Classification of pancreatic tumors radiology easily
Reading File
Finding Sources
Finding Sources
Searching the Web
pancreatic tumors classification radiology CT MRI features easy summary 2024
Finding Sources
Reading Web Page
https://radiopaedia.org/articles/pancreatic-neoplasms?lang=u…
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material. Let me compile the full answer with all the key radiology-oriented classification details.
Classification of Pancreatic Tumors - Radiology Made Easy
The big-picture split is solid vs. cystic, then you refine by vascular behavior on CT (hypo- vs. hypervascular) and cyst morphology (micro- vs. macrocystic, communicating vs. non-communicating duct). Here is the full framework.
Step 1 - The Master Split
PANCREATIC TUMORS
├── SOLID
│ ├── Hypovascular (most common)
│ │ ├── Pancreatic Ductal Adenocarcinoma (PDAC) ← 85% of all
│ │ └── Acinar Cell Carcinoma (ACC)
│ └── Hypervascular
│ └── Pancreatic Neuroendocrine Tumor (pNET)
│ (also: metastases from RCC, HCC, melanoma)
└── CYSTIC
├── Benign (almost always)
│ └── Serous Cystadenoma (SCA)
├── Premalignant / Mucinous
│ ├── Mucinous Cystic Neoplasm (MCN)
│ └── IPMN (main-duct / branch-duct / mixed)
└── Mixed Solid-Cystic
└── Solid Pseudopapillary Neoplasm (SPN)
SOLID TUMORS
1. Pancreatic Ductal Adenocarcinoma (PDAC) - 85%
| Feature | Finding |
|---|---|
| CT appearance | Hypodense/hypoattenuating mass - arterial AND portal venous phase (due to desmoplastic stroma = hypovascular) |
| Margins | Ill-defined, infiltrative |
| Location | 70% pancreatic head |
| Secondary signs | Pancreatic duct dilation ("double duct sign" = dilated CBD + PD), upstream pancreatic atrophy, vascular encasement (SMA, celiac, portal/SMV) |
| Modality of choice | Multiphasic CT (pancreatic protocol); MRI/MRCP for small tumors not visible on CT |
| Key sign | Double duct sign = dilated common bile duct + dilated pancreatic duct; strongly suggests head PDAC |
"Typical imaging features of pancreatic cancer on dynamic CT include a hypoattenuating mass compared with the adjacent pancreatic parenchyma in the late arterial and portal venous phases due to decreased vascularity within the tumoral tissue and desmoplastic stroma." - Current Surgical Therapy 14e
Resectability on CT (Varadhachary/Katz System):
- Resectable: no vascular contact, no distant mets
- Borderline resectable: <180° contact with SMA/CA, short segment SMV/PV involvement
- Unresectable: >180° SMA/celiac encasement, solid aortic contact, distant metastases
2. Pancreatic Neuroendocrine Tumors (pNETs)
| Feature | Finding |
|---|---|
| CT appearance | Hypervascular - bright arterial enhancement (opposite of PDAC) |
| Location | Any part; functional tumors tend to be small |
| Functional vs. non-functional | Functioning = insulinoma, gastrinoma, VIPoma, glucagonoma; Non-functioning = usually large at diagnosis |
| Insulinoma | Smallest, most common functional pNET; usually benign; intense arterial blush |
| Gastrinoma | May be in "gastrinoma triangle"; associated with MEN-1 |
| WHO 2017 Grade | G1 (Ki-67 <3%), G2 (3-20%), G3 (>20%), NEC (poorly diff.) |
CYSTIC TUMORS
Quick Memory Table
| Feature | SCA | MCN | IPMN | SPN |
|---|---|---|---|---|
| Who gets it | Older F (postmenopausal) | Perimenopausal F | Older M or F | Young F (<40) |
| Location | Anywhere | Body/tail | Head (main-duct); Anywhere (branch) | Body/tail |
| CT/MRI appearance | Microcystic honeycomb; central scar/calcification | Macro-cystic, unilocular/multilocular; NO duct communication | Duct dilation (main-duct) or "grape-like" cluster (branch) | Mixed solid + cystic; hemorrhagic |
| Malignant potential | None (nearly) | Yes (5-15%) | Yes (main > branch) | Low (15%) |
| Key differentiator | Honeycomb + low CEA | Ovarian stroma; elevated CEA; does NOT communicate with PD | Communicates with PD (MRCP key!) | Mixed solid/cystic in young woman |
| Management | Observe if <4 cm, asymptomatic | All resect (lifetime malignancy risk) | Main-duct: resect; Branch-duct: Fukuoka criteria | Resect (curative) |
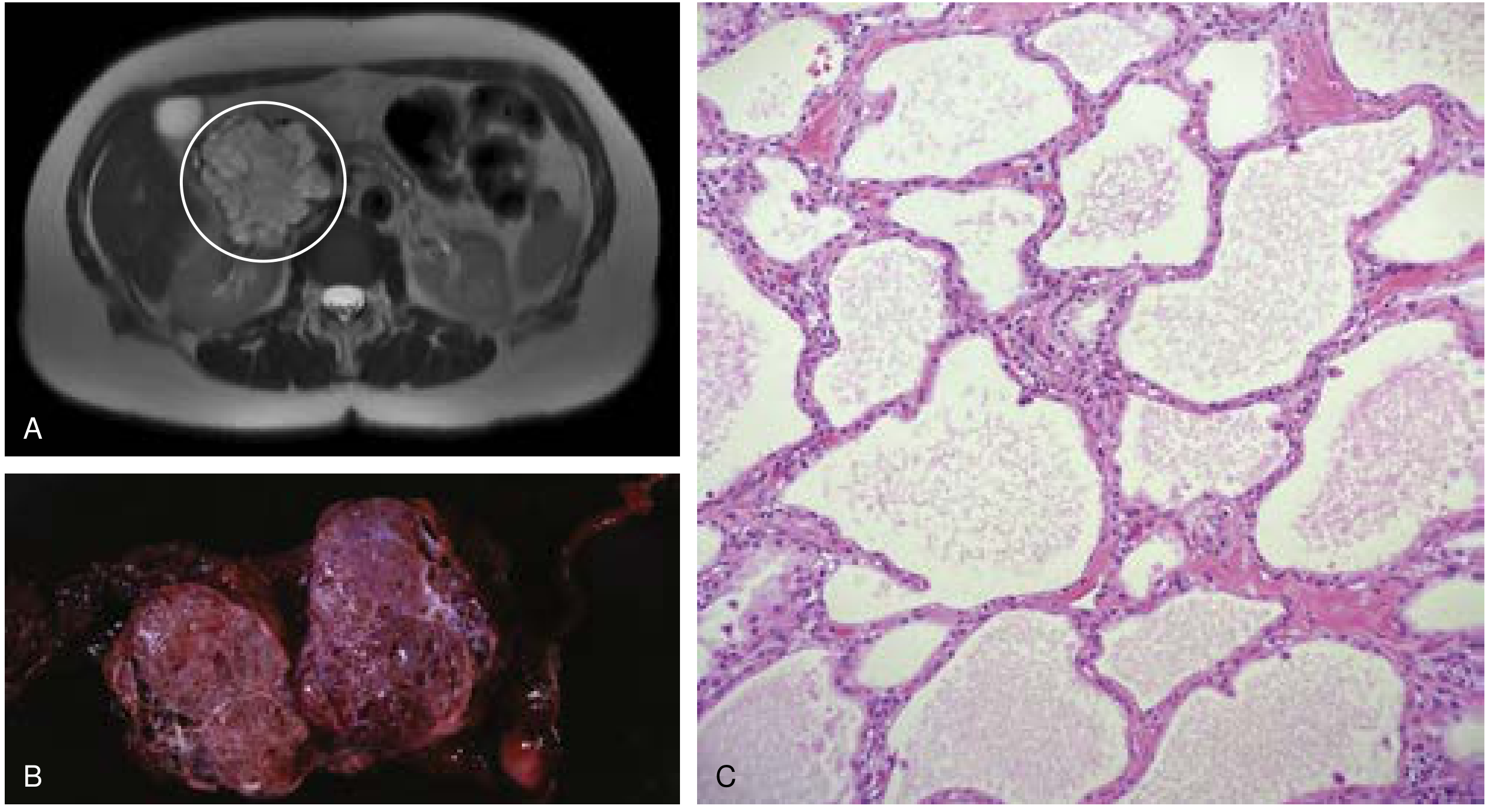
3. Serous Cystadenoma (SCA) - Benign
- Accounts for 33% of pancreatic cysts; almost universally benign
- CT/MRI: classic "honeycomb" or microcystic pattern (many tiny cysts <2 cm each) with a central stellate scar and sunburst calcification
- Fluid: very low CEA (<5 ng/mL) and low amylase - this is diagnostic
- Associated with Von Hippel-Lindau syndrome (lifetime risk ~40%)
4. Mucinous Cystic Neoplasm (MCN) - Premalignant
- 25% of pancreatic cysts; almost exclusively perimenopausal females
- Located in body/tail
- CT/MRI: well-encapsulated, unilocular or multilocular cyst; does NOT communicate with pancreatic duct (important!)
- Elevated CEA in cyst fluid; elevated CEA + low amylase = MCN
- Malignancy risk: 5-15%; red flags = mural nodule, solid component, calcifications, wall thickening
- Path hallmark: ovarian-type stroma underneath the epithelium (required for diagnosis)
5. IPMN (Intraductal Papillary Mucinous Neoplasm)
Three subtypes by location:
| Type | Imaging | Malignancy Risk | Action |
|---|---|---|---|
| Main-duct IPMN | Diffuse or segmental PD dilation (>5 mm) | High (60-70%) | Resect |
| Branch-duct IPMN | "Cluster of grapes" cysts; communicates with PD on MRCP | Lower (~25%) | Fukuoka guidelines (observe vs. resect) |
| Mixed | Both features | High | Resect |
- Key test: MRCP - shows communication between cyst and pancreatic duct (pathognomonic for IPMN vs. MCN)
- Worrisome features (Fukuoka): mural nodule, thickened/enhancing walls, PD 5-9 mm, abrupt PD caliber change
- High-risk stigmata: obstructive jaundice, enhancing mural nodule >5 mm, PD ≥10 mm - resect
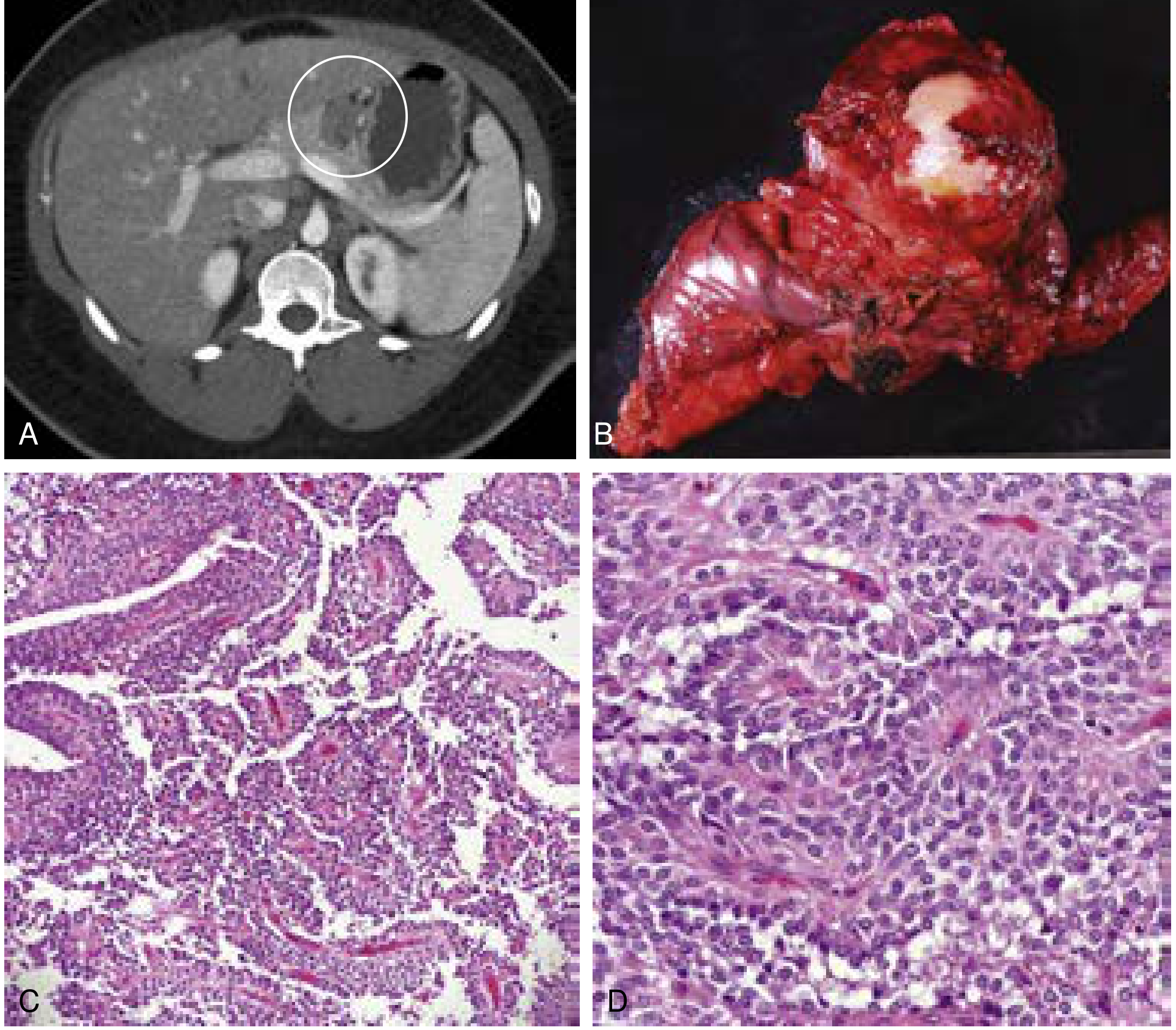
6. Solid Pseudopapillary Neoplasm (SPN) - Low Malignant Potential
- Young females (~20s-30s); rare (5% of resected cysts; 1% of all pancreatic tumors)
- CT: mixed solid + cystic mass; hypoenhancing; often hemorrhagic with fluid-fluid levels; well-circumscribed
- MRI: heterogeneous T1/T2 signal due to hemorrhage; fibrous capsule
- Pathognomonic: "floating debris" from internal hemorrhage and necrosis
- WNT/beta-catenin pathway mutations (90%)
- Management: resection is usually curative; ~4.4% recurrence rate
Rare Solid Tumors (Know for Completeness)
| Tumor | Key Radiology Clue |
|---|---|
| Acinar Cell Carcinoma (ACC) | Large exophytic solid mass; 1-2% of pancreatic tumors; males; can be cystic variant |
| Pancreatoblastoma (PBA) | Children; solid mass with calcifications; pancreatic head; elevated AFP; associated with Beckwith-Wiedemann |
| PEComa | Hypoenhancing mass, well-circumscribed; HMB-45 positive |
| Lymphoma | Bulky, homogeneous, hypovascular mass; no duct obstruction despite large size ("silent" obstruction) |
| Metastases | Most common from RCC (hypervascular), lung, melanoma; may be multiple |
The "Radiology First Look" Decision Tree
Is it CYSTIC or SOLID?
│
├── SOLID
│ └── Is it HYPERVASCULAR on arterial phase?
│ ├── YES → pNET (also consider RCC met)
│ └── NO (hypodense) → PDAC (most likely)
│
└── CYSTIC
├── Microcystic/honeycomb → SCA (benign, observe)
├── Macrocystic, body/tail, no duct comm., F only → MCN (resect all)
├── Communicates with pancreatic duct (MRCP) → IPMN
│ └── Main duct dilated? → High risk (resect)
│ └── Branch-duct? → Fukuoka criteria
└── Mixed solid/cystic, young woman → SPN (resect)
Key Imaging Protocols
- Pancreatic protocol CT: Non-contrast + arterial phase (35-40 s) + portal venous phase (70 s) + sometimes delayed. Arterial phase is key for hypervascular tumors (pNET) and for vascular involvement assessment
- MRI/MRCP: Best for cystic lesions, duct communication, and small tumors missed on CT
- EUS + FNA: For cyst fluid analysis (CEA, amylase, cytology) when CT/MRI are equivocal
Sources: Current Surgical Therapy 14e; Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Maingot's Abdominal Operations; Harrison's Principles of Internal Medicine 22E (2025)
This is a shared conversation. Sign in to Orris to start your own chat.