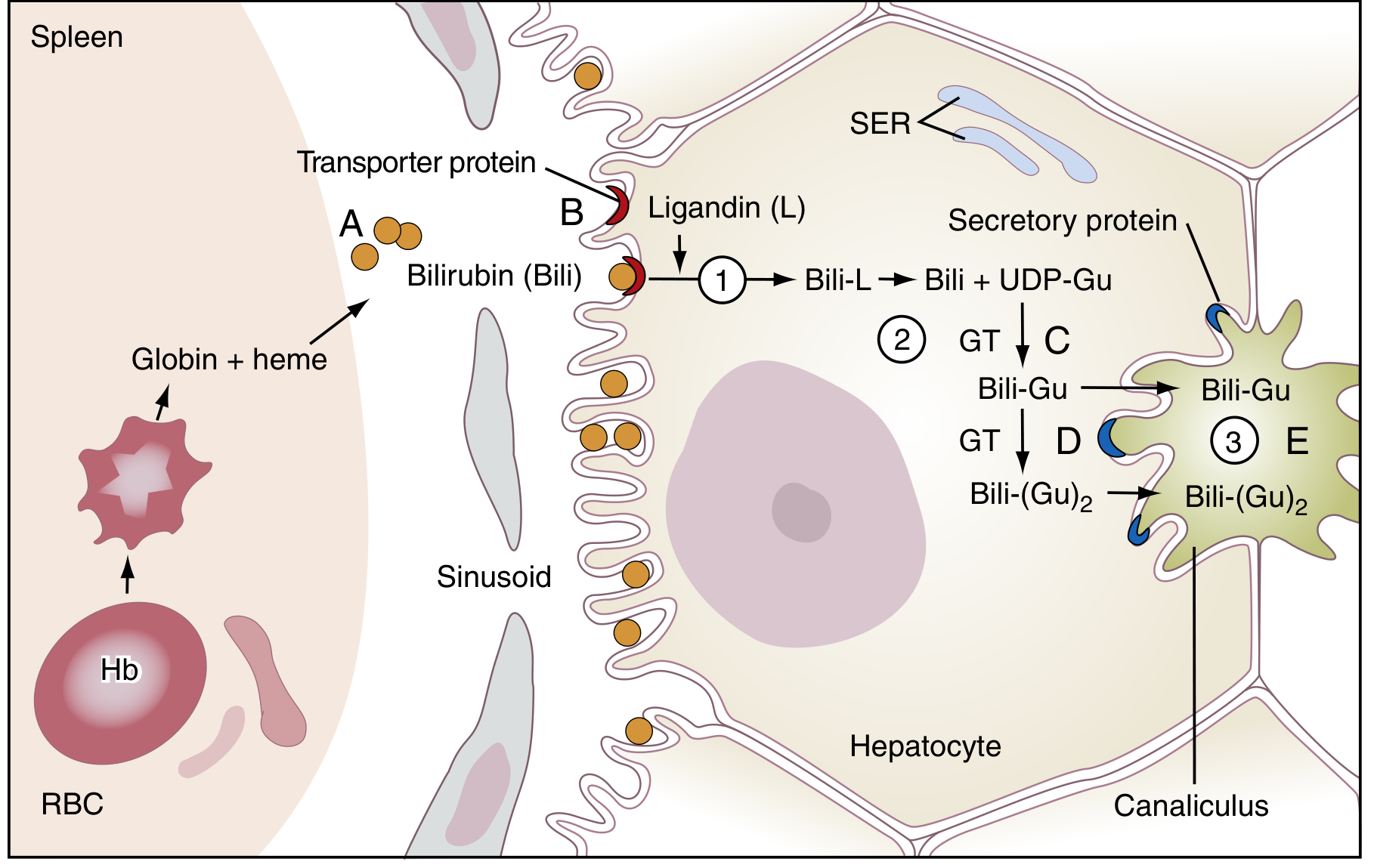
Figure 22.2 - Schematic of bilirubin transport and metabolism from spleen to bile canaliculus (Henry's Clinical Diagnosis, Laboratory Methods)
Hepatic handling involves four distinct steps:
-
Uptake: Principally by facilitated transport (via organic anion transport proteins - OATPs - and Na⁺/taurocholate transporting protein NTCP on the sinusoidal membrane) and, to a lesser extent, passive diffusion. The fenestrated sinusoidal endothelium facilitates access.
-
Intracellular binding: Bilirubin binds sequentially to cytosolic Y and Z proteins (glutathione-S-transferase family), then to ligandin, which chaperones it to the smooth endoplasmic reticulum (SER). This binding also prevents back-diffusion into blood.
-
Conjugation: In the SER, bilirubin is conjugated with glucuronic acid (from UDP-glucuronic acid) by the enzyme UDP-glucuronosyltransferase isoform UGT1A1 (encoded by the UGT1 gene complex). This produces mainly bilirubin diglucuronide (80%), with some monoglucuronide (1:4 mono:di ratio in bile, 1:1 in plasma). Conjugation renders bilirubin water-soluble, allowing biliary excretion.
-
Canalicular secretion: Conjugated bilirubin (CB) is actively transported into bile canaliculi by the ATP-dependent transporter MRP2 (multidrug resistance-associated protein 2, also called cMOAT/ABCC2). When MRP2 capacity is exceeded, MRP3 on the sinusoidal membrane can also secrete CB back into plasma.
Step 4: Intestinal Fate and Enterohepatic Circulation
- Conjugated bilirubin (bilirubin diglucuronide) is secreted into bile and enters the intestinal lumen.
- Intestinal bacteria hydrolyze the glucuronide conjugates and reduce bilirubin to urobilinogen (colorless).
- Most urobilinogen is excreted in feces, oxidized by bacteria to stercobilin (brown color of stool).
- A small fraction (~20%) is reabsorbed from the colon, enters the portal circulation (enterohepatic circulation), and is re-excreted by the liver. A tiny fraction reaches the systemic circulation and is excreted in urine as urobilin (yellow pigment).
3. Bilirubin Fractions (Laboratory Terms)
| Fraction | Chemical Nature | Diazo Reaction | Other Names |
|---|---|---|---|
| Unconjugated bilirubin | Bilirubin-albumin complex | Indirect (slow, needs accelerator) | α-bilirubin |
| Monoconjugated bilirubin | Bilirubin monoglucuronide | Direct (fast) | β-bilirubin |
| Diconjugated bilirubin | Bilirubin diglucuronide | Direct (fast) | γ-bilirubin |
| Delta (δ) bilirubin | Covalently bound to albumin | Direct | δ-bilirubin |
- Tietz Textbook of Laboratory Medicine, 7th Ed.
4. Classification of Jaundice
Jaundice (icterus) is the yellow discoloration of skin, mucous membranes, and sclera caused by bilirubin deposition, secondary to hyperbilirubinemia. It becomes clinically visible when serum bilirubin exceeds ~2-3 mg/dL.
A. Physiologic Classification (by mechanism)
I. Unconjugated (Indirect) Hyperbilirubinemia
1. Increased production of unconjugated bilirubin from heme
- Hemolysis (hereditary: spherocytosis, elliptocytosis, G6PD deficiency, pyruvate kinase deficiency; acquired: immune-mediated ABO/Rh incompatibility)
- Ineffective erythropoiesis
- Rapid RBC turnover in the neonate
2. Decreased delivery to hepatocyte
- Right-sided congestive heart failure
- Portocaval shunting
3. Decreased uptake across the hepatocyte membrane
- Drug competition (e.g., rifampicin)
- Gilbert syndrome (also involves reduced UGT1A1 activity)
- Sepsis, fasting
4. Decreased intracellular storage (reduced Y/Z proteins)
- Competitive inhibition
- Fever
5. Decreased biotransformation (conjugation defect)
- Physiologic jaundice of the newborn (transient UGT1A1 deficiency)
- Drug inhibition
- Hereditary: Crigler-Najjar syndrome
- Type I: complete UGT1A1 deficiency; bilirubin 18-45 mg/dL; unresponsive to phenobarbital; fatal without treatment (phototherapy 12 hrs/day + early liver transplant)
- Type II: partial deficiency (~10% activity); bilirubin 6-25 mg/dL; responds to phenobarbital
- Gilbert syndrome: UGT1A1 activity 10-33% of normal; bilirubin 1.5-4 mg/dL; benign; homozygous A(TA)₇TAA promoter mutation (UGT1A1*28)
- Hepatocellular dysfunction
II. Conjugated (Direct) Hyperbilirubinemia / Cholestasis
1. Decreased secretion of conjugated bilirubin into canaliculi
- Hepatocellular disease, hepatitis
- Intrahepatic cholestasis
- Hereditary: Dubin-Johnson syndrome (MRP2/ABCC2 mutation; autosomal recessive; black liver pigment)
- Rotor syndrome (possibly related to SLCO1B1/SLCO1B3 mutations)
- Drugs (e.g., estradiol, anabolic steroids)
2. Decreased bile drainage
-
Extrahepatic obstruction: gallstones, carcinoma (pancreatic head, cholangiocarcinoma), stricture, biliary atresia, sclerosing cholangitis
-
Intrahepatic obstruction: drugs, granulomas, primary biliary cirrhosis/cholangitis, bile duct paucity, tumors
-
Tietz Textbook of Laboratory Medicine, 7th Ed., Box 51.2
B. Anatomical/Clinical Classification (most commonly used in clinical practice)
| Type | Also Called | Bilirubin Elevated | Mechanism | Classic Features |
|---|---|---|---|---|
| Hemolytic | Pre-hepatic | Unconjugated (indirect) | Excessive RBC destruction overwhelms liver conjugation capacity | Dark urine (urobilinogen), pale stools normal, no bilirubin in urine, anemia, splenomegaly |
| Hepatocellular | Hepatic | Both (mixed) | Liver cell damage → defective uptake, conjugation, and/or secretion | Elevated transaminases, both fractions raised; bilirubin in urine |
| Obstructive | Post-hepatic, cholestatic | Conjugated (direct) | Obstruction of bile flow (intra- or extrahepatic) | Pale/clay stools, dark urine (bilirubinuria), pruritus, elevated ALP/GGT |
| Neonatal | Physiologic/pathologic | Unconjugated (mainly) | Immature UGT1A1 + increased RBC turnover + enterohepatic recirculation | Appears day 2-3, resolves by week 1-2 in term infants |
C. Hereditary Hyperbilirubinemias - Summary Table
| Syndrome | Bilirubin Type | Defect | Serum Bilirubin | Clinical |
|---|---|---|---|---|
| Gilbert | Unconjugated | UGT1A1 ↓ (10-33%) + uptake defect | 1.5-4 mg/dL | Benign, exacerbated by fasting/illness |
| Crigler-Najjar I | Unconjugated | UGT1A1 absent | 18-45 mg/dL | Kernicterus, fatal without treatment |
| Crigler-Najjar II | Unconjugated | UGT1A1 ↓ (≤10%) | 6-25 mg/dL | Responds to phenobarbital |
| Dubin-Johnson | Conjugated | MRP2 (canalicular secretion) defect | Mild elevation | Benign, black liver pigment, impaired BSP excretion |
| Rotor syndrome | Conjugated | SLCO1B1/1B3 (sinusoidal reuptake) | Mild elevation | Benign, no black pigment, no BSP defect |
- Goldman-Cecil Medicine, International Edition
Key Clinical Points
- Normal serum bilirubin: 0.3-1.0 mg/dL total (direct <0.2 mg/dL)
- Jaundice becomes clinically detectable at ~2-3 mg/dL
- Scleral icterus is often the earliest visible sign (sclera has high elastin affinity for bilirubin)
- In hemolytic jaundice: urine is dark (increased urobilinogen), stools are normal, NO bilirubinuria (unconjugated bilirubin is albumin-bound and cannot be filtered)
- In obstructive jaundice: stools are pale/clay (no stercobilin reaches gut), urine is dark (bilirubinuria), and pruritus occurs from bile salt deposition
- Delta (δ) bilirubin: covalently bound to albumin; appears in prolonged cholestasis; cleared slowly (half-life ~18 days - albumin half-life); explains why jaundice persists even after obstruction is relieved
Sources:
- Lippincott's Illustrated Reviews: Biochemistry, 8th ed.
- Henry's Clinical Diagnosis and Management by Laboratory Methods
- Tietz Textbook of Laboratory Medicine, 7th Ed.
- Goldman-Cecil Medicine, International Edition
- Textbook of Family Medicine, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.