
Interpret
Reading File
Finding Sources
Finding Sources
Searching the Web
St James Hospital classification anal fistula Grade 2 MRI intersphincteric
Reading File
Reading File
Loading Image
Loading Image
Here is a full interpretation of this MR Fistulogram report:
Patient Summary
Fayis, 42-year-old male - Presenting with right-side perianal swelling and discharge. MRI performed with T1, T2, STIR sequences (axial, coronal, sagittal planes).
What Was Found
1. Fistula Type - Intersphincteric
The tract is T2 hyperintense (bright on T2/STIR), which indicates an active, fluid-filled tract with inflammation. It lies entirely within the intersphincteric plane - the space between the internal and external anal sphincters - without crossing the external sphincter. This is the most common type of anal fistula (roughly 45% of cases).
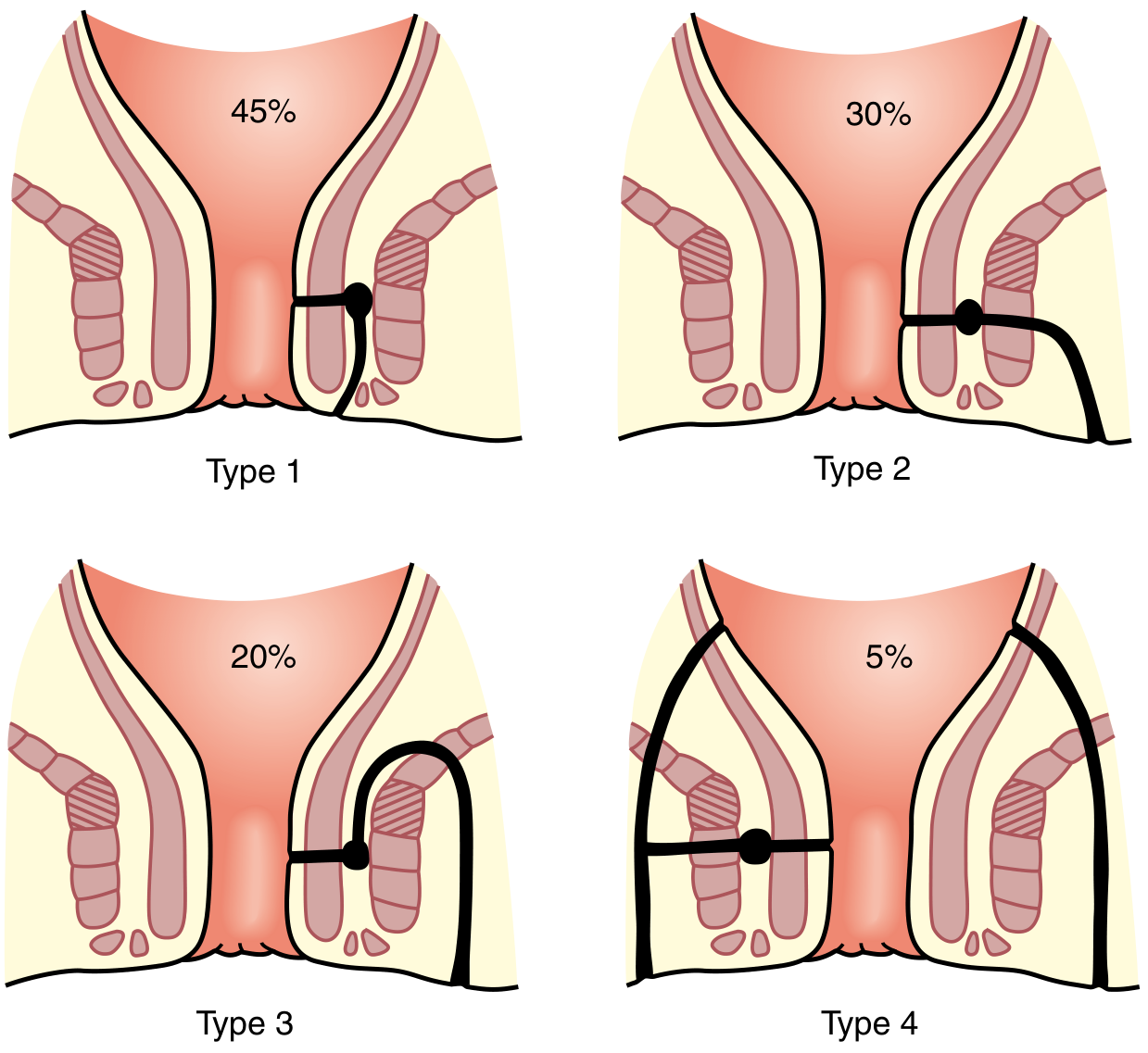
Parks' Classification - This patient has a Type 1 (Intersphincteric) fistula. - Sabiston Textbook of Surgery, p. 2163
2. Internal Opening
- Located approximately 13 mm from the anal verge, at the 6 o'clock position (posterior midline)
- Described as "not clearly visible" - this is common on MRI when edema or inflammation obscures the precise mucosa breach
- The 6 o'clock position is the most common site for cryptoglandular fistula origin (posterior anal glands)
3. Course of the Tract
- Runs inferiorly through the intersphincteric plane
- The inferior margin reaches just below the anal verge and approaches the skin surface in the posterior perianal region
- Total length: 25-30 mm - a short, relatively simple tract
4. External Opening
- Located in the posterior perianal region
- Described as "cutaneous opening indistinct" - the skin opening may not be clearly defined/may be partially healed or intermittently patent
5. Associated Abscess - KEY FINDING
- A small intersphincteric fluid pocket (13 mm transverse x 2 mm thickness) at the level of the inner opening, spanning 6-9 o'clock
- This is a small intersphincteric abscess - it represents active sepsis and undrained infection at the fistula origin
- This is what upgrades the classification from Grade 1 to Grade 2 (see below)
6. Favorable Findings (What Was NOT Found)
| Feature | Finding | Significance |
|---|---|---|
| Side branches | None | Simpler surgery, lower recurrence |
| Supralevator extension | Absent | Not a high/complex fistula |
| Ischioanal fat | Normal | No ischiorectal involvement |
| Sphincter complex | Normal bulk | Continence likely preserved post-op |
Classification
St. James University Hospital MRI Grade 2
This is an MRI-based radiological classification (not Parks'):
| Grade | Description |
|---|---|
| Grade 1 | Simple linear intersphincteric fistula |
| Grade 2 (this patient) | Intersphincteric fistula with intersphincteric abscess or secondary tract |
| Grade 3 | Trans-sphincteric fistula (no abscess) |
| Grade 4 | Trans-sphincteric fistula with ischiorectal abscess |
| Grade 5 | Supralevator or translevator disease |
This patient is Grade 2 specifically because of the small intersphincteric fluid collection at the inner opening. Without it, this would be a Grade 1.
In the Parks' classification, this is a Type 1 Intersphincteric fistula.
In the AGA classification, this is a simple fistula (low intersphincteric tract, single external opening, no horseshoe extension, no supralevator involvement). - Bailey & Love's Short Practice of Surgery, 28th Ed., p. 1458
Clinical Implications
-
Abscess drainage first: The intersphincteric fluid pocket needs to be addressed - it is a source of ongoing sepsis and likely the driver of the patient's swelling and discharge. If not drained, it can perpetuate the fistula or lead to recurrence.
-
Definitive surgical options for this type:
- Fistulotomy (laying open) - the standard treatment for low intersphincteric fistulae; generally safe with low risk to continence since the external sphincter is NOT involved
- Alternatively, intersphincteric fistula tract (LIFT) procedure or advancement flap if sphincter preservation is a priority
-
Good prognosis: The absence of side branches, no supralevator extension, normal sphincter bulk, and no ischiorectal involvement all indicate a favorable surgical anatomy with low complexity.
-
The indistinct inner and outer openings mean the surgeon should probe carefully at the time of examination under anesthesia (EUA), using this MRI as a roadmap. The 6 o'clock position at 13 mm from the verge is the target.
Bottom line: This is an active, low-complexity intersphincteric anal fistula with a small associated abscess at the inner opening. It is amenable to standard surgical management with a good expected outcome. The main preoperative concern is the abscess component, which may require drainage either simultaneously or as a staged procedure.
What to advice
Finding Sources
Finding Sources
Searching the Web
intersphincteric anal fistula with abscess Grade 2 MRI management treatment 2024
Reading File
Reading File
Here is a structured management plan for this patient (Fayis, 42M, intersphincteric fistula with intersphincteric abscess, St. James Grade 2):
Management Advice
Step 1 - Immediate: Address Active Sepsis
The intersphincteric abscess (13 mm at 6-9 o'clock) is the most urgent issue. Active sepsis must be controlled before any definitive fistula repair - attempting closure with ongoing infection will fail.
Admit and arrange Examination Under Anaesthesia (EUA)
- EUA allows proper examination that is not possible in clinic due to pain/guarding
- Confirms the internal opening location (6 o'clock, 13 mm from anal verge)
- Allows abscess drainage at the same sitting
- Do not attempt drainage in the outpatient setting
Abscess drainage technique for intersphincteric abscess:
- Drain transrectally (through the rectal wall) - NOT through the ischioanal fossa
- Drainage across the ischiorectal fossa would artificially convert a simple intersphincteric abscess into a suprasphincteric fistula - a much more complex problem - Current Surgical Therapy 14e, p. 347
Step 2 - Definitive Fistula Surgery
Once sepsis is controlled, definitive treatment depends on sphincter assessment and surgeon preference. For a low intersphincteric fistula in a 42-year-old male the options are:
| Option | Notes | Recommendation |
|---|---|---|
| Fistulotomy (laying open) | First-line for intersphincteric fistulae; safe in men as only internal sphincter is divided | Preferred - can be done at same sitting as EUA if sepsis is mild |
| LIFT procedure | Ligation of Intersphincteric Fistula Tract; sphincter-sparing | Good option if sphincter preservation strongly desired |
| Advancement flap | For complex/recurrent cases | Not needed here |
| Fibrin glue / collagen plug | Low success rates; not preferred for simple fistulae | Not indicated |
Fistulotomy is the standard of care for this type. In this patient - male, no prior anorectal surgery, normal sphincter bulk on MRI - dividing the internal sphincter carries minimal incontinence risk. - Current Surgical Therapy 14e
Step 3 - Perioperative Advice
Pre-op:
- Routine blood work, anaesthetic fitness
- Bowel prep (single enema the morning of surgery is sufficient)
- No specific antibiotic prophylaxis required unless immunocompromised or signs of significant cellulitis
Intraoperative:
- Use MRI as a roadmap - inner opening at 6 o'clock, 13 mm from anal verge
- Probe gently; do not force (risk of creating false passages)
- The external opening in the posterior perianal region may need to be freshened/widened for adequate drainage
- No side branches to worry about (MRI confirmed none)
- No supralevator extension - surgery stays below the levators
Post-op:
- Wound heals by secondary intention - usually 6-12 weeks
- Daily sitz baths after bowel movements
- High-fibre diet + stool softeners to reduce straining
- Wound packing/dressing changes initially
- Clinic review at 2-4 weeks to assess healing
Step 4 - Counselling Points for the Patient
- Surgery is necessary - this will not resolve on its own. Antibiotics alone will not heal a fistula
- There will be an open wound in the perianal area post-op that takes several weeks to heal - set expectations clearly
- Risk of incontinence is very low given the fistula type and his sphincter being intact
- Recurrence rate after fistulotomy for intersphincteric fistula is low (5-10%) but possible if the internal opening is not correctly identified
- Advise him to return immediately if he develops fever, worsening swelling, or spreading redness (sign of spreading sepsis)
What NOT to Do
- Do not prescribe antibiotics alone and send home - will only temporarily suppress symptoms
- Do not attempt transanal or perineal drainage in clinic without anaesthesia
- Do not perform a complex sphincter-cutting procedure - this is a simple intersphincteric tract, not a high/complex one
- Avoid delay - the intersphincteric abscess can extend if left untreated
Summary in one line: Refer to a colorectal/general surgeon for urgent EUA + intersphincteric abscess drainage, followed by fistulotomy as definitive treatment. Prognosis is excellent.
But he doesn't have sepsis
Good clarification. The MRI shows only a small, localised intersphincteric fluid pocket (13 mm x 2 mm) - not systemic sepsis. The patient's main complaint is chronic swelling and discharge, which is typical of a low-grade, smouldering fistula. This actually simplifies management considerably.
Revised Management Advice
The Clinical Picture
This is a chronic, active intersphincteric fistula with a small associated fluid collection - no fever, no cellulitis, no systemic sepsis. The abscess here is essentially a perianal collection at the inner opening, which is part of the fistula anatomy rather than an acute surgical emergency.
What to Advise
1. Surgical Referral - Elective, Not Urgent
Refer to a colorectal surgeon for elective surgery. This is not an emergency. The patient can be listed for a planned procedure.
2. The Operation: EUA + Fistulotomy in One Sitting
Since there is no active spreading sepsis, this can be done as a single-stage procedure:
- Examination Under Anaesthesia (EUA) to confirm anatomy and identify the internal opening at 6 o'clock
- Fistulotomy (laying open the tract) - the definitive treatment
- The small intersphincteric fluid pocket will be naturally debrided/drained when the tract is laid open
- No need for a staged approach (drain first, then repair later)
This is the standard, safe approach for low intersphincteric fistulae in the absence of acute sepsis. - Current Surgical Therapy 14e
3. While Awaiting Surgery
- Sitz baths (warm water soaks) 2-3 times daily - reduces local discomfort and keeps the external opening patent so discharge can drain freely
- High-fibre diet (25-30 g/day) + adequate hydration to keep stools soft and reduce anal trauma with defaecation
- Maintain hygiene - gentle cleaning of the perianal area after each bowel movement; avoid vigorous wiping
- A small pad/dressing over the external opening to manage discharge and protect clothing
- No antibiotics needed - they will not heal the fistula and are not indicated without signs of infection
4. Red Flag Symptoms - Return Immediately If:
- Sudden increase in pain and swelling (abscess expanding)
- Fever or chills (sepsis developing)
- Inability to pass stools
- Spreading redness of the perianal skin
Prognosis - Reassure the Patient
- Fistulotomy success rate for low intersphincteric fistulae is over 90%
- Incontinence risk is very low - he is male, 42 years old, with normal sphincter bulk confirmed on MRI, and only the internal sphincter will be divided
- No side branches, no suprasphincteric extension - this is straightforward anatomy
- Wound heals by secondary intention over 6-10 weeks post-op
- He should expect a period of wound care after surgery but full recovery is the norm
Bottom line for the referring doctor: Elective surgical referral for single-stage EUA + fistulotomy. No urgent intervention needed. Advise sitz baths and hygiene measures in the interim. Reassure the patient - this is a simple fistula with an excellent surgical outcome.
This is a shared conversation. Sign in to Orris to start your own chat.