Local anaesthetics review
Reading File
Finding Sources
Finding Sources
Searching PubMed
"local anesthetics" AND pharmacology
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have a very comprehensive set of data. Let me compile the full review.
Local Anaesthetics - Complete Review
1. Chemical Structure
Local anaesthetics share a common three-part molecular structure:
- Lipophilic aromatic ring - provides membrane affinity
- Intermediate chain - either an ester (-C-O-) or amide (-NHC-) bond
- Hydrophilic tertiary amine - partially protonated at physiological pH
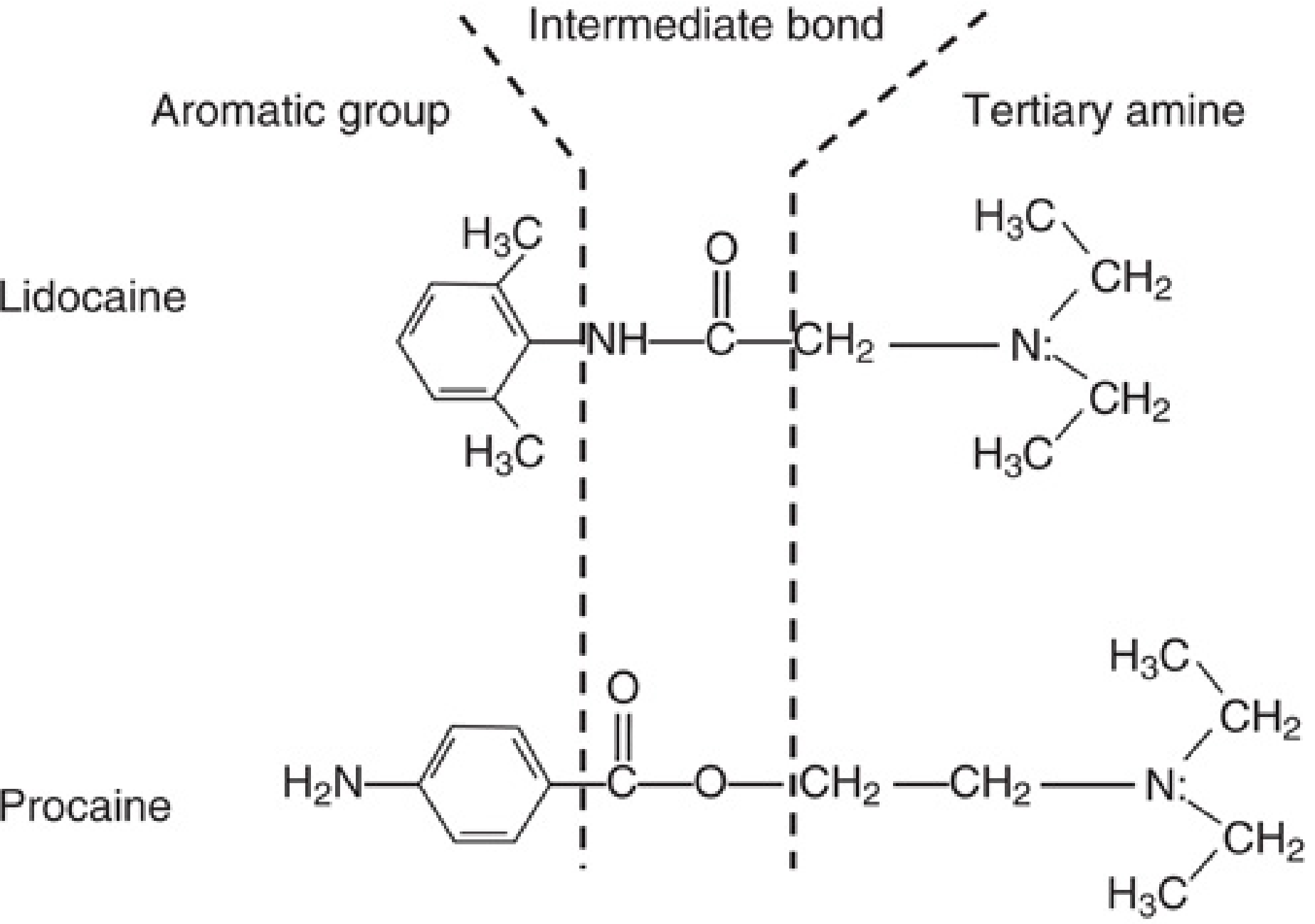
Fig. 25.1 from Miller's Anesthesia 10e: Lidocaine (aminoamide) and procaine (aminoester). The hydrophobic aromatic group is joined to the hydrophilic tertiary amine by the intermediate ester or amide bond.
Classification
| Class | Bond | Examples | Metabolism |
|---|---|---|---|
| Aminoesters | Ester (-COO-) | Cocaine, Procaine, Tetracaine, Chloroprocaine, Benzocaine | Plasma pseudocholinesterase; PABA metabolite (allergenic) |
| Aminoamides | Amide (-NHCO-) | Lidocaine, Bupivacaine, Ropivacaine, Levobupivacaine, Prilocaine, Mepivacaine | Hepatic microsomal enzymes |
Memory aid: Amides have two "i"s in their name (lidocaine, bupivaine, ropivacaine); esters have one or none.
2. Mechanism of Action
Local anaesthetics block voltage-gated Na+ channels, preventing the depolarisation phase of the action potential.
The pKa and Ionisation Concept
Local anaesthetics are weak bases formulated as hydrochloride salts. In tissue they exist in equilibrium between:
- Neutral base (B) - lipid-soluble, crosses the axonal membrane
- Charged cation (BH+) - binds the intracellular face of the Na+ channel and is the active blocking form
The Henderson-Hasselbalch equation governs this balance:
pH = pKa + log[B]/[BH+]
Clinical implication: In infected/inflamed tissue (lower pH), more drug is in the charged cation form, which cannot cross the membrane → local anaesthetics work poorly in acidic/infected tissue.
Adding sodium bicarbonate to a local anaesthetic solution raises pH, increases the neutral base fraction, accelerates diffusion across the membrane, and speeds onset.
Use-Dependent (Phasic) Block
Local anaesthetics show use-dependent block: the more frequently a nerve fires, the greater the degree of blockade. The drug preferentially binds the open or inactivated state of the Na+ channel. This is why rapidly firing nociceptive fibres are blocked preferentially at lower concentrations. - Miller's Anesthesia 10e, p. 3565
Where does the drug act?
- The uncharged base crosses the lipid membrane
- The charged cation acts from the cytoplasmic (intracellular) surface of the Na+ channel - this is the primary site of potency
- Benzocaine (permanently uncharged) is an exception: it works only in its neutral form, explaining its utility as a topical agent
3. Physicochemical Properties and Their Clinical Correlates
| Property | Clinical Effect |
|---|---|
| Higher lipid solubility (hydrophobicity) | Greater potency, longer duration |
| Lower pKa (closer to physiologic pH) | More neutral base at pH 7.4, faster onset |
| Higher protein binding | Longer duration of action |
| Vasodilatory effect | Increases systemic absorption; shorter duration (hence epinephrine is added) |
Key Drug Properties
| Drug | pKa | Onset | Duration | Notes |
|---|---|---|---|---|
| Lidocaine | 7.9 | Fast | Short-medium | Versatile; IV antiarrhythmic |
| Bupivacaine | 8.1 | Slow | Long | Cardiotoxic; sensory > motor |
| Ropivacaine | 8.1 | Slow | Long | Less cardiotoxic than bupivacaine; more sensory selectivity |
| Levobupivacaine | 8.1 | Slow | Long | S-enantiomer; less cardiotoxic |
| Prilocaine | 7.9 | Fast | Medium | Least systemic toxicity; causes methaemoglobinaemia |
| Mepivacaine | 7.6 | Fast | Medium | - |
| Chloroprocaine | 8.7 | Very fast | Very short | Ester; lowest systemic toxicity |
| Tetracaine | 8.5 | Slow | Long | Ester; spinal anaesthesia |
| Cocaine | 8.6 | Medium | Medium | Unique vasoconstrictor; ENT use only |
4. Nerve Fibre Susceptibility
| Fibre | Myelination | Diameter | Function | Sensitivity to LA |
|---|---|---|---|---|
| Aα | Heavy | Largest | Motor, proprioception | Most resistant |
| Aβ | Heavy | Large | Touch, pressure | Resistant |
| Aδ | Light | Small | Pain (sharp/fast), temperature | Sensitive |
| B | Light | Small | Preganglionic sympathetic | Very sensitive |
| C | None | Smallest | Pain (dull/slow), temp, postganglionic sympathetic | Sensitive |
Important nuance (Miller's 10e): Traditional teaching states that small C fibres are most susceptible, but careful single-fibre measurements show Aδ and B fibres are actually blocked before C fibres. The apparent clinical differential is better explained by length of nerve exposed (anatomical factors) and impulse frequency (use-dependent block), not simply fibre diameter alone.
Order of loss in epidural/spinal block:
- Sympathetic (vasodilation, temperature) - lost first
- Pain and temperature
- Touch and pressure
- Motor function - lost last
This is the basis for differential blockade - dilute epidural bupivacaine (0.0625-0.125%) can provide labour analgesia with minimal motor block.
5. Maximum Doses and Vasoconstrictor Additives
| Drug | Max Dose (plain) | Max Dose (with epinephrine) |
|---|---|---|
| Lidocaine | 3 mg/kg | 7 mg/kg |
| Bupivacaine | 2 mg/kg | 2 mg/kg (no increase) |
| Ropivacaine | 3-4 mg/kg | - |
| Prilocaine | 6 mg/kg | 9 mg/kg |
| Levobupivacaine | 2 mg/kg | - |
Bailey & Love's 28th Edition, Table 23.2
Epinephrine (Adrenaline) as Additive
- Causes local vasoconstriction → reduces vascular absorption → prolongs duration, lowers peak plasma concentration, raises safe dose limit
- Hastens onset
- Contraindicated in: end-arterial sites (digits, nose, penis, ears), patients with cardiovascular disease, those on MAOIs or tricyclic antidepressants
6. Techniques of Administration
| Technique | Description |
|---|---|
| Topical | Applied to mucous membranes or skin (EMLA, amethocaine gel); superficial effect only |
| Infiltration | Injected directly into tissue; duration doubled with epinephrine |
| Peripheral nerve block | Injection near specific nerve or plexus (e.g., brachial plexus, femoral nerve) |
| IV regional (Bier block) | Lidocaine into exsanguinated limb; requires double-cuff tourniquet |
| Epidural | Injection into epidural space; segmental block |
| Spinal (intrathecal) | Injection into CSF in subarachnoid space; rapid, dense block |
| Caudal | Epidural via sacral hiatus; paediatric and perineal surgery |
Ultrasound guidance has transformed regional anaesthesia: allows visualisation of nerve and LA spread, smaller effective volumes, fewer complications compared to landmark/nerve stimulator techniques. - Bailey & Love's 28th Edition
Site-Dependent Pharmacokinetics
Onset is fastest intrathecally (no sheath, drug immediately adjacent to cord). Brachial plexus blocks have the slowest onset because the drug must diffuse through perineural tissue. Duration is shortest intrathecally (small drug volume) and longest with brachial plexus blocks (slow vascular absorption, large drug volume, long exposed nerve segment). - Miller's Anesthesia 10e, p. 3585
7. Systemic Toxicity (LAST - Local Anaesthetic Systemic Toxicity)
LAST arises from dose-related sodium channel blockade in non-target tissues - primarily brain and heart. Most commonly due to inadvertent intravascular injection or excessive dosing. - Tintinalli's Emergency Medicine
Risk Reduction
- Aspirate before every injection
- Fractionated (incremental) dosing with repeated aspiration
- Epinephrine test dose (1:200,000 - tachycardia indicates intravascular injection)
- Use minimum effective dose and concentration
- Real-time ultrasound guidance
CNS Toxicity (occurs at lower plasma levels)
Progressive course:
- Perioral tingling, numbness of tongue, metallic taste
- Tinnitus, visual disturbance, dizziness
- Muscular twitching, tremors
- Tonic-clonic seizures
- CNS depression, respiratory arrest
Cardiovascular Toxicity (occurs at higher plasma levels)
- Prolonged PR interval, wide QRS
- Ventricular tachycardia / fibrillation
- Cardiac arrest
Bupivacaine is the most cardiotoxic because its high lipid solubility leads to prolonged Na+ channel binding ("fast in, slow out"). It causes refractory ventricular arrhythmias. This is why bupivacaine must never be used intravenously (no IV regional anaesthesia).
Ropivacaine and levobupivacaine are less cardiotoxic alternatives.
Treatment of LAST
- Stop injection immediately
- Airway management - 100% O2, ventilate, intubate if needed
- Seizures - benzodiazepines (e.g., midazolam); avoid propofol (cardiac depression) if haemodynamically compromised
- 20% Lipid emulsion therapy (Intralipid):
- Bolus: 1.5 mL/kg IV over 1 minute
- Infusion: 0.25 mL/kg/min for 10 minutes after haemodynamic stability
- If unstable: repeat bolus; maximum ~10 mL/kg over 30 minutes
- Mechanism: "lipid sink" - sequesters lipid-soluble drug away from myocardium
- Cardiac arrest - standard ACLS; avoid vasopressin; epinephrine in reduced doses; avoid lidocaine (further Na+ channel blockade)
- Consider cardiopulmonary bypass for refractory bupivacaine cardiac arrest
Tintinalli's Emergency Medicine; Miller's Anesthesia 10e
8. Specific Drug Toxicities
| Drug | Unique Toxicity |
|---|---|
| Bupivacaine | Most cardiotoxic; refractory ventricular arrhythmia; never IV |
| Prilocaine | Methaemoglobinaemia (metabolite o-toluidine oxidises Hb); treat with methylene blue 1-2 mg/kg IV |
| Cocaine | Sympathomimetic; vasoconstriction; dysrhythmias; abuse potential |
| Benzocaine | Methaemoglobinaemia (topical spray - particularly in airway procedures) |
| Tetracaine | Most toxic ester systemically; narrow therapeutic window |
| Chloroprocaine | Neurotoxicity if injected intrathecally in large volumes (due to bisulfite preservative, not drug itself) |
9. Allergy
- True allergy to amides is extremely rare (< 1% of reported "reactions")
- Esters metabolise to para-aminobenzoic acid (PABA) which is genuinely allergenic - cross-reactivity within ester class
- No cross-reactivity between ester and amide classes
- Most "allergic reactions" are vasovagal, epinephrine-related, or anxiety responses
- Methylparaben preservative (used in multi-dose amide vials) is a PABA derivative and can cause true allergy
10. Special Considerations
Pregnancy
- Epidural and spinal spread is greater in pregnancy (engorgement of epidural veins, reduced CSF volume, hormonal effects on nerve sensitivity)
- Lower doses are required
- LAST risks are amplified
Inflamed/Infected Tissue
- Reduced efficacy due to lower tissue pH (more ionised drug, less membrane penetration)
- Use higher volumes, add bicarbonate, or supplement with systemic analgesia
Mixtures
- Combining a fast-onset agent (lidocaine, chloroprocaine) with a long-acting agent (bupivacaine) is occasionally used for faster onset with prolonged block
- Toxicity is additive - do not use maximum doses of both
Carbonation / Alkalinisation
- Adding bicarbonate to lidocaine or bupivacaine increases base fraction, speeds onset
- Risk of precipitation with bupivacaine
- Less relevant with ultrasound guidance
11. Topical Agents Summary
| Agent | Composition | Use | Onset |
|---|---|---|---|
| EMLA | Lidocaine 2.5% + Prilocaine 2.5% | Intact skin (venepuncture, minor procedures) | 60 min under occlusion |
| Amethocaine (Ametop) gel | Tetracaine 4% | Intact skin | 30 min |
| LET gel | Lidocaine 4% + Epinephrine + Tetracaine | Open wounds/lacerations | 20-30 min |
| Cocaine | 4-10% | Nasal/ENT surgery | 2-5 min |
| Benzocaine spray | 20% | Mucosal surfaces | 15-30 sec |
| Viscous lidocaine | 2% | Airway topicalisation | 2-5 min |
Tintinalli's Emergency Medicine, Table 36-1
Key Sources
- Miller's Anesthesia, 10th Edition, Chapter 25 (Local Anaesthetic Molecule, Mechanism, Differential Block, Dosing)
- Bailey & Love's Short Practice of Surgery, 28th Edition, Chapter 23 (Clinical Table)
- Goodman & Gilman's Pharmacological Basis of Therapeutics (Topical, Infiltration)
- Tintinalli's Emergency Medicine (LAST Management, Topical Agents)
- Morgan & Mikhail's Clinical Anesthesiology, 7e (Differential Neural Blockade)
This is a shared conversation. Sign in to Orris to start your own chat.