Colon cancer sugery and parts which are remved and with pictures and main difference
Reading File
Finding Sources
Finding Sources
Searching the Web
colon cancer surgery types parts removed hemicolectomy colectomy diagrams
Finding Sources
Reading Web Page
https://www.mayoclinic.org/tests-procedures/colon-cancer-sur…
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive textbook and visual information. Let me compile the full answer.
Colon Cancer Surgery: Types, Parts Removed, and Key Differences
Overview
Surgery is the primary treatment for colon cancer. The operation is called a colectomy (or colon resection) - it removes the cancerous segment of colon plus a margin of healthy tissue on each side, the attached mesentery, and the regional lymph nodes. The specific type depends entirely on where the tumor sits in the colon.
The Colon: Anatomy at a Glance
The colon is divided into segments, each with its own blood supply, which determines what gets removed:
- Cecum - Ascending colon - Hepatic flexure - Transverse colon - Splenic flexure - Descending colon - Sigmoid colon - Rectum
Overview: All Surgery Types

Types of Surgery and Parts Removed
1. Right Hemicolectomy
Tumor location: Cecum or ascending colon
Parts removed:
- Terminal ileum (last part of small bowel, ~10 cm)
- Cecum
- Ascending colon
- Right portion of transverse colon
- Ileocolic artery, right colic artery (if present), and right branch of middle colic vessels
- Associated mesentery and lymph nodes
Anastomosis: Small bowel (ileum) reconnected to mid-transverse colon (ileocolic anastomosis)
2. Extended Right Hemicolectomy
Tumor location: Hepatic flexure or right transverse colon
Parts removed: Everything in right hemicolectomy PLUS most of the transverse colon. The entire middle colic vessels are divided at their origin (not just the right branch).
3. Transverse Colectomy
Tumor location: Mid-transverse colon
Parts removed:
- Transverse colon segment
- Middle colic vessels divided at origin
- Requires mobilization of both hepatic and splenic flexures to allow tension-free anastomosis
4. Left Hemicolectomy
Tumor location: Distal transverse colon, splenic flexure, or proximal descending colon
Parts removed:
- Left half of transverse colon
- Splenic flexure
- Descending colon
- Left branch of middle colic artery + left colic artery (ligated at its origin from the inferior mesenteric artery)
- Associated mesentery and lymph nodes

5. Sigmoid Colectomy
Tumor location: Sigmoid colon
Parts removed:
- Sigmoid colon
- Superior rectal artery and its takeoff from the inferior mesenteric artery
- Associated mesentery and lymph nodes
Anastomosis: Descending colon reconnected to upper rectum
6. Subtotal / Total Colectomy
Tumor location: Multiple synchronous tumors, or hereditary syndromes (Lynch syndrome, FAP, IBD-related cancer)
Parts removed:
- Subtotal: Most of the colon, leaving the rectum
- Total: Entire colon, leaving the rectum intact (ileorectal anastomosis)
7. Total Proctocolectomy
Tumor location: When both colon and rectum are involved
Parts removed: Entire colon AND rectum - requires a permanent ileostomy or ileal pouch-anal anastomosis (IPAA)
Vessel Ligation Diagram (Right-Sided Resection)
This textbook diagram shows the vessels ligated during a right-sided resection - ileocolic pedicle, right colic vessels, and middle colic vessels at their origins:
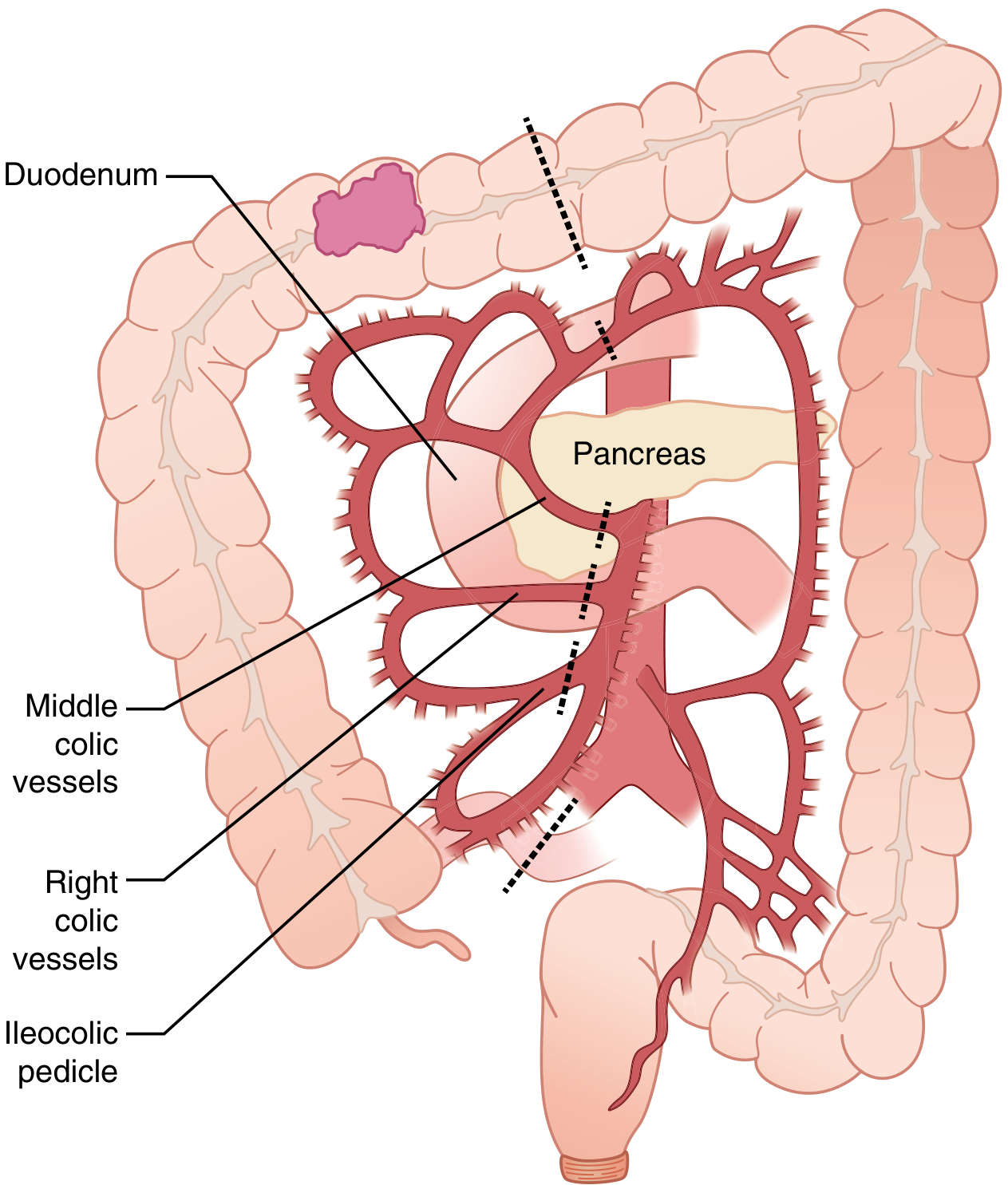
(Sabiston Textbook of Surgery, Fig. 96.5)
What Is ALWAYS Removed (Regardless of Type)
| Structure | Why |
|---|---|
| Cancerous colon segment | Primary tumor removal |
| 5+ cm healthy margin on each side | Prevent positive margins |
| Mesentery (fatty tissue holding colon) | Contains lymphatic channels |
| Regional lymph nodes (aim: 12+) | Staging and cure |
| Draining blood vessels | Oncologic control |
| Attached omentum segment | Possible lymph node involvement |
Key Differences: Quick Comparison Table
| Surgery | Tumor Location | Main Parts Removed | Vessels Ligated | Anastomosis |
|---|---|---|---|---|
| Right hemicolectomy | Cecum, ascending colon | Cecum, ascending colon, terminal ileum | Ileocolic + right branch middle colic | Ileum to transverse colon |
| Extended right hemicolectomy | Hepatic flexure, right transverse | Above + most transverse colon | Ileocolic + ALL middle colic | Ileum to distal transverse |
| Transverse colectomy | Mid-transverse colon | Transverse colon | Middle colic only | Ascending to descending |
| Left hemicolectomy | Splenic flexure, descending colon | Left transverse + descending colon | Left branch middle colic + left colic | Transverse to sigmoid |
| Sigmoid colectomy | Sigmoid colon | Sigmoid colon | IMA branches (superior rectal) | Descending colon to rectum |
| Subtotal colectomy | Multiple/hereditary | Most of colon (rectum spared) | IMA + SMA branches | Ileum to rectum |
| Total proctocolectomy | Colon + rectum | Entire colon + rectum | All colonic vessels | Ileostomy or pouch |
Open vs. Laparoscopic vs. Robotic Surgery
All the above resections can be performed by three approaches:
| Approach | How | Key Points |
|---|---|---|
| Open (laparotomy) | Single long abdominal incision | Preferred for locally advanced/obese cases |
| Laparoscopic | 3-5 small ports | Less pain, faster recovery, shorter stay - same cancer outcomes |
| Robotic | Robot-assisted ports | Lower conversion rates, better visualization, higher cost |
Multiple large randomized trials have confirmed that laparoscopic colectomy produces equivalent long-term cancer outcomes to open surgery, with better short-term recovery. - Mulholland and Greenfield's Surgery, 7th ed.
Stoma (Colostomy/Ileostomy)
Sometimes the two bowel ends cannot be safely rejoined (due to infection, poor blood supply, or radiation). In that case, the surgeon brings the bowel end out through the abdominal wall as a stoma - either temporary (closed later) or permanent. An ileostomy uses small bowel; a colostomy uses large bowel.
Sources: Mulholland and Greenfield's Surgery (7th ed.), Sabiston Textbook of Surgery, Mayo Clinic, Cleveland Clinic
Write a ten matks ans on peripheral artery occlusion disease
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive textbook material from multiple authoritative sources. Let me compose the full 10-mark answer.
Peripheral Arterial Occlusive Disease (PAOD) - 10-Mark Answer
Definition
Peripheral Arterial Disease (PAD) broadly denotes stenotic, occlusive, and aneurysmal diseases of the aorta and its branch arteries, exclusive of the coronary arteries. In clinical practice, it specifically refers to atherosclerotic stenosis or occlusion of the arteries supplying the lower extremities, defined by an ankle-brachial index (ABI) < 0.9. It is the third leading cause of atherosclerotic morbidity worldwide after coronary artery disease and stroke.
Epidemiology
- Affects 12% of the U.S. adult population and nearly 20% of adults over 70 years
- Symptomatic PAD (claudication) affects >10 million Americans
- Prevalence: 1-2% in those <50 years, 5% in those aged 50-70, and 10% in those >70
- 1-3% of those >50 with PAD have Chronic Limb-Threatening Ischemia (CLTI)
Risk Factors
| Major Risk Factors | Additional Risk Factors |
|---|---|
| Age | Non-white ethnicity |
| Male sex | Elevated C-reactive protein |
| Smoking (4x increased risk) | Chronic renal insufficiency |
| Diabetes mellitus (3x increased risk) | Homocysteinaemia |
| Hypertension | Family history |
| Dyslipidaemia |
Smokers predominantly develop superficial femoral artery disease; diabetics more often develop tibial artery disease.
Pathophysiology
The underlying mechanism is atherosclerosis - progressive narrowing and occlusion of arterial walls by atheromatous plaques at specific anatomic sites. The most common pattern is short-segment total occlusion of the superficial femoral artery (SFA) in the Hunter canal. As stenosis worsens:
- Collateral circulation compensates (profunda femoris artery bypasses SFA occlusion)
- When collaterals are insufficient for exercise demands → claudication
- When insufficient even at rest → rest pain
- When tissue perfusion fails → ulceration/gangrene
Clinical Presentation & Classification
Fontaine / Rutherford Classification
| Fontaine Stage | Symptoms | ABI Range |
|---|---|---|
| I | Asymptomatic | < 0.9 but no symptoms |
| IIa | Mild claudication (>200 m) | 0.5 - 0.9 |
| IIb | Severe claudication (<200 m) | 0.5 - 0.9 |
| III | Ischaemic rest pain | 0.4 - 0.5 |
| IV | Ulceration or gangrene | < 0.4 |
Cardinal Symptom: Intermittent Claudication
- Cramping, aching, reproducible muscle pain on walking
- Consistently triggered at the same distance
- Rapidly relieved by rest (within minutes)
- Calf pain = SFA/popliteal disease; buttock/thigh pain = aortoiliac disease (Leriche syndrome)
Distinguishing True Claudication from Pseudoclaudication
| Feature | True Claudication | Spinal Stenosis (Pseudo) |
|---|---|---|
| Character | Cramping, tightness | Tingling, weakness |
| Induced by | Exercise only | Exercise or standing |
| Distance | Reproducible | Variable |
| Relief | Rapid rest | Requires sitting or position change |
| Pulses | Diminished | Normal |
Rest Pain (Stage III)
- Severe forefoot/metatarsal pain at rest
- Worse at night - patient hangs leg over bed for relief (gravity aids perfusion)
- Trophic changes: hair loss, nail thickening, muscle wasting, skin atrophy
Tissue Loss (Stage IV)
- Ischaemic ulcers (painful, punched-out, on toes/pressure points)
- Dry or wet gangrene
Diagnosis
1. Ankle-Brachial Index (ABI)
The single most useful diagnostic test:
| ABI Value | Interpretation |
|---|---|
| 1.0 - 1.4 | Normal |
| 0.91 - 0.99 | Borderline |
| < 0.9 | Abnormal (PAD) |
| 0.5 - 0.9 | Claudication range |
| 0.4 - 0.5 | Rest pain |
| < 0.4 | Tissue loss / critical ischaemia |
| > 1.4 | Non-compressible vessels (DM/CRI - medial calcinosis) |
In diabetics with calcified vessels, ABI is falsely elevated - use toe-brachial index instead (< 0.7 = abnormal; absolute toe pressure < 30-50 mmHg = severe ischaemia)
2. Segmental Pressure Measurements
- At upper thigh, lower thigh, upper calf, ankle, metatarsal levels
- A drop of >20 mmHg between adjacent levels indicates haemodynamically significant stenosis
3. Duplex Ultrasonography
- Combines B-mode imaging with Doppler velocity measurements
- Sensitivity/specificity >90% for detecting ≥50% stenosis
- First-line non-invasive imaging; can be used for operative planning
4. CTA and MRA
- Both provide 3D vascular reconstructions
- CTA: requires iodinated contrast + radiation; excellent for stent visualization
- MRA: uses gadolinium; no radiation; avoids metallic implant patients; may overestimate ostial lesions
- Both have largely replaced invasive angiography as initial mapping tools
5. Digital Subtraction Angiography (DSA)
- Remains the gold standard for pre-operative planning, especially for tibial/pedal targets
- Retrograde femoral approach from contralateral limb
- Allows immediate endovascular intervention in the same sitting
Management
A. Conservative / Medical Management (All Patients)
1. Risk Factor Modification (cornerstone):
- Smoking cessation: reduces progression, cardiovascular mortality, and amputation risk
- BP control: target <130/80 mmHg
- Lipid control: statin therapy - target LDL <70 mg/dL; statins also stabilise plaque and reduce vascular inflammation independently of lipid lowering
- Diabetes control: target HbA1c < 7%
- Weight reduction
2. Antiplatelet Therapy:
- Aspirin or clopidogrel - both reduce cardiovascular morbidity and mortality in PAD
- The COMPASS trial showed: aspirin + rivaroxaban 2.5 mg twice daily reduced Major Adverse Limb Events (MALE)
- The VOYAGER PAD trial: same combination reduced acute limb ischaemia, amputation, MI, stroke, and death after revascularisation
3. Exercise Therapy:
- Structured supervised walking programme is strongly evidence-based for claudication
- Patients instructed to "walk through" claudication pain, resting as needed
- Improves walking distance and quality of life
4. Pharmacotherapy:
- Cilostazol (phosphodiesterase inhibitor): improves walking distance and quality of life (modest evidence)
- Pentoxifylline: rheologic agent; earlier studies supported use but later evidence questioned benefit
B. Revascularisation - Indications
- Lifestyle-limiting claudication not responsive to 3-6 months of conservative treatment
- CLTI - rest pain or tissue loss (urgent indication)
Choosing Endovascular vs. Surgical Approach
The TASC classification guides this decision:
- TASC A lesions: Short stenoses/occlusions → primary endovascular treatment
- TASC B/C lesions: Individualised approach (endovascular vs. surgical based on anatomy and risk)
- TASC D lesions: Long complex occlusions → primary surgical bypass
The Global Vascular Guidelines (GVG) 2019 advocate a "whole-limb" approach using the WIfI classification (Wound, Ischaemia, foot Infection) and the Global Anatomic Staging System (GLASS).
C. Endovascular Treatment
- Performed under local anaesthesia
- Options include: percutaneous transluminal angioplasty (PTA), bare metal stenting, drug-eluting stents, drug-coated balloons
- Best for shorter, more proximal lesions
- Patency decreases with: more distal disease, multiple lesions, longer/more severe stenoses
D. Open Surgical Revascularisation
- Infrainguinal bypass is the signature vascular surgical procedure
- Conduit: autologous great saphenous vein is preferred (best patency); prosthetic (PTFE/Dacron) used when vein is unavailable
- Common bypasses: femoro-popliteal bypass, femoro-tibial bypass, femoro-pedal bypass
- Success is highly dependent on conduit quality and surgical technique
E. Hybrid Procedures
- Combined endovascular + open surgical approach
- Useful when disease is present at multiple levels
F. Amputation
- Indicated when limb is non-viable (irreversible ischaemia, extensive infection, or non-ambulatory patient)
- Primary amputation preferred over futile revascularisation in selected cases
Acute Limb Ischaemia (ALI) - Distinguished from Chronic PAD
Recognised by the 6 Ps: Pain, Pallor, Pulselessness, Paraesthesia, Paralysis, Perishing cold
| Category | Description | Management |
|---|---|---|
| I - Viable | Not immediately threatened | Anticoagulation + investigation |
| IIa - Marginally threatened | Salvageable if promptly treated | Urgent endovascular or surgical |
| IIb - Immediately threatened | Sensory + motor loss | Emergency surgery |
| III - Irreversible | Profound paralysis + anaesthesia | Primary amputation |
- Symptoms <14 days: endovascular thrombolysis (rtPA) preferred
- Symptoms >14 days: surgical thrombectomy/bypass preferred
Prognosis
- 70-80% of claudicants remain stable or improve with risk factor modification
- Only 5-10% progress to CLTI over their lifetime
- However, PAD is a marker of severe systemic atherosclerosis: 20% experience MI/stroke, and 10-15% die from cardiovascular causes within 5 years
- Annual mortality ~2-5%; annual limb loss ~1% in claudicants
Sources: Mulholland and Greenfield's Surgery, 7th ed. | Goldman-Cecil Medicine, International Edition
This is a shared conversation. Sign in to Orris to start your own chat.