I now have comprehensive information from all the key textbooks (Harrison's 22E 2025, Red Book AAP, Dermatology 5e, Fitzpatrick's, Sherris & Ryan's Medical Microbiology, Tintinalli's Emergency Medicine, Jawetz Medical Microbiology) plus the 2024 updated review by Leung et al. Let me now compose the full lecture.
🏫 EXPERT PG PEDIATRICS CLASSROOM LECTURE
ROSEOLA INFANTUM (EXANTHEM SUBITUM / SIXTH DISEASE)
A 120-Minute Evidence-Based Postgraduate Lecture
Professor of Pediatrics | MD/DNB Residents | Tertiary Care Teaching Hospital
"Good morning, everyone. Before we begin, I want to ask you something. You are on night duty. A worried mother walks in at 2 AM with a 10-month-old infant who has had fever of 39.5°C for the past 3 days. Tonight, the fever broke. This morning, the baby is afebrile - and now covered in a rash from trunk to neck. The mother is terrified. What is your single most important clinical diagnosis? Yes - Roseola Infantum. And that is exactly what we are going to master today."
SECTION 1: INTRODUCTION
1.1 Definition
Roseola Infantum is a common, acute, self-limited viral illness of early childhood caused primarily by Human Herpesvirus-6B (HHV-6B), characterized by:
- High fever (38.9-40.6°C) lasting 3-5 days
- Abrupt defervescence followed within hours by
- Rose-pink maculopapular rash on the trunk, spreading centrifugally - appearing AFTER the fever resolves
The entire illness is typically benign and self-limited in immunocompetent children.
[Source: Sherris & Ryan's Medical Microbiology, 8th Ed.; Dermatology 2-Volume Set 5e]
1.2 Historical Background
"Who can tell me - who first described this disease? No? Let me tell you."
| Year | Milestone |
|---|
| 1910 | John Zahorsky first described and distinguished Exanthem Subitum from other childhood rashes. He called it "roseola infantilis." |
| 1941 | Breese confirmed it as a distinct clinical entity. |
| 1988 | Yamanishi et al. used serologic methods to confirm HHV-6 as the causative agent - a landmark discovery. |
| 1992 | HHV-6 classified into two variants: A and B. |
| 2012 | HHV-6A and HHV-6B formally recognized as distinct species (not just variants) - increasing known human herpesviruses to 9. |
[Source: Dermatology 2-Volume Set 5e; Red Book 2021 AAP]
1.3 Synonyms
| Synonym | Meaning |
|---|
| Roseola Infantum | "Rose-colored [disease] of infants" (Latin) |
| Exanthem Subitum | "Sudden rash" (Latin) - describes the abrupt appearance |
| Sixth Disease | The 6th classical childhood exanthem |
| Roseola Infantilis | Early historical term (Zahorsky) |
1.4 Why Is It Called the "Sixth Disease"?
"Residents, I always get asked this in viva. Know it cold."
The classical childhood exanthems were numbered historically:
| Number | Disease | Causative Agent |
|---|
| First disease | Measles (Rubeola) | Measles virus (Paramyxovirus) |
| Second disease | Scarlet Fever | Group A Streptococcus |
| Third disease | Rubella (German measles) | Rubella virus (Togavirus) |
| Fourth disease | Duke's disease (Filatov-Dukes) | Now questioned/obsolete |
| Fifth disease | Erythema Infectiosum (Slapped cheek) | Parvovirus B19 |
| Sixth disease | Roseola Infantum | HHV-6B |
Exam Favorite: This numbering came from the 19th-20th century when clinicians attempted to categorize childhood febrile rashes. Duke's disease (4th disease) is now considered either a form of Scarlet Fever or staphylococcal scalded skin syndrome, and is largely abandoned.
SECTION 2: EPIDEMIOLOGY
2.1 Global Burden
- HHV-6 infection is essentially universal worldwide - no geographic exceptions.
- Seroprevalence reaches 80-95% by 2-3 years of age in all populations studied.
- In emergency clinics, HHV-6 accounts for 10-45% of all febrile illnesses in infants 6-12 months of age.
- About 20% of all ED visits for febrile children 6-12 months of age are attributable to HHV-6.
[Source: Medscape/Emedicine citing population-based data; Red Book AAP 2021]
2.2 Incidence
- Only ~30% of children with primary HHV-6 infection develop the classic rash of roseola (exanthem subitum).
- The remaining 70% have undifferentiated febrile illness without rash or are subclinical.
- This is a key point - HHV-6 causes FAR more febrile illness than "roseola" alone.
2.3 Age Distribution
"If a 4-year-old presents with this picture, think twice. This disease has a narrow age window."
- Peak incidence: 6-21 months (some sources say 6-12 months as the single peak)
- 95% of cases occur between 6 months and 3 years
- Rare before 3 months (protected by maternal antibody)
- Rare after 4 years (most children already infected)
- Peak HHV-6 seroprevalence of 90-100% by 3-4 years
- Boys and girls equally affected (no sex predilection)
[Source: Dermatology 2-Volume Set 5e; Leung et al., Curr Pediatr Rev 2024]
2.4 Maternal Antibody Dynamics - Pathognomonic Concept
"This is beautiful immunology. Let me draw this on the board."
Birth ——→ 3 months: High maternal IgG (protective)
3-6 months: Maternal IgG waning
6-12 months: NADIR of maternal IgG → PEAK susceptibility to HHV-6
12-24 months: Most children seroconvert
3-4 years: 90-100% seropositive
Maternal IgG is present in 70-97% of fetuses at birth. As it wanes by 6 months, primary infections surge. This perfectly explains the age distribution.
2.5 Seasonal Variation
- Infections occur throughout the year without strict seasonality (Red Book AAP).
- Spring has the highest incidence in some studies (Fitzpatrick's dermatology).
- Summer and fall epidemics have also been reported.
- HHV-7 infections tend to occur slightly later in childhood than HHV-6.
2.6 Risk Factors
- Waning maternal antibody (6-12 months)
- Daycare attendance (close contact with infected children/adults)
- Immunocompromised state (for severe disease/reactivation)
- Hematopoietic stem cell transplantation (HSCT) - reactivation in ~50% of recipients
- Cord blood transplant recipients - highest risk for limbic encephalitis
2.7 Transmission Dynamics
- Primary route: Respiratory secretions / saliva
- The salivary glands are an important site of viral replication and persistence
- Adults chronically shed HHV-6 in saliva - asymptomatically - and serve as the source of infection for infants (usually parents or older siblings)
- Older siblings are a particularly common source of transmission
- HHV-6 DNA also detected in cervix (potential perinatal route)
- NOT transmitted in breast milk
- In transplant settings: donor organ can transmit HHV-6 (rare)
2.8 Infectious Period
- HHV-6 is shed continuously in saliva by seropositive adults - no defined infectious period for the asymptomatic carrier
- During acute primary infection, viremia lasts 3-4 days
- Secondary cases are rarely identified - suggesting community exposure is the norm, not household transmission clusters
SECTION 3: ETIOLOGY AND VIROLOGY
3.1 Classification
Human Herpesvirus 6 (HHV-6):
- Family: Herpesviridae
- Subfamily: Betaherpesvirinae (most closely related to CMV)
- Genus: Roseolovirus (also includes HHV-7)
- Two formally distinct species: HHV-6A and HHV-6B (classified as separate species since 2012)
Human Herpesvirus 7 (HHV-7):
- Also a Roseolovirus, Betaherpesvirus
- ~50% DNA homology with HHV-6
- Isolated in 1990 from T lymphocytes of a healthy adult
3.2 HHV-6A vs HHV-6B - Important Differences
| Feature | HHV-6A | HHV-6B |
|---|
| Association with Roseola | NOT clearly associated | MAJOR cause of roseola infantum |
| Pathogenic role | Unclear; possibly neurotropic | Well-established childhood pathogen |
| Reactivation disease | Both can reactivate | Predominant in post-transplant disease |
| Associations | Possibly Hashimoto disease; MS (research ongoing) | Febrile seizures, encephalitis, DRESS |
| Chromosomal integration | Both can integrate (ciHHV-6) | Both can integrate (ciHHV-6) |
| Geographic distribution | More common in Africa | Worldwide |
3.3 HHV-6 Virology
Structure:
- Double-stranded DNA virus
- Genome: 160-170 kbp (kilobase pairs), G+C content 43-44%
- Genome organization resembles CMV
- Lipid envelope (making it susceptible to common disinfectants)
- Icosahedral capsid, tegument layer, envelope with glycoproteins
Cellular Receptor:
- CD46 (complement regulatory protein) - the primary cellular receptor for HHV-6
- This explains its tropism for CD4+ T lymphocytes (which express CD46)
- Also infects: CD8+ T cells, B cells, monocytes/macrophages, NK cells, astrocytes, microglia, oligodendrocytes, neurons
Antigenic Relationships:
- HHV-6 is largely unrelated antigenically to other human herpesviruses
- Limited cross-reactivity exists between HHV-6 and HHV-7
3.4 Viral Replication
- Attachment via glycoprotein H/L complex to CD46 receptor
- Fusion with host cell membrane
- Transport of capsid to nucleus
- Lytic infection in activated CD4+ T lymphocytes: rapid replication, cytopathic effect
- DNA replication using viral DNA polymerase
- Virion assembly, tegument acquisition, envelopment
- Release by exocytosis or cell lysis
3.5 Latency and Reactivation - A Critical Concept
"This is where HHV-6 gets really interesting - and clinically dangerous."
Latency:
- After primary infection, HHV-6 establishes lifelong latency in:
- CD4+ T lymphocytes (peripheral blood mononuclear cells)
- Central nervous system
- Salivary glands
- Female genital tract
- Lung
Chromosomal Integration (ciHHV-6) - Unique Feature:
- HHV-6 can integrate its entire genome into telomeres of host chromosomes
- When this occurs in germline cells, offspring carry a copy in every nucleated cell
- ~1% of the general population has ciHHV-6 (inherited chromosomally integrated HHV-6)
- These individuals will always test PCR-positive for HHV-6 - a critical diagnostic pitfall!
- Pregnant women with ciHHV-6 may have higher risk of pre-eclampsia or spontaneous abortion (Harrison's 22E, 2025)
Reactivation Triggers:
- Immunosuppression (transplantation, HIV, corticosteroids)
- Fever from other infections
- Pregnancy
Clinical Reactivation States:
- Immunocompetent: Usually asymptomatic
- Post-HSCT: Occurs in ~50% of patients, peaks 2-4 weeks post-transplant; can cause limbic encephalitis, delayed engraftment, increased mortality
- Solid organ transplant: Fever, rash, hepatitis, graft rejection
SECTION 4: PATHOGENESIS - STEP BY STEP
"Now we come to the most important part. If you understand pathogenesis, you understand every clinical feature. Follow me through this carefully."
Step 1: Viral Entry
- Route: Upper respiratory tract (infected saliva from an asymptomatic adult/older sibling)
- Virus binds to CD46 receptor on epithelial cells of oropharynx
- Initial replication occurs in oropharyngeal epithelium and regional lymph nodes (cervical, occipital)
- Clinical correlate: Mild pharyngitis, cervical/occipital lymphadenopathy seen early
Step 2: Initial Viremia (Primary Viremia)
- Virus spreads via lymphatics to blood
- Infects activated CD4+ T lymphocytes (its primary tropism)
- Also infects monocytes, macrophages, dendritic cells
Step 3: Secondary Viremia - Dissemination
- Viremia in immunocompetent children lasts 3-4 days
- Virus reaches: liver, spleen, salivary glands, CNS, skin
- Clinical correlate: Fever, hepatomegaly (mild), irritability
Step 4: The Fever Mechanism
- HHV-6 infects monocytes/macrophages and triggers release of:
- IL-1β, TNF-α, IL-6 (major pyrogenic cytokines)
- These act on the hypothalamic thermoregulatory center via prostaglandin E2 (PGE2)
- Fever is HIGH (39.5-40.6°C) because the cytokine response to primary HHV-6 is intense
- Fever is classically remittent (persists 3-5 days, peaks in early evenings)
"Ask yourself - why does the fever break so suddenly on day 3-5? Because the immune response - specifically CD8+ cytotoxic T cells and NK cells - clears the viremia. The moment viremia ends, the cytokine storm resolves, and temperature normalizes."
Step 5: The Immune Response
- Innate immunity: NK cells, type I interferons (IFN-α/β) provide early defense
- Adaptive immunity: CD8+ cytotoxic T cells - the primary clearance mechanism
- Antibody response: IgM appears within 5-7 days of infection; IgG follows
- As immune response matures → viremia clears → fever resolves → rash appears
Step 6: Why Does Rash Appear AFTER Defervescence? - The Key Pathogenic Question
"This is THE most important question in roseola pathogenesis. I guarantee this comes in your viva."
Mechanism of the rash:
- The rash is an immune-mediated phenomenon - NOT direct viral cytopathic effect on skin
- When the adaptive immune response (CD8+ T cells) clears viremia, immune complexes and cytotoxic T-cell activity in dermal vessels cause a vasodilatory inflammatory response
- This produces the characteristic rose-pink maculopapules (similar to the mechanism in rubella)
- Since the rash requires mounting of adaptive immunity → it appears AFTER the fever (viremic phase) resolves
- This is analogous to other post-infectious exanthems
Simplified teaching mnemonic: "Virus first, immune rash second"
Step 7: Mechanism of Febrile Seizures
- HHV-6 is the single most common cause of febrile seizures in infancy (10-20% of all febrile seizures in infants are HHV-6-related)
- Mechanism is multifactorial:
- Rapid rise in temperature (rate of temperature change more important than absolute value)
- Direct neurotropism: HHV-6 infects astrocytes, microglia, neurons → direct CNS excitability
- Cytokine-mediated neuronal excitability: IL-6 lowers seizure threshold
- Transient neuronal hyperexcitability due to CNS inflammation
- This is why ~10-15% of roseola cases are complicated by febrile seizures (Red Book AAP)
Step 8: Why Children Recover Rapidly
- HHV-6 infection in immunocompetent children is self-limited because:
- Rapid and effective innate immune response (interferon, NK cells)
- Brisk CD8+ T-cell response clears viremia efficiently
- Antibody seroconversion provides durable protection against reinfection
- The virus retreats into latency after primary viremia is cleared
SECTION 5: CLINICAL FEATURES
The Classic Biphasic Course
Day 0-1: Abrupt onset high fever (39.5-40.6°C)
Days 1-3: Persistent high fever; child may be surprisingly well-appearing
Associated: irritability, rhinorrhea, mild diarrhea
Day 3-5: ABRUPT DEFERVESCENCE (fever breaks suddenly)
Hours later: RASH APPEARS (erythematous maculopapular, trunk-first)
Days 5-7: Rash fades; child completely recovered
"Remember: 'Rose after the fever goes.' That is roseola."
5.1 The Fever
- Temperature: 38.9-40.6°C (102-105°F) - often alarmingly high
- Pattern: Remittent; tends to peak in early evenings
- Duration: 3-5 days (some sources say 3-7 days)
- Quality: Child often looks surprisingly well despite high fever - "happy, active, playful, alert" (Leung et al., 2024)
- Important: The fever is the stage of viremia; child is most contagious during this phase
5.2 The Rash
This is the pathognomonic feature.
| Feature | Description |
|---|
| Morphology | Discrete, rose-pink/rose-red macules and papules |
| Size | 2-5 mm in diameter |
| Special feature | Often surrounded by a white halo (pathognomonic) |
| Blanching | YES - blanches with pressure |
| Distribution | Trunk first → neck → proximal extremities; face occasionally |
| Duration | 24-48 hours (some say 1-5 days) |
| Progression | Does NOT spread progressively like measles (cephalocaudal) |
| Resolution | Fades without desquamation, without hyperpigmentation |
| Pruritus | None (non-pruritic) |
| Timing | Appears 1 day before to 1-2 days AFTER fever resolves |
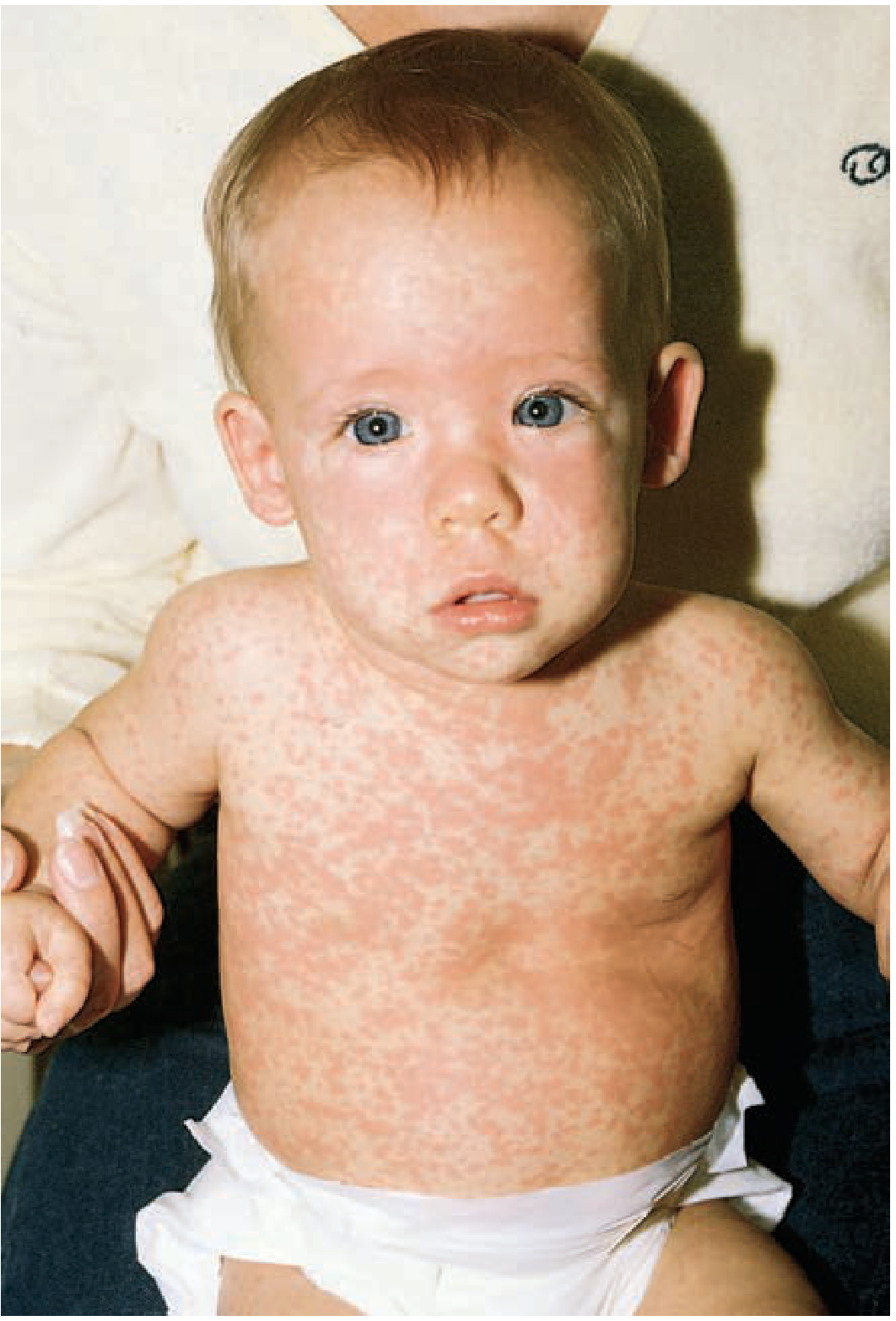
The White Halo Sign: Discrete rose-red macules/papules surrounded by a pale white halo - this is characteristic and distinguishes roseola from rubella and other exanthems.
Typical roseola infantum rash - discrete rose-pink maculopapular eruption on trunk and face appearing after fever breaks (Tintinalli's Emergency Medicine)
5.3 Associated Symptoms - Mechanism for Each
1. Irritability
- Caused by high-grade fever + direct CNS involvement (neurotropism of HHV-6)
- Children may be difficult to soothe during the febrile phase
- EXAM POINT: Despite high fever, children are often "alert and active" - this reassures against serious bacterial infection
2. Mild Diarrhea
- HHV-6 infects intestinal epithelium → mild mucosal inflammation
- Self-limited, watery, non-bloody
- Occurs in ~68% of primary HHV-6 infections (Asano et al., 1994)
3. Rhinorrhea / Coryza
- Mild upper respiratory tract inflammation
- Reflects viral replication in oropharyngeal mucosa
4. Conjunctivitis / Palpebral Edema
- Mild injection of conjunctivae
- Palpebral (eyelid) edema - gives a "sleepy appearance" - characteristic sign in roseola (Fitzpatrick's)
5. Mild Pharyngitis / Tonsillar inflammation
- Site of initial viral entry and replication
6. Inflamed (injected) Tympanic Membranes
- Cited in the Red Book AAP - a common but underappreciated finding
- TRAP: Can mislead residents into diagnosing otitis media and prescribing antibiotics unnecessarily!
5.4 NAGAYAMA SPOTS - High-Yield Sign
"How many of you know Nagayama spots? Let me teach you. This is frequently asked in viva and PG exams."
- Erythematous red papules on the soft palate and uvula
- Also: Ulcers at the uvula and palatoglossal junction (pathognomonic finding, per Dermatology 2-Volume Set 5e)
- Described by Dr. Nagayama in Japan
- Present in many but not all cases
- They may PRECEDE the skin exanthem - thus can serve as an early diagnostic clue before the rash appears
- Distinct from Koplik spots of measles (which are bluish-white on a red base on buccal mucosa)
| Nagayama Spots (Roseola) | Koplik Spots (Measles) |
|---|
| Location | Soft palate, uvula, palatoglossal junction | Buccal mucosa opposite to lower molars |
| Morphology | Red/erythematous papules | Bluish-white granules on red base |
| Timing | During fever (may precede rash) | BEFORE measles rash (prodromal) |
| Association | HHV-6/HHV-7 | Measles virus |
5.5 Bulging Anterior Fontanelle
- Seen in some infants with roseola
- Mechanism: Mild aseptic meningeal irritation and increased intracranial pressure from cytokine-mediated CNS inflammation
- NOT always indicative of bacterial meningitis - context matters!
- In the presence of roseola, a bulging fontanelle usually resolves spontaneously
- Clinical pearl: Always perform LP to rule out bacterial meningitis if fontanelle is tense and child is toxic - do NOT assume roseola without ruling out serious bacterial infection
5.6 Cervical and Occipital Lymphadenopathy
- Common finding during febrile phase
- Occipital lymphadenopathy is particularly associated with roseola (also with rubella)
- Post-occipital lymphadenopathy was described as a diagnostic sign by McEnery (1970)
- Reflects initial replication in cervical lymph nodes
5.7 Febrile Seizures
- Occur in 10-15% of children with primary HHV-6 infection (Red Book AAP; Dermatology 5e)
- HHV-6 accounts for 10-20% of all febrile seizures during infancy (Harrison's 22E, 2025)
- Usually occur during the febrile phase (not after rash appears)
- Most are simple febrile seizures: generalized, <15 minutes, single episode
- Complex febrile seizures (prolonged, focal, or multiple within 24 hours) can occur
- Seizures can precede the rash - making diagnosis retrospective
SECTION 6: PHYSICAL EXAMINATION
"Let me walk you through how I examine a child I suspect has roseola. This is bedside teaching."
6.1 General Inspection (From the Door)
- Overall appearance: Alert, active, playful (despite fever) OR irritable
- Hydration status: Assess capillary refill, skin turgor, mucous membranes, fontanelle
- Note: A "happy" febrile infant - think roseola
6.2 Vital Signs
- Temperature: Rectal temperature preferred for accuracy in infants <3 months (axillary acceptable for older infants)
- Heart rate: Tachycardia proportional to fever
- Respiratory rate: Count for a full minute
- Blood pressure: Check if appears toxic
6.3 Skin Examination
Febrile phase: Skin is hot, flushed; no rash
Post-febrile phase:
- Inspect trunk first (undress the child completely)
- Note: Rose-pink discrete macules/papules, 2-5mm, with white halo
- Check neck, proximal extremities, face
- Blanching test: Press with a glass slide (diascopy) - if it blanches → vasodilatory/inflammatory rash; if non-blanching → purpuric → ALARM SIGN (think meningococcemia, HSP)
- Note absence of desquamation, absence of vesicles, absence of petechiae/purpura
6.4 Lymph Node Examination
- Palpate cervical (anterior + posterior), occipital, submandibular chains
- Occipital + posterior cervical nodes enlarged → supports roseola/rubella
- Note: size, tenderness, consistency, overlying skin changes
6.5 Oral Cavity (VERY IMPORTANT)
- Look for: Nagayama spots on soft palate, uvula
- Koplik spots? → Think measles
- Strawberry tongue? → Think scarlet fever, Kawasaki
- Oral ulcers at palatoglossal junction → supports roseola
- Check pharynx for erythema, exudate
6.6 Neurological Examination
- Assess fontanelle: flat/bulging/tense
- Neck stiffness: Kernig's + Brudzinski's (if meningeal signs present → LP)
- Level of consciousness: AVPU scale or GCS
- Look for focal deficits
- Post-ictal state if seizure occurred
6.7 Ear Examination
- Otoscopy: Injected tympanic membranes (common in roseola - do NOT automatically prescribe antibiotics)
- Assess for signs of true AOM: loss of light reflex, bulging, effusion
6.8 Abdominal Examination
- Palpate for hepatomegaly (mild; present in ~10% with acute HHV-6 infection)
- Splenomegaly: Uncommon in uncomplicated roseola
6.9 Red Flag Findings (Admit/Urgent Workup)
| Red Flag | Action |
|---|
| Petechial/purpuric rash | Rule out meningococcemia - EMERGENCY |
| Bulging tense fontanelle + toxic-looking child | LP to rule out bacterial meningitis |
| Febrile seizure | Assess: simple vs complex; admission criteria |
| Altered consciousness, encephalopathy | ICU evaluation, neuroimaging, LP |
| Immunocompromised child | Admit, antiviral consideration |
| Neonates (<3 months) with fever | Full sepsis workup regardless |
| Prolonged fever (>7 days) | Reconsider diagnosis |
SECTION 7: CLASSICAL CLINICAL SCENARIO
"Let me present a case. This is exactly how you will be tested in an OSCE or final examination."
Case Presentation
History:
"A 10-month-old male child was brought to the pediatric OPD by his mother with complaints of high-grade fever for 4 days and rash all over the body since this morning. Fever was sudden in onset, high-grade (measured at 40°C at home), remittent, not associated with chills or rigors. Child was irritable but active and feeding well. Mother noted mild loose stools (2-3 per day, watery, no blood/mucus) and mild coryza. No seizures. No similar episodes in the past. No antibiotic use. Immunization up to date (BCG, OPV, Pentavalent, IPV). On examination this morning, the fever has broken. Child is afebrile (37.0°C), alert, active, smiling. There is a widespread rash on the trunk and neck."
"What are you thinking? Roseola! Now let me take you through the examination."
Physical Examination:
- Vitals: Afebrile, HR 110/min, RR 30/min, SpO2 99%
- Skin: Discrete rose-pink maculopapules, 2-4mm, blanching on pressure, with white halos; present on trunk, neck, proximal extremities; face mildly involved. No petechiae. No desquamation.
- Lymph nodes: Bilateral posterior cervical and occipital lymph nodes palpable (0.5-1cm), soft, non-tender
- Oral: Erythematous papules on soft palate (Nagayama spots)
- ENT: Mild pharyngeal congestion; tympanic membranes mildly injected bilaterally
- Fontanelle: Flat (normal)
- Neurological: No neck stiffness; Kernig's/Brudzinski's negative; normal tone, reflexes
- Abdomen: Soft; liver just palpable (1cm below right costal margin, normal for age)
"This is a textbook case. What is your diagnosis? Exanthem Subitum / Roseola Infantum. No investigations needed. Management: Parental reassurance, symptomatic treatment."
Investigation Plan: NONE required. This is a clinical diagnosis.
Parental Counselling:
- "Your child has a viral illness called Roseola. The fever has broken. The rash appeared because the body's immune system is now fighting the virus successfully - this is actually a GOOD sign."
- "The rash will disappear on its own in 1-2 days without any treatment."
- "Continue oral feeds; paracetamol if uncomfortable; return if seizure occurs, rash becomes dark/non-blanching, child becomes very lethargic, or fever returns."
SECTION 8: DIFFERENTIAL DIAGNOSIS
"This section will be crucial for your clinical practice and examination. Let me build a comparison table for you."
8.1 Comprehensive Differential Diagnosis Table
| Feature | Roseola | Measles | Rubella | Scarlet Fever |
|---|
| Age | 6-24 months | Any (unvaccinated) | Any | 2-10 years |
| Causative agent | HHV-6B | Measles virus | Rubella virus | Group A Strep |
| Fever pattern | High, 3-5 days, then BREAKS | High, prodromal (3-4d) | Low-moderate | High, persists with rash |
| Rash timing | AFTER fever resolves | During fever (day 3-4) | With or just after fever | Concurrent with fever |
| Rash type | Rose-pink macules/papules, white halo | Red-brown confluent maculopapules | Pink, discrete macules | Fine papules (sandpaper feel), confluent |
| Rash distribution | Trunk → neck → extremities | Face (hairline) → downward cephalocaudal | Face → trunk → extremities | Neck → trunk, spares face (palms/soles in KD) |
| Koplik spots | Absent | Present (pathognomonic) | Absent | Absent |
| Nagayama spots | Present | Absent | Absent | Absent |
| Strawberry tongue | Absent | Absent | Absent | Present |
| Lymphadenopathy | Occipital/cervical | Present (generalized) | Suboccipital, postauricular | Absent |
| Cough, coryza, conjunctivitis (3 C's) | Mild/absent | Prominent (all 3) | Mild | Absent |
| Desquamation | None | Minimal (fine) | None | Marked perioral/fingertips |
| CBC | Leukopenia, relative lymphocytosis | Leukopenia | Normal/mild lymphocytosis | Leukocytosis, neutrophilia |
| Serious complications | Febrile seizures | Pneumonia, SSPE, encephalitis | Congenital rubella syndrome | Rheumatic fever, GN |
| Feature | Dengue | Enteroviral exanthem | Drug eruption | Kawasaki disease |
|---|
| Age | Any (school age common) | Any infant/child | Any | <5 years (peak 1-2y) |
| Fever pattern | Biphasic ("saddleback") | Variable | Follows drug exposure | Persistent >5 days |
| Rash timing | Day 3-5; after initial fever | Variable | After drug exposure | During fever |
| Rash type | "Sea of red with isles of white" petechiae | Variable (maculopapular, vesicular, hand-foot-mouth) | Morbilliform, urticarial, fixed | Polymorphous |
| Rash distribution | Generalized; spares palms/soles (often) | Variable; HFMD - palms/soles | Generalized | Trunk, perineum (groin desquamation) |
| Lymphadenopathy | Present (hepatosplenomegaly) | Absent/mild | Absent | Unilateral cervical >1.5cm (one of 5 criteria) |
| Oral findings | Absent | Oral ulcers (enteroviral) | Mucositis (SJS) | Strawberry tongue, red cracked lips |
| CBC | Leukopenia, thrombocytopenia, raised hematocrit | Normal/mild lymphocytosis | Eosinophilia (drug) | Leukocytosis, raised CRP/ESR, elevated platelets (late) |
| Key labs | NS1 antigen, IgM/IgG dengue | Nasopharyngeal/stool culture | Clinical history | Echo (coronary aneurysm), ECHO |
| Serious complications | DHF, DSS, hemorrhage | Neonatal sepsis (enteroviral), myocarditis | SJS/TEN | Coronary artery aneurysm |
| Feature | MIS-C | Parvovirus B19 | Adenovirus |
|---|
| Age | School age, adolescent | 4-12 years | Any age |
| Trigger | 2-6 weeks post COVID-19 | None | None |
| Fever pattern | High, persistent (>3 days) | Low-grade after slapped cheek | High, persistent |
| Rash | Polymorphous | Slapped cheek → lacy reticular trunk rash | Morbilliform (less common) |
| Distribution | Variable, trunk predominant | Face first, then trunk/extremities (lacy) | Variable |
| Oral findings | Strawberry tongue, red lips | Absent | Pharyngoconjunctival fever |
| Lymphadenopathy | Absent/mild | Absent | Bilateral cervical LAP |
| CBC | Elevated CRP/ESR/ferritin, lymphopenia | Normal/mild anemia (aplastic crisis in SCA) | Leukocytosis or normal |
| Serious complications | Cardiac shock, multisystem inflammation | Aplastic crisis in hemolytic anemias, hydrops fetalis | Pneumonia, hepatitis |
8.2 Memory Aid for Rash Timing
BEFORE fever / during prodrome: Koplik spots (measles)
DURING fever with rash: Measles, Scarlet fever, Dengue, Drug rash, Kawasaki
AFTER fever resolves: ROSEOLA (Exanthem Subitum) ← UNIQUE
SECTION 9: DIAGNOSIS
9.1 Clinical Diagnosis - The Gold Standard
"In the vast majority of cases - roseola is a CLINICAL diagnosis. No tests needed."
Diagnostic criteria (clinical):
- Age 6 months - 3 years
- High fever (≥38.5°C) for 3-5 days
- Abrupt defervescence
- Rose-pink maculopapular rash appearing AFTER fever resolves
- Otherwise well-appearing child
- Nagayama spots (if present, strongly supportive)
- Occipital/cervical lymphadenopathy
9.2 When Investigations ARE Unnecessary
- Typical presentation with above criteria
- Immunocompetent child
- No complications
- Rash has appeared (confirming diagnosis retrospectively)
9.3 CBC Findings
| Finding | Significance |
|---|
| Leukopenia (WBC <4,000/mm³) | Classic finding in roseola; suggests viral etiology |
| Relative lymphocytosis (>50-60%) | Typical of viral infections |
| Atypical lymphocytes | May be seen |
| Neutropenia | Can be marked; raises concern for secondary bacterial infection if severe |
| Normal platelet count | Differentiates from dengue |
Exam pearl: CBC showing leukopenia in a febrile infant 6-24 months → think HHV-6 / roseola
9.4 Other Lab Parameters
| Test | Result in Roseola | Clinical Significance |
|---|
| CRP | Normal to mildly elevated | High CRP (>20-40) → think bacterial |
| ESR | Normal to mildly elevated | Non-specific |
| Serum transaminases (AST/ALT) | Mildly elevated (10% of cases) | Subclinical hepatitis |
| LFT | Usually normal | Raised in severe/immunocompromised |
| Procalcitonin | Low/normal | Normal PCT + leukopenia → strongly viral |
| CSF (if LP done) | Normal or mild pleocytosis | In roseola encephalitis: lymphocytic pleocytosis, normal glucose/protein usually |
| Urinalysis | Normal | Useful to rule out UTI as cause of fever |
9.5 Specific Laboratory Diagnosis (When Needed)
Indications for specific testing:
- Immunocompromised patients (transplant, HIV, malignancy)
- Severe/atypical presentation
- Encephalitis workup
- Epidemiological purposes
- ciHHV-6 detection
1. PCR (Polymerase Chain Reaction) - Best Method
- Quantitative real-time PCR is the test of choice for active infection
- Detects HHV-6 DNA in:
- Peripheral blood (PBMC) - most common
- CSF (for encephalitis evaluation)
- Tissue biopsies
- Qualitative PCR CANNOT distinguish: latent vs active infection
- Quantitative PCR: HIGH viral load = active/replicating infection; low/undetectable = latent
- ciHHV-6 pitfall: Very high viral load (~10⁶ copies/whole blood) in all samples → suspect ciHHV-6
2. Serology
- IgM: Appears within 5-7 days; BUT IgM is NOT reliable - may not be detectable in all primary infections, and can be positive in asymptomatic adults (due to reactivation)
- IgG: Fourfold rise from acute to convalescent (2-4 weeks apart) = evidence of recent primary infection
- IgG avidity testing: Low-avidity IgG → recent primary infection; useful to distinguish from reactivation
- Cross-reactivity between HHV-6 and HHV-7 serology
3. Viral Culture
- Possible in CD4+ T lymphocytes or saliva
- Low sensitivity, long turnaround (3-4 weeks), expensive
- Rarely used clinically (Red Book AAP)
4. Multiplex PCR Panels (e.g., FilmArray Meningitis/Encephalitis Panel)
- FDA-cleared panels include HHV-6 as a target for CSF
- Important caveat: A positive HHV-6 result may represent ciHHV-6 in the 1% of population with chromosomal integration - must interpret with clinical context and high viral loads
9.6 Summary Table: When to Test
| Scenario | Investigation Needed? |
|---|
| Typical roseola in immunocompetent infant | No |
| Roseola + febrile seizure, post-ictal resolved | Usually no; LP only if <18 months, first seizure, unclear diagnosis |
| Roseola + encephalopathy/altered sensorium | Yes: LP (CSF PCR for HHV-6), MRI brain, EEG |
| Immunocompromised + HHV-6 reactivation | Yes: Quantitative blood PCR, organ-specific workup |
| Post-HSCT fever (2-4 weeks post-transplant) | Yes: Blood HHV-6 PCR monitoring |
| Unexplained fever in infant without obvious diagnosis | Consider HHV-6 PCR |
SECTION 10: MANAGEMENT
"Management of roseola is largely about what NOT to do - don't over-investigate, don't over-treat, and don't under-counsel the parents."
10.1 Outpatient Management (Majority of Cases)
1. Fever Management
- Paracetamol (Acetaminophen): 10-15 mg/kg/dose every 4-6 hours (max 5 doses/24h) - FIRST LINE
- Ibuprofen: 5-10 mg/kg/dose every 6-8 hours - Alternative (avoid <6 months, avoid in dengue possibility)
- Luke-warm sponging: Adjunct; tepid water (not cold, not ice)
- Do NOT use aspirin (Reye's syndrome risk)
- Do NOT use aspirin in any viral illness in children
2. Hydration
- Encourage oral fluids: ORS, breast milk, formula, water
- Continue feeds; anorexia is temporary
- If vomiting/poor intake → IV fluids if hospitalized
3. Isolation
- No specific isolation required for typical roseola in immunocompetent children
- Child can return to daycare once fever-free for 24 hours
- No exclusion required once asymptomatic (virus continues to be shed in saliva for life, so isolation beyond fever is impractical)
4. No Antiviral Therapy
- No antiviral is indicated for uncomplicated roseola in immunocompetent children (StatPearls, Red Book AAP)
- No vaccine currently available
10.2 Parent Counselling - Key Points
"This is an OSCE station. You will be scored on communication."
- Explain the diagnosis: "Your child has a viral illness called Roseola. It is very common in infants this age."
- Explain the rash: "The rash appearing AFTER the fever is NOT an allergic reaction. It is actually a sign that your baby's immune system has successfully fought the virus. It will go away on its own in 1-2 days."
- Prognosis: "This is a self-limiting illness. Your child will recover completely."
- Return to clinic if:
- Seizure occurs
- Rash becomes dark/non-blanching (red alarm: meningococcemia)
- Child becomes very lethargic, difficult to arouse
- Fever returns after resolution
- Child is not tolerating fluids
- Rash does not fade within 5 days
- Fever management at home: Explain antipyretic dosing and schedule
- Daycare: Can return when fever-free for 24 hours
- Siblings: Explain that other young children in the home may develop similar illness
10.3 Hospital Admission Criteria
| Indication for Admission | Rationale |
|---|
| Complex febrile seizure | Prolonged (>15 min), focal, or multiple |
| First febrile seizure in infant <12 months | Close monitoring, rule out meningitis |
| Encephalopathy, altered sensorium | Neuro-ICU evaluation |
| Immunocompromised child | Risk of severe HHV-6 disease |
| Dehydration with poor oral intake | IV fluids |
| Toxic-appearing child (high suspicion of bacterial co-infection) | Sepsis workup |
| Uncertain diagnosis (non-blanching rash, etc.) | Rule out serious infections |
SECTION 11: FEBRILE SEIZURES IN ROSEOLA
"This is a standalone chapter in any pediatrics textbook, but let me contextualize it for roseola."
11.1 Epidemiology
- HHV-6 is responsible for 10-20% of all febrile seizures in infants (Harrison's 22E, 2025)
- Febrile seizures occur in 10-15% of children with roseola (Red Book AAP; Leung et al. 2024)
- Age: predominantly 6-18 months (peak risk)
- Risk with genetic mutations: RandBP2, POLG, CPT2 mutations predispose to severe neurological disease with HHV-6 (Red Book AAP)
11.2 Classification
| Type | Features |
|---|
| Simple febrile seizure | Generalized, duration <15 minutes, single episode within 24 hours, no focal features, full recovery |
| Complex febrile seizure | Focal OR duration >15 minutes OR >1 episode in 24 hours OR postictal focal deficits (Todd's palsy) |
"In roseola, most seizures are SIMPLE. If you see a complex febrile seizure - always consider HHV-6 encephalitis or a genetic predisposition."
11.3 Initial Management of Febrile Seizure
Acute Management Algorithm:
Step 1: ABC - Position (recovery position), O2, venous access
Step 2: Assess duration (time the seizure from onset)
Step 3: If seizure >5 minutes → TREAT (don't wait for 15 minutes)
Step 4: First-line drug → IV/IM/buccal/rectal Benzodiazepine
→ IV Diazepam: 0.3 mg/kg IV (max 10mg)
→ Buccal/intranasal Midazolam: 0.2-0.3 mg/kg (preferred if no IV access)
→ Rectal Diazepam: 0.5 mg/kg
Step 5: If no response in 5-10 min → REPEAT benzodiazepine
Step 6: If refractory (status epilepticus) → IV Phenobarbitone 20 mg/kg
or IV Phenytoin 20 mg/kg (or Fosphenytoin 20 PE/kg)
Step 7: Treat underlying fever with antipyretics
Step 8: Identify cause - roseola context → reassure if typical
11.4 When to Do Lumbar Puncture (LP)
| Indication for LP | AAP Recommendation |
|---|
| Meningeal signs: Neck stiffness, Kernig's, Brudzinski's | Yes - mandatory |
| Infant <12-18 months (signs of meningitis may be subtle) | Strong consideration |
| Complex febrile seizure | Consider if no clear viral diagnosis |
| Post-ictal state prolonged (>30 min) | Consider |
| Second visit for fever without apparent source in same illness | Consider (AAP 2011 guideline) |
| Already received antibiotics (may mask meningitis) | Yes |
| Immunocompromised child | Yes |
11.5 Neuroimaging - When Is It Required?
- NOT required for simple febrile seizure
- MRI brain indicated when:
- Focal neurological signs
- Prolonged postictal state (>30-60 min)
- Focal seizure
- Encephalopathy persisting after seizure
- Suspicion of HHV-6 encephalitis (especially in immunocompromised - look for mesial temporal signal changes on MRI)
11.6 EEG Indications
- NOT required after simple febrile seizure
- Indicated if:
- Concern for epileptic disorder (afebrile seizures, atypical febrile seizures)
- Complex febrile seizure
- Encephalitis evaluation
11.7 Prophylaxis After Febrile Seizure
- NOT recommended for simple febrile seizures (AAP Position Statement)
- Parents should be counselled on home management (rectal/buccal diazepam for prolonged seizures)
- Continuous antiepileptic drugs NOT routinely recommended
SECTION 12: COMPLICATIONS
12.1 In Immunocompetent Children
| Complication | Frequency | Details |
|---|
| Febrile seizures | 10-15% | Most common complication; usually benign simple febrile seizure |
| Hepatitis | ~10% (subclinical) | Mild elevated transaminases; rarely symptomatic; self-limited |
| Encephalitis | Rare | Altered sensorium, seizures, focal deficits; HHV-6 DNA in CSF |
| Meningitis | Very rare | Lymphocytic pleocytosis; benign course |
| Bulging fontanelle | Occasional | Usually mild increase in ICP; resolves spontaneously |
| Thrombocytopenic purpura | Rare | Self-limited |
| Mononucleosis syndrome | Rare | ~5% of all mononucleosis cases attributed to HHV-6 |
| Pneumonitis | Very rare | Interstitial pattern; self-limited |
| Hemophagocytic syndrome (HLH) | Very rare | Fever, cytopenias, splenomegaly, elevated ferritin, hemophagocytosis on BM biopsy |
| Myocarditis | Very rare case reports | |
12.2 In Immunocompromised Patients - Severe Disease
"This is where roseola stops being benign. HHV-6 in transplant patients is life-threatening."
Post-HSCT Complications (Reactivation in ~50% of HSCT recipients):
| Complication | Details |
|---|
| Post-transplant acute limbic encephalitis (PALE) | Best characterized HHV-6B reactivation syndrome; characterized by anterograde amnesia, seizures, insomnia, confusion, SIADH; MRI shows mesial temporal signal; worst with cord blood transplant |
| Delayed engraftment | HHV-6 suppresses hematopoiesis |
| Pneumonitis | Interstitial pneumonia |
| Syncytial giant-cell hepatitis | Severe hepatic dysfunction |
| Bone marrow suppression | Cytopenias; worsens engraftment |
| Graft-versus-host disease (exacerbation) | HHV-6 may worsen GVHD |
| Fever and morbilliform rash | Non-specific; common |
| Graft dysfunction/rejection | In solid organ transplant |
| Increased all-cause mortality | High plasma HHV-6 DNA loads correlate with mortality (Harrison's 22E) |
12.3 Hemophagocytic Lymphohistiocytosis (HLH) - Important
- HHV-6 is a recognized trigger of secondary HLH
- Suspect HLH if: Prolonged fever + cytopenias + splenomegaly + hyperferritinemia + elevated triglycerides + reduced NK activity
- HLH-2004 criteria (5 of 8): Fever, splenomegaly, bicytopenia, hypertriglyceridemia/hypofibrinogenemia, hemophagocytosis on BM biopsy, low/absent NK activity, elevated ferritin (>500), elevated sCD25
SECTION 13: SPECIAL SITUATIONS
13.1 Neonates (<3 Months)
- Roseola is rare due to maternal antibody protection
- Any febrile neonate (<28 days) → full sepsis workup (CBC, blood culture, LP, CXR, urine culture) regardless of suspected viral etiology
- HHV-6 can rarely cause neonatal sepsis-like picture
- Congenital HHV-6 occurs (see below)
13.2 Congenital HHV-6 Infection
- Occurs in ~1% of newborns (Red Book AAP; Harrison's 22E)
- Two mechanisms:
- ciHHV-6: Germline passage of chromosomally integrated HHV-6 from parent (most common - ~86%)
- Transplacental infection: From active maternal primary infection or reactivation
- Usually asymptomatic
- Some reports of subtle neurologic defects
- Harrison's 22E (2025): Women with ciHHV-6 may have higher risk of pre-eclampsia or spontaneous abortion
- Diagnostic challenge: ciHHV-6 infants will always test PCR-positive - must use quantitative/droplet digital PCR + parental testing to differentiate from active infection
13.3 HIV-Infected Children
- In vitro: HHV-6 may both increase AND decrease HIV-1 replication depending on conditions
- No definitive evidence that HHV-6 accelerates HIV disease progression (Dermatology 5e)
- However: HHV-6 reactivation more likely with CD4+ depletion
13.4 Transplant Recipients
HSCT Recipients:
- HHV-6 reactivation in ~50% (peak 2-4 weeks post-transplant)
- Higher risk: Allelic-mismatched donors (haploidentical, cord blood), glucocorticoid use
- Monitor with quantitative blood PCR
- Treatment (Red Book AAP): Ganciclovir/valganciclovir or foscarnet for symptomatic HHV-6 disease; specifically recommended for HHV-6 encephalitis in HSCT/solid organ transplant
- Antiviral resistance can occur
Solid Organ Transplant:
- HHV-6 from donor organ (rare)
- Reactivation causing fever, hepatitis, graft dysfunction
13.5 Pregnancy
- HHV-6 reactivation common in pregnancy
- ciHHV-6 in pregnant women: Possible higher risk of pre-eclampsia, spontaneous abortion (Harrison's 22E 2025 - recent finding requiring further study)
- Congenital infection via transplacental route possible
SECTION 14: PROGNOSIS
- Immunocompetent children: Excellent prognosis; complete recovery within 1 week
- Fever resolves in 3-7 days; rash fades in 1-5 days without sequelae
- No long-term neurological deficits from uncomplicated roseola
- No recurrence (lifelong immunity after primary infection in most)
- Latency: HHV-6 persists lifelong in latent state in CD4+ T cells, CNS, salivary glands; asymptomatic in immunocompetent individuals
- Immunocompromised: Guarded prognosis depending on severity of reactivation disease; limbic encephalitis in HSCT carries significant morbidity/mortality
SECTION 15: PREVENTION
15.1 Infection Control
- Hand hygiene: Handwashing with soap and water - most effective measure
- Respiratory etiquette: Cover coughs/sneezes; avoid sharing utensils/saliva
- HHV-6 is enveloped → susceptible to standard disinfectants (alcohol-based sanitizers, soap)
15.2 Daycare Precautions
- Exclude from daycare until fever-free for 24 hours
- No prolonged exclusion needed (virus shed asymptomatically in saliva by adults anyway)
- Clean surfaces and toys regularly
15.3 Vaccine Status
- No vaccine available for HHV-6 or HHV-7 as of 2026
- Research into HHV-6 vaccines is ongoing
- MMR vaccine indirectly protects against measles and rubella (important differentials)
15.4 Antiviral Prophylaxis
- Not routinely recommended for immunocompetent individuals
- Ganciclovir prophylaxis may prevent HHV-6 reactivation in high-risk BMT patients (reported in literature; further double-blind trials needed per Medscape)
SECTION 16: 40 VIVA QUESTIONS WITH ANSWERS
"These are questions that senior examiners at DM Pediatrics and MD finals ask. Learn every answer."
Q1. What are the two causative agents of roseola infantum?
A: HHV-6B (primary, major cause) and HHV-7 (less common). Occasionally adenoviruses, coxsackieviruses, and echoviruses can mimic roseola.
Q2. Why is it called "Sixth disease"?
A: It is the 6th in the historical numbering of classical childhood exanthems: 1st-Measles, 2nd-Scarlet fever, 3rd-Rubella, 4th-Duke's disease (obsolete), 5th-Erythema infectiosum (Parvovirus B19), 6th-Roseola infantum.
Q3. What is the cellular receptor for HHV-6?
A: CD46 (a complement regulatory protein expressed on CD4+ T lymphocytes and many other cell types).
Q4. Why does the rash appear AFTER fever resolves?
A: The rash is immune-mediated (not direct viral cytopathic effect). The adaptive CD8+ T cell response clears viremia (fever resolves), and the subsequent immune complex deposition and vasodilatory inflammatory response in dermal vessels produces the rose-pink exanthem.
Q5. What is the incubation period of HHV-6?
A: 5-15 days, average 9-10 days.
Q6. What are Nagayama spots?
A: Erythematous red papules on the soft palate and uvula (with ulcers at the palatoglossal junction) seen in roseola infantum. They may precede the skin exanthem and aid early diagnosis.
Q7. What CBC finding is characteristic of roseola?
A: Leukopenia with relative lymphocytosis (WBC typically <4,000/mm³ with >50% lymphocytes).
Q8. How common are febrile seizures in roseola?
A: 10-15% of children with primary HHV-6 infection develop febrile seizures. HHV-6 is responsible for 10-20% of ALL febrile seizures in infancy.
Q9. What is ciHHV-6 and why is it clinically important?
A: Chromosomally integrated HHV-6 occurs in ~1% of the population due to germline integration of HHV-6 into telomeres. These individuals always test PCR-positive for HHV-6 (even at high viral loads) and may be mistakenly diagnosed with active HHV-6 disease. Droplet digital PCR and parental testing help distinguish ciHHV-6 from active infection.
Q10. What is Post-Transplant Acute Limbic Encephalitis (PALE)?
A: A specific syndrome of HHV-6B reactivation in HSCT recipients characterized by anterograde amnesia, seizures, insomnia, confusion, and SIADH. MRI shows mesial temporal signal abnormalities. Cord blood transplant recipients have highest risk.
Q11. What antiviral drugs are used for HHV-6 disease in immunocompromised patients?
A: Ganciclovir (or valganciclovir) or foscarnet. Both are active against HHV-6. Recommended by Red Book AAP for HHV-6 encephalitis in HSCT/solid organ transplant patients.
Q12. How does the rash of roseola differ from measles rash?
A: Roseola: pink-rose, discrete, maculopapular with white halo, trunk-first, appears AFTER fever; no cephalocaudal spread; no Koplik spots; no cough/coryza/conjunctivitis (3 C's). Measles: red-brown confluent maculopapules, cephalocaudal spread from hairline downward, appears DURING fever on day 3-4, preceded by Koplik spots, 3 C's prominent.
Q13. What is the pathognomonic clinical finding of roseola?
A: Rose-pink maculopapular rash with white halo appearing AFTER defervescence, in an infant 6-24 months. Nagayama spots (if present) are strongly supportive.
Q14. What percentage of primary HHV-6 infections present with the classic roseola rash?
A: Only ~23-30%. The majority (70-80%) present with undifferentiated febrile illness without rash (Fitzpatrick's; Dermatology 5e).
Q15. What is the mechanism of febrile seizures in HHV-6 infection?
A: Multifactorial: (1) rapid rise in temperature, (2) direct neurotropism of HHV-6 for astrocytes/neurons increasing neuronal excitability, (3) cytokine-mediated (IL-6) lowering of seizure threshold.
Q16. Name three genetic mutations associated with severe CNS disease during primary HHV-6 infection.
A: RandBP2, POLG, and carnitine palmitoyl-transferase 2 (CPT2) gene mutations (Red Book AAP).
Q17. What is the difference between HHV-6A and HHV-6B?
A: HHV-6B causes roseola infantum and post-transplant disease. HHV-6A has no clearly established disease association (possible association with Hashimoto disease and MS). Both classified as separate species since 2012.
Q18. Why are infants aged 6-24 months predominantly affected?
A: Maternal IgG antibodies protect neonates, but wane by 6 months. This creates a window of susceptibility that persists until the infant develops their own immunity through infection (90% seropositive by 3-4 years).
Q19. What is the role of LP in roseola presenting with febrile seizure?
A: LP is NOT routinely required for simple febrile seizure in a child >18 months with a known viral diagnosis. LP is indicated if: meningeal signs present, infant <12-18 months (subtle signs of meningitis), complex febrile seizure, prior antibiotic exposure, immunocompromised state, or persistent encephalopathy.
Q20. What are Koplik spots and how do they differ from Nagayama spots?
A: Koplik spots (measles): Bluish-white granules on red base on buccal mucosa (opposite lower molars); pathognomonic; appear 1-2 days before measles rash. Nagayama spots (roseola): Erythematous red papules on soft palate/uvula; appear during fever; may precede skin rash.
Q21. What is the "happy febrile infant" sign and its significance?
A: Despite temperatures of 39-40°C, children with roseola remain alert, active, and playful. This distinguishes roseola from bacterial infections where the child appears toxic and lethargic.
Q22. What is the seasonal pattern of HHV-6 infection?
A: Most common in spring (Fitzpatrick's); Red Book AAP states infections occur throughout the year without a seasonal pattern. Summer and fall epidemics also reported.
Q23. How is HHV-6 transmitted?
A: Primarily through respiratory secretions/saliva. Adults (especially parents and older siblings) asymptomatically shed HHV-6 in saliva and serve as the source for primary infant infection. Also: cervical secretions (possible perinatal route), donor organ (transplant).
Q24. What is the role of procalcitonin in differentiating roseola from bacterial infection?
A: Normal or low procalcitonin (<0.5 ng/mL) + leukopenia strongly suggests viral etiology (roseola). High procalcitonin (>2 ng/mL) + leukocytosis with neutrophilia suggests bacterial co-infection.
Q25. What are the indications for MRI in a child with roseola?
A: Focal neurological signs, prolonged postictal state, focal seizures, encephalopathy persisting after seizure, suspicion of HHV-6 encephalitis (especially immunocompromised - look for mesial temporal T2/FLAIR signal changes).
Q26. What is the rash distribution in roseola and why?
A: Trunk first, then neck, proximal extremities, occasionally face. Palms and soles are typically spared. The truncal predominance reflects the distribution of dermal vasculature where immune complex deposition occurs first.
Q27. What is the significance of a bulging fontanelle in roseola?
A: Indicates mild aseptic meningeal irritation from cytokine-mediated CNS inflammation. Usually benign and resolves. However, if child is toxic or fontanelle is tense → mandatory LP to rule out bacterial meningitis.
Q28. Can roseola cause encephalitis in immunocompetent children?
A: Yes, but rarely. HHV-6 encephalitis in immunocompetent children is uncommon but recognized. In immunocompromised children (especially HSCT), it is a serious and defined complication (PALE).
Q29. What is hemophagocytic syndrome (HLH) in the context of HHV-6?
A: HHV-6 is a recognized trigger of secondary (acquired) HLH - a life-threatening hyperinflammatory syndrome. Suspect if: prolonged fever + cytopenias + splenomegaly + hyperferritinemia (>500, often >10,000) + hemophagocytosis on bone marrow biopsy.
Q30. How does HHV-7 differ from HHV-6 in causing roseola?
A: HHV-7 causes less common and later-onset roseola (age at infection slightly older than HHV-6). HHV-7 rash is lighter and presents later in the disease course. HHV-7 seroprevalence: most acquire it slightly later than HHV-6 but nearly universally by adulthood (75% shed in saliva of adults).
Q31. What is the role of EEG after febrile seizure in roseola?
A: NOT indicated after simple febrile seizure. Indicated if complex febrile seizure, concern for epileptic disorder, suspicion of encephalitis, or repeated unprovoked seizures.
Q32. Name the drugs for status epilepticus management.
A: Step 1: Benzodiazepines (IV diazepam 0.3 mg/kg, buccal/intranasal midazolam 0.2-0.3 mg/kg). Step 2 (if refractory): IV phenobarbitone 20 mg/kg OR IV fosphenytoin 20 PE/kg. Step 3 (refractory SE): IV valproate, levetiracetam, anesthesia (midazolam/propofol/thiopental infusion).
Q33. What precautions should you give parents regarding fever management?
A: Paracetamol 10-15 mg/kg every 4-6 hours (max 60 mg/kg/day); avoid aspirin; maintain hydration; sponging with tepid water; do NOT bundle the child during fever; return immediately if seizure/dark rash/very lethargic.
Q34. What is the recurrence risk of roseola?
A: Essentially nil after primary infection in immunocompetent individuals - lifelong immunity develops. However, HHV-6 persists in latency and can reactivate asymptomatically or symptomatically in immunocompromised states.
Q35. What is the role of corticosteroids in roseola?
A: No role in uncomplicated roseola. In HHV-6 reactivation in transplant patients, corticosteroids (used for GVHD) may worsen HHV-6 reactivation.
Q36. What is the "sea of red with isles of white" rash?
A: Characteristic of dengue fever - widespread erythema with scattered pale islands (normal skin). Distinct from the "discrete rose macules with white halos" of roseola.
Q37. When should you suspect drug eruption vs roseola?
A: Drug eruption if: drug history 7-14 days prior, pruritic rash, morbilliform or urticarial morphology, eosinophilia on CBC, timing coincides with drug rather than defervescence, no Nagayama spots.
Q38. What HHV-6 DNA levels in whole blood suggest ciHHV-6 vs active infection?
A: ciHHV-6: ~10⁶ copies/whole blood (approximately 1 copy per cell); present in ALL samples consistently. Active infection: variable, typically lower; does not persist at consistently high levels. Droplet digital PCR comparing viral DNA to human cell number can identify ciHHV-6.
Q39. What is the significance of mesial temporal signal changes on MRI in HHV-6?
A: Highly suggestive of HHV-6 limbic encephalitis - especially in HSCT recipients. This specific pattern (T2/FLAIR hyperintensity in hippocampus/amygdala) is characteristic of post-transplant acute limbic encephalitis (PALE) caused by HHV-6B reactivation.
Q40. What is the first-line antiviral for HHV-6 encephalitis in HSCT recipients?
A: Ganciclovir or foscarnet (both have activity against HHV-6). Valganciclovir (oral) can be used as step-down. Red Book AAP recommends these for HHV-6 encephalitis in HSCT/solid organ transplant patients. Note: Acyclovir has minimal activity against HHV-6.
SECTION 17: OSCE STATIONS
Station 1: History Taking (7 minutes)
Scenario card for student: "A 14-month-old child is brought to you. The mother says the child has had fever for 4 days and a new rash appeared today. Take a relevant history."
Marks scheme - Key history points:
| History Domain | Key Questions |
|---|
| Presenting complaint | Onset, duration, pattern of fever; onset/duration of rash |
| Fever characterization | Maximum temperature, diurnal variation (peaks in evening), response to antipyretics |
| Rash | When did rash appear relative to fever? Was fever present when rash started? Color? Itching? Distribution? Blanching? |
| Associated symptoms | Irritability, loose stools, rhinorrhea, cough, oral lesions, seizures |
| Behavior | "Is the child active/playful or lethargic?" |
| Birth + Developmental history | Prematurity, immunodeficiency |
| Immunization history | Up to date? Recent MMR (post-MMR rash is a differential) |
| Drug history | Any antibiotics, other medications (rule out drug rash) |
| Contact history | Sick contacts, daycare attendance, siblings |
| Family history | Febrile seizures in family (risk factor) |
Red flags to specifically ask about:
- Seizure? (Duration, type, recovery)
- Non-blanching rash?
- Decreased level of consciousness?
- Stiff neck?
- Poor feeding/decreased urine output (dehydration)?
Station 2: Physical Examination (7 minutes)
Scenario: "Examine this 12-month-old child who presented with 4-day fever that resolved yesterday and developed a rash this morning. You have 7 minutes."
Marks scheme:
1. Wash hands, introduce yourself, explain to "parent" (examiner)
2. General inspection: Appearance (alert/toxic), hydration, rash visible?
3. Vital signs: Temperature, HR, RR, SpO2 (state you would check these)
4. Skin: Undress completely; describe rash (morphology, distribution,
blanching test with glass slide)
5. Head: Anterior fontanelle (flat/bulging/tense), scalp
6. Eyes: Conjunctivitis? Palpebral edema?
7. Ears: Otoscopy - tympanic membranes
8. Oral cavity: Nagayama spots on soft palate, uvula; Koplik spots?;
Strawberry tongue?; Pharynx
9. Lymph nodes: Occipital, posterior cervical, anterior cervical,
submandibular, inguinal
10. Respiratory: Auscultation
11. Cardiovascular: Heart sounds, pulse
12. Abdomen: Hepatomegaly, splenomegaly
13. Neurology: Neck stiffness (Kernig's, Brudzinski's), tone, reflexes
14. Summarize findings to examiner
Station 3: Rash Identification Station (5 minutes)
Instructions: "You will be shown 4 clinical photographs. For each, identify the rash and give one clinical differentiating feature from roseola infantum."
Expected answers:
| Photo | Diagnosis | Key differentiating feature from Roseola |
|---|
| Measles rash | Measles (Rubeola) | Cephalocaudal spread, rash appears DURING fever, 3 C's, Koplik spots |
| Slapped cheek rash | Erythema Infectiosum (Fifth disease, Parvovirus B19) | Intense facial erythema ("slapped cheek") then lacy reticular body rash; school-age children |
| Fine papular sandpaper rash | Scarlet Fever | Sandpaper texture, circumoral pallor, strawberry tongue, petechiae on palate |
| Purpuric/petechial rash | Meningococcemia | NON-BLANCHING, rapidly progressive, septic shock, emergency! |
Station 4: Parent Counselling (7 minutes)
Scenario: "A 10-month-old child has been diagnosed with Roseola Infantum. Counsel the anxious mother who is worried about the rash that appeared after the fever resolved."
Marks scheme - key points:
| Communication Point | Marks |
|---|
| Introduce yourself, establish rapport | 1 |
| Ask what mother already understands | 1 |
| Explain: "Roseola is a common viral illness" | 2 |
| Explain: "Rash appears after fever - is a GOOD sign (immune response)" | 3 |
| Prognosis: "Rash will disappear in 1-2 days; complete recovery expected" | 2 |
| Management: Paracetamol dosing, hydration, continue feeds | 2 |
| Return to hospital if: seizure, dark rash, very drowsy, high fever returns | 3 |
| Daycare: Return when fever-free 24 hours | 1 |
| Questions from mother - answers empathetically | 1 |
SECTION 18: 30 CLINICAL PEARLS
"These pearls have been forged over 30 years at the bedside. Write them down."
-
"Rose after the fever goes" - the single most memorable fact about roseola.
-
The Happy Febrile Infant: A child with temperature 40°C who is smiling and alert → think roseola; the same child appearing toxic → think serious bacterial infection.
-
Nagayama spots before the rash: Look in the mouth of every febrile infant. Soft palate papules may be your early clue to diagnose roseola before the rash appears.
-
Leukopenia in a febrile infant: When CBC shows WBC <4,000 with relative lymphocytosis in a 6-24-month-old with high fever - strongly suggests HHV-6.
-
The "injected TM trap": Inflamed tympanic membranes in roseola do NOT mean bacterial otitis media. Check clinical context before prescribing antibiotics.
-
Rash + defervescence = reassurance: When a febrile child develops rash as the fever breaks, parents are often terrified. Explain that this is the best possible sign - the fever has cleared and the immune system has "won."
-
ciHHV-6 trap: If a PCR shows very high HHV-6 DNA (close to 1 copy per cell) in all samples including CSF - suspect chromosomal integration, not active encephalitis.
-
HHV-6 is the #1 cause of febrile seizures: Every time a resident says "it's just a febrile seizure" - remember that HHV-6 is directly neurotropic and can cause encephalitis. The decision to do LP must be individualized.
-
Rash duration <48 hours: If you see a child with a pinkish truncal rash that their parents said was present 3 days ago but is now fading - you may be seeing roseola resolving. History of preceding fever is the key.
-
No antiviral, no antibiotic, no steroid: Uncomplicated roseola needs none of these. The management is education, antipyretics, hydration.
-
HHV-6 in transplant patients = emergency: Post-HSCT fever at 2-4 weeks should always trigger HHV-6 PCR monitoring. Delay in diagnosis of limbic encephalitis worsens outcome.
-
Ganciclovir/foscarnet, NOT acyclovir: Unlike HSV/VZV where acyclovir works, HHV-6 has minimal sensitivity to acyclovir. Always use ganciclovir or foscarnet for HHV-6 disease.
-
Seasonal peak in spring: Important for epidemiological context in exams.
-
Cord blood transplant = highest risk for PALE: Among HSCT subtypes, cord blood recipients have highest risk of post-transplant acute limbic encephalitis.
-
Mothers' saliva is the source: Caregivers asymptomatically shed HHV-6 in saliva throughout life. Telling parents "where it came from" - it came from them (or older siblings), and that is normal.
-
The palpebral edema sign: Eyelid edema giving a "sleepy appearance" in an otherwise alert febrile infant → characteristic of roseola (Fitzpatrick's).
-
Rash starts on trunk, not face: Unlike measles (starts at hairline/face), scarlet fever (neck/trunk), rubella (face first) - roseola rash is TRUNK-FIRST.
-
MRI mesial temporal signal: In any post-transplant patient with HHV-6 + confusion/amnesia/seizures → MRI showing hippocampal signal = PALE until proven otherwise.
-
HHV-6 and MS: HHV-6 (like EBV) has been implicated in the pathogenesis of multiple sclerosis, though the association vs causation remains to be established (Harrison's 22E 2025).
-
Seroprevalence is NOT immunity to disease: In adults, high HHV-6 seroprevalence means latent infection, but reactivation in immunocompromised individuals can cause life-threatening disease.
-
Never diagnose roseola in a neonate: A febrile neonate (<28 days) gets a full sepsis workup regardless. Roseola is rare before 3 months.
-
LP in infant <12 months with first febrile seizure: Always consider - meningeal signs are subtle or absent in this age group.
-
Roseola rash is non-pruritic: If itching is prominent, think drug rash, viral exanthem other than roseola, or urticaria.
-
RandBP2 and POLG mutations: Children with these mutations who get HHV-6 infection can develop severe encephalopathy - a genetic susceptibility link (Red Book AAP).
-
Hepatomegaly in roseola: Mild, transient. If hepatomegaly is prominent with raised transaminases → think HLH, other viral hepatitis (EBV, CMV, adenovirus).
-
HHV-7 roseola is lighter: The rash in HHV-7-induced exanthem subitum is lighter in color and appears later in the disease course than HHV-6 infection (Dermatology 5e).
-
Antipyretic choice in dengue-endemic areas: Use paracetamol; AVOID ibuprofen (NSAIDs increase bleeding risk in dengue). In any febrile child where dengue is possible → paracetamol only until dengue ruled out.
-
The white halo sign: Discrete rose-red maculopapule surrounded by a pale halo = essentially pathognomonic for roseola.
-
HHV-6 encephalitis in immunocompetent adult: Increasingly recognized; consider in adult with temporal lobe encephalitis of unknown cause (PMID 39301106).
-
The retrospective diagnosis: In practice, you often diagnose roseola retrospectively - a child seen during the febrile phase, sent home with "viral fever," returns with a rash after fever has broken. Connecting these two visits makes the diagnosis.
SECTION 19: COMMON MISTAKES BY RESIDENTS
"In 30 years, I have seen the same mistakes made repeatedly. Learn from others' errors."
1. Diagnosing bacterial otitis media due to red eardrums
HHV-6 routinely causes injected tympanic membranes. Prescribing antibiotics without AOM criteria (bulging, effusion, loss of light reflex) is incorrect.
2. Panicking when rash appears and calling it drug rash or allergic reaction
Parents often return to ED alarmed when the rash appears after the fever breaks. Residents sometimes misdiagnose this as antibiotic allergy or drug rash and stop medications. Always ask: "When did the fever break? When did the rash start?"
3. Doing extensive workup in a typical case
CBC, blood cultures, CXR, urine culture for a well-appearing 12-month-old with 3-day fever + rash after defervescence + no red flags = unnecessary. Clinical diagnosis saves time and money.
4. Missing the meningococcemia diagnosis
Conversely - NOT doing a diascopy test (blanching test) on every rash. A non-blanching purpuric rash is a medical emergency, not roseola. This mistake can be fatal.
5. Not checking the soft palate for Nagayama spots
A comprehensive oral examination is often skipped. Nagayama spots in a febrile infant can be the earliest clue to roseola before the skin exanthem appears.
6. Assuming "febrile seizure = simple febrile seizure"
Always classify: simple vs complex. Complex febrile seizures (focal, prolonged >15 min, or recurrent in 24 hours) require more extensive evaluation, including LP consideration and possible neuroimaging.
7. Using acyclovir for HHV-6 encephalitis
Acyclovir is not effective against HHV-6. Use ganciclovir or foscarnet.
8. Interpreting a single HHV-6 IgM positive as diagnostic
IgM to HHV-6 is unreliable - may be absent in primary infection and positive in asymptomatic adults due to reactivation. Fourfold IgG rise or documented seroconversion is more meaningful.
9. Missing HHV-6 reactivation in a post-HSCT patient
Not thinking about HHV-6 in a febrile, confused post-transplant patient (2-4 weeks post-HSCT). Always include HHV-6 PCR in the workup.
10. Not counselling parents about febrile seizure risk
Failing to warn parents that ~10-15% of roseola children can have febrile seizures, and providing home management guidance (including when to call emergency services).
11. Not doing LP in infant <12 months with first febrile seizure
Signs of meningitis are subtle in infants. LP threshold should be low, not high, in this age group.
12. Confusing the rash timing with rubella
Rubella rash appears WITH or just after fever, spreads face → body. Roseola: strictly AFTER fever resolves, trunk-first.
SECTION 20: RECENT ADVANCES (2021-2026)
"Let me briefly cover what is new in the last 5 years - important for your research awareness."
1. Leung et al. 2024 - Updated Review (PMID 36411550)
- Curr Pediatr Rev 2024;20(2):119-128
- Comprehensive updated review confirming all classical clinical features
- Emphasizes that failure to recognize roseola leads to unnecessary investigations, misuse of healthcare expenditure, and delayed treatment of mimickers
2. Harrison's 22E (2025) - ciHHV-6 and Pregnancy
- New concern: Women with ciHHV-6 may have higher risk of pre-eclampsia or spontaneous abortion
- Reinforces importance of distinguishing ciHHV-6 from active infection
3. HHV-6 Limbic Encephalitis in Immunocompetent Adults (PMID 39301106)
- Webb et al., Open Forum Infect Dis 2024
- HHV-6 encephalitis increasingly recognized in immunocompetent adults (not just transplant patients)
- Review of diagnostic challenges and management
4. Chromosomal Integration - Expanded Understanding
- Droplet digital PCR now preferred over standard qPCR for ciHHV-6 identification
- Germline integration of HHV-6A is actually more common than HHV-6B integration in general population
5. Potential Role in Multiple Sclerosis
- HHV-6 (particularly HHV-6A) along with EBV being actively studied in MS pathogenesis
- Molecular mimicry and myelin destruction pathways being investigated
6. HHV-6 and DRESS Syndrome
- HHV-6 (plus EBV, CMV, HHV-7) reactivation confirmed as driver of drug reaction with eosinophilia and systemic symptoms (DRESS) - important in the immunocompromised and drug-exposed
7. Genetic Susceptibility Markers
- RandBP2 and POLG mutations increasingly recognized as predisposing to severe HHV-6 CNS disease - potential for genetic screening in severely affected children
SECTION 21: SUMMARY AND REVISION AID
21.1 Key Take-Home Messages
- Roseola infantum = high fever (3-5 days) + rash appearing AFTER defervescence in a 6-24-month infant
- HHV-6B is the primary cause; 30% of primary HHV-6 infections show the classic rash
- The child appears happy and active despite high fever
- Leukopenia is characteristic on CBC
- Nagayama spots (soft palate red papules) are a diagnostic clue
- Management is supportive; no antiviral for uncomplicated disease
- HHV-6 is the #1 cause of febrile seizures in infancy
- ciHHV-6 (in 1% of population) always tests PCR-positive - a diagnostic pitfall
- In immunocompromised patients (especially HSCT), HHV-6 reactivation is serious - treat with ganciclovir/foscarnet
- The rash is immune-mediated - reassure parents it is a good sign
21.2 MNEMONICS
Mnemonic: ROSEOLA - Clinical features
- R - Rose-pink rash (trunk-first, after fever)
- O - Occipital lymphadenopathy
- S - Sixth disease / Sudden fever
- E - Exanthem Subitum
- O - Only 30% show classic rash (70% undifferentiated fever)
- L - Leukopenia (characteristic CBC)
- A - Age 6-24 months (peak)
Mnemonic: SIX C's of Roseola
- S - Sixth disease
- I - Infant (6-24 months)
- X - eXanthem Subitum
- C1 - Chromic (lifelong latency)
- C2 - CD4+ T cell tropism; CD46 receptor
- C3 - Clears fever first, THEN rash appears
Mnemonic for Differential: "MADE SRP" (diseases with fever + rash)
- M - Measles (rash DURING fever, cephalocaudal, Koplik)
- A - Adenovirus (pharyngoconjunctival fever)
- D - Dengue (thrombocytopenia, biphasic fever)
- E - Enteroviral exanthem (HFMD, oral ulcers)
- S - Scarlet fever (sandpaper rash, strawberry tongue)
- R - Roseola (rash AFTER fever)
- P - Parvovirus B19 (slapped cheek)
21.3 DIAGNOSTIC ALGORITHM
FEBRILE INFANT 6-24 MONTHS
│
┌───────┴───────┐
Fever present Fever resolved
(days 1-5) + Rash appeared
│ │
Leukopenia on CBC? ROSEOLA INFANTUM
Nagayama spots? │
Happy, active? No investigations
│ needed (typical)
Consider HHV-6 │
(clinical diagnosis) Reassure parents
│ Antipyretics PRN
┌─────────┴─────────┐
Febrile seizure? Rash non-blanching?
│ │
Simple or complex? EMERGENCY - rule out
│ meningococcemia
Simple: reassure
Complex: LP, EEG,
neuroimaging if indicated
21.4 MANAGEMENT ALGORITHM
DIAGNOSIS: ROSEOLA INFANTUM (Typical Presentation)
│
┌───────────┴───────────┐
Immunocompetent child Immunocompromised child
│ │
OUTPATIENT ADMIT
│ │
Paracetamol 10-15 mg/kg HHV-6 PCR (quantitative)
q4-6h PRN fever LFTs, CBC, metabolic panel
Oral hydration Consider ganciclovir/
Parent counselling foscarnet
Return precautions Organ-specific workup
No antiviral Infectious disease consult
No antibiotics
No isolation
│
Febrile seizure occurs?
│
Assess: Simple vs Complex
│
Simple → No LP (if >18 months, typical roseola)
→ Rectal/buccal diazepam at home
→ Parent seizure education
│
Complex or infant <12 months → Consider LP
→ Neuroimaging if focal Sx
→ Admit for observation
21.5 ONE-PAGE REVISION SHEET
╔══════════════════════════════════════════════════════════════════════╗
║ ROSEOLA INFANTUM - HIGH YIELD SUMMARY ║
╠══════════════════════════════════════════════════════════════════════╣
║ CAUSE │ HHV-6B (primary); HHV-7 (secondary) ║
║ AGE │ 6-24 months (peak); 95% cases in <3 years ║
║ SEASON │ Spring (highest); year-round ║
║ RECEPTOR │ CD46 on CD4+ T cells ║
╠══════════════════════════════════════════════════════════════════════╣
║ CLINICAL │ Fever (39.5-40.6°C) × 3-5 days → ABRUPT defervescence ║
║ │ → Rose-pink maculopapular TRUNK-FIRST rash (2-5mm) ║
║ │ → White halo sign (pathognomonic) ║
║ │ → Happy, active child despite high fever ║
╠══════════════════════════════════════════════════════════════════════╣
║ SIGNS │ Nagayama spots (soft palate); Occipital LAP ║
║ │ Palpebral edema; Injected TMs; Bulging fontanelle (mild) ║
╠══════════════════════════════════════════════════════════════════════╣
║ CBC │ LEUKOPENIA + relative LYMPHOCYTOSIS ║
╠══════════════════════════════════════════════════════════════════════╣
║ COMPLICATIONS │ Febrile seizures (10-15%) ← MOST COMMON ║
║ │ Encephalitis (rare in immunocompetent) ║
║ │ HLH, hepatitis, pneumonitis (very rare) ║
║ │ IMMUNOCOMPROMISED: PALE (limbic encephalitis), ║
║ │ bone marrow suppression, graft rejection ║
╠══════════════════════════════════════════════════════════════════════╣
║ TREATMENT │ SUPPORTIVE - Paracetamol, oral hydration ║
║ │ NO antiviral, NO antibiotic (uncomplicated) ║
║ │ Immunocompromised → Ganciclovir/Foscarnet ║
╠══════════════════════════════════════════════════════════════════════╣
║ ciHHV-6 │ 1% of population; always PCR+; NOT active infection ║
╠══════════════════════════════════════════════════════════════════════╣
║ PROGNOSIS│ Excellent; complete recovery; lifelong immunity ║
╠══════════════════════════════════════════════════════════════════════╣
║ REMEMBER │ "ROSE after the fever GOES" ║
║ │ Only 30% of HHV-6 infections show classic rash ║
║ │ HHV-6 = #1 cause of febrile seizures in infancy ║
╚══════════════════════════════════════════════════════════════════════╝
21.6 PG ENTRANCE AND DM PEDIATRICS HIGH-YIELD FACTS
| Fact | High-Yield Level |
|---|
| HHV-6B = major cause of roseola (NOT HHV-6A) | ⭐⭐⭐ |
| Rash appears AFTER defervescence (unique!) | ⭐⭐⭐ |
| 6th disease (1st: Measles, 2nd: Scarlet fever, 3rd: Rubella, 5th: Parvovirus B19) | ⭐⭐⭐ |
| Nagayama spots = soft palate/uvula red papules | ⭐⭐⭐ |
| HHV-6 = #1 cause of febrile seizures in infancy | ⭐⭐⭐ |
| Cellular receptor: CD46 (on CD4+ T cells) | ⭐⭐⭐ |
| Leukopenia on CBC | ⭐⭐⭐ |
| ciHHV-6 in 1% of population; always PCR+ | ⭐⭐⭐ |
| Only 30% of HHV-6 primary infections = classic roseola | ⭐⭐⭐ |
| Ganciclovir/foscarnet for immunocompromised (NOT acyclovir) | ⭐⭐⭐ |
| Post-transplant acute limbic encephalitis (PALE) = HHV-6B reactivation | ⭐⭐⭐ |
| White halo sign around rose-red macules/papules | ⭐⭐ |
| Incubation period: 5-15 days (average 9-10 days) | ⭐⭐ |
| Seasonal peak: Spring | ⭐⭐ |
| HHV-6A vs HHV-6B - distinct species since 2012 | ⭐⭐ |
| Cord blood HSCT = highest risk for PALE | ⭐⭐ |
| RandBP2, POLG mutations → severe HHV-6 CNS disease | ⭐⭐ |
| Palpebral edema/"sleepy appearance" in roseola | ⭐⭐ |
| No vaccine available for HHV-6 | ⭐⭐ |
| HHV-6 and DRESS syndrome (with EBV, CMV, HHV-7) | ⭐⭐ |
SOURCES
This lecture is based on the following authoritative sources:
- Harrison's Principles of Internal Medicine, 22nd Edition (McGraw Hill Medical, 2025) - HHV-6 and HHV-7 chapter
- Red Book: 2021 Report of the Committee on Infectious Diseases (AAP) - Human Herpesvirus 6 (Including Roseola) and 7 chapter
- Dermatology 2-Volume Set, 5th Edition - HHV-6/Exanthem Subitum section
- Fitzpatrick's Dermatology - Human Herpesvirus 6 section
- Sherris & Ryan's Medical Microbiology, 8th Edition - Roseola Infantum chapter
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Edition - HHV-6 and HHV-7 chapter
- Tintinalli's Emergency Medicine, A Comprehensive Study - Roseola Infantum section
- Textbook of Family Medicine, 9th Edition - Other Human Herpesviruses section
- Leung AKC, Lam JM, Barankin B, Leong KF, Hon KL. Roseola Infantum: An Updated Review. Curr Pediatr Rev. 2024;20(2):119-128. PMID 36411550
- Webb G et al. Diagnostic Dilemmas: HHV-6 Encephalitis in Immunocompetent Adults. Open Forum Infect Dis. 2024. PMID 39301106
- StatPearls - Roseola Infantum (NCBI Bookshelf)
"That concludes our 120-minute lecture on Roseola Infantum. This is a disease that every pediatric resident will encounter in their first month. The beauty of roseola is that it teaches you the core of pediatric clinical reasoning: trust the defervescence-rash sequence, know your differentials, counsel your parents well, and resist the urge to over-investigate. See you at the bedside!"
Lecture structured for independent sectional teaching. Each section (Epidemiology, Pathogenesis, Clinical Features, Differential Diagnosis, Management, Febrile Seizures, Viva, OSCE) can be taught as an independent 15-20 minute classroom or slide session.