Beta lactams
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive data to write a thorough answer. Let me compile everything.
Beta-Lactam Antibiotics
Beta-lactam antibiotics are the largest and most widely used class of antibiotics. They all share a four-membered beta-lactam ring as their core structural feature and share the same fundamental mechanism of action - inhibiting bacterial cell wall synthesis.
Chemistry and Structure
All beta-lactams contain the four-membered beta-lactam ring (ring B). The different classes fuse this ring with additional ring systems:
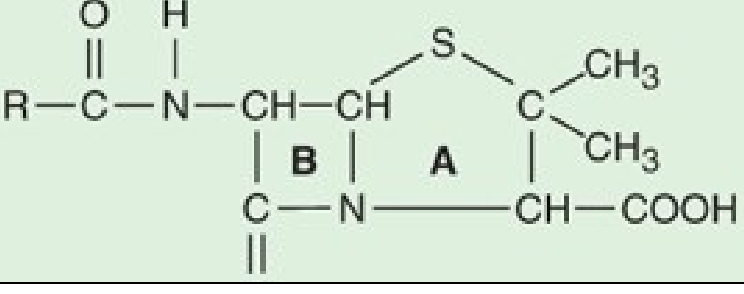
- Penicillins: beta-lactam ring + thiazolidine ring (5-membered sulfur ring). Variable R-group on the amino group creates the many different penicillins (Figure 43-1, Katzung 16e).
- Cephalosporins: beta-lactam ring + dihydrothiazine ring (6-membered ring). Derived from 7-aminocephalosporanic acid.
- Carbapenems: similar bicyclic structure but with a different stereochemical configuration in the lactam ring - this confers resistance to most common beta-lactamases.
- Monobactams: monocyclic beta-lactam ring only (no fused ring). Only aztreonam is available in the USA.
Structural integrity of the beta-lactam nucleus is essential for activity. Hydrolysis of the beta-lactam ring (by bacterial beta-lactamases) yields penicilloic acid, which lacks antibacterial activity.
Mechanism of Action
Beta-lactams inhibit bacterial growth by blocking the transpeptidation reaction in cell wall synthesis. Here is the sequence:
- The bacterial cell wall is made of peptidoglycan - a cross-linked polymer of alternating N-acetylglucosamine and N-acetylmuramic acid sugars, with pentapeptide side chains.
- Transpeptidase enzymes (also called penicillin-binding proteins, PBPs) normally remove the terminal d-alanine residue from the peptide side chain and form cross-links between adjacent chains - this cross-linking gives the wall its rigidity.
- Beta-lactams are structural analogs of the natural d-Ala-d-Ala substrate. They covalently bind to the active site of PBPs, irreversibly inhibiting the transpeptidation reaction.
- Peptidoglycan synthesis stops; bacterial autolysins continue degrading the wall and the cell dies.
Key point: Beta-lactams are bactericidal only against actively growing cells synthesizing new cell wall - they are ineffective against dormant or stationary-phase bacteria.
Classes of Beta-Lactams
1. Penicillins
| Subclass | Key Drugs | Spectrum / Notes |
|---|---|---|
| Natural penicillins | Penicillin G (IV), Penicillin V (oral) | Streptococci, meningococci, spirochetes, syphilis |
| Long-acting formulations | Benzathine penicillin, Procaine penicillin | IM; maintain levels for days-weeks; used for strep throat, syphilis |
| Antistaphylococcal | Nafcillin, Oxacillin, Dicloxacillin | Resistant to staphylococcal beta-lactamase; used for MSSA infections |
| Aminopenicillins | Ampicillin, Amoxicillin | Extended gram-negative coverage (E. coli, H. influenzae, Listeria) |
| Extended-spectrum | Piperacillin | Anti-pseudomonal activity; always used with tazobactam |
Pharmacokinetics of penicillins:
- Most are renally excreted (90% by tubular secretion); dose-adjust in renal failure.
- Normal half-life of penicillin G is ~30 minutes (up to 10 hours in renal failure).
- Food impairs absorption of most oral penicillins (amoxicillin is an exception).
- Penetration into CNS is poor normally, but adequate for meningitis treatment when inflamed meninges are present (with high IV doses).
- Nafcillin is cleared by bile, not kidneys - no dose adjustment needed in renal failure.
2. Cephalosporins (by generation)
1st generation (cefazolin IV, cephalexin PO):
- Good gram-positive (MSSA, streptococci), limited gram-negative.
- Used for: skin/soft tissue infections, UTI, surgical prophylaxis.
- Poor CNS penetration.
2nd generation (cefuroxime, cefoxitin, cefotetan):
- Improved gram-negative (H. influenzae, M. catarrhalis).
- Cefoxitin/cefotetan have anaerobic coverage (B. fragilis) - used for abdominal/pelvic infections, PID.
- Cefuroxime crosses blood-brain barrier but inferior to 3rd gen for meningitis.
3rd generation (ceftriaxone, cefotaxime, ceftazidime; oral: cefixime, cefpodoxime, cefdinir):
- Expanded gram-negative coverage including Citrobacter, Serratia, Providencia.
- Most penetrate CSF - used for meningitis.
- Ceftazidime is the only 3rd-gen agent with useful anti-Pseudomonas activity.
- Ceftriaxone: half-life 7-8 hours (once-daily dosing); used for pneumonia, meningitis, gonorrhea.
- Hydrolyzed by AmpC beta-lactamases; not reliably active against Enterobacter sp.
4th generation (cefepime):
- Extended gram-negative activity including Pseudomonas.
- Stable to AmpC beta-lactamases (can treat Enterobacter).
- Good gram-positive activity.
- Penetrates CSF; used for nosocomial pneumonia, febrile neutropenia.
5th generation (ceftaroline):
- Activity against MRSA (unique among cephalosporins).
- Used for community-acquired pneumonia, skin/soft tissue infections.
ESBL note: Strains of E. coli and Klebsiella expressing extended-spectrum beta-lactamases (ESBLs) can hydrolyze most cephalosporins - this is a growing clinical problem.
3. Carbapenems (imipenem, meropenem, ertapenem, doripenem)
- Broadest spectrum of all beta-lactams.
- Active against gram-positives, gram-negatives (including most Pseudomonas and Enterobacter), and anaerobes.
- Resistant to most beta-lactamases due to altered stereochemistry of the lactam ring.
- Imipenem is combined with cilastatin (a renal dehydropeptidase inhibitor) to prevent renal inactivation.
- Used for: severe hospital-acquired infections, polymicrobial infections, infections with ESBL-producing organisms.
- Carbapenemases (KPC, NDM, OXA-48 enzymes) represent the most serious resistance threat - can render organisms resistant to essentially all beta-lactams.
4. Monobactams (Aztreonam)
- Monocyclic beta-lactam; the only available agent.
- Spectrum limited to aerobic gram-negative bacteria only (including Pseudomonas) - no activity against gram-positives or anaerobes.
- Structurally similar to ceftazidime - potential cross-reactivity with ceftazidime allergy.
- Safe in penicillin-allergic patients (no cross-reactivity with penicillins).
- IV dosing: 1-2 g every 8 hours; penetrates CSF well.
- Half-life 1-2 hours; requires dose adjustment in renal failure.
5. Beta-Lactamase Inhibitors (BLIs)
BLIs are not antibiotics themselves (weak intrinsic activity), but they protect their partner beta-lactam from enzymatic destruction. They are always given in combination.
| Inhibitor | Type | Partner Drug | Coverage |
|---|---|---|---|
| Clavulanic acid | Traditional (Ambler class A) | Amoxicillin, ticarcillin | Class A beta-lactamases |
| Sulbactam | Traditional (class A) | Ampicillin | Class A; also direct Acinetobacter activity |
| Tazobactam | Traditional (class A) | Piperacillin | Class A; broader than clavulanate |
| Avibactam | Novel (non-beta-lactam) | Ceftazidime | Class A, C, and some class D (OXA-48) |
| Vaborbactam | Novel (non-beta-lactam) | Meropenem | Class A and C (including KPC) |
| Relebactam | Novel | Imipenem-cilastatin | Similar to avibactam |
Traditional BLIs are not effective against class C AmpC beta-lactamases produced by Enterobacter, Citrobacter, Serratia, and Pseudomonas.
Mechanisms of Resistance
Three main mechanisms (Goodman & Gilman; Katzung 16e):
-
Alteration of PBP target - reduced affinity for beta-lactams:
- MRSA acquires an additional low-affinity PBP (PBP2a, encoded by mecA) via a transposon - conferring resistance to all beta-lactams.
- Penicillin-resistant pneumococci have altered PBPs via interspecies homologous recombination.
-
Reduced concentration at the target site:
- Porin loss in gram-negative bacteria - reduced outer membrane permeability.
- Efflux pumps - actively remove the drug before it can act.
- When porin loss + efflux combine with beta-lactamase production = high-level resistance.
-
Enzymatic degradation - beta-lactamases:
- The most common and clinically important mechanism.
- Gram-positive bacteria: secrete large amounts of narrow-spectrum penicillinase (encoded on plasmids; transferable by bacteriophage).
- Gram-negative bacteria: beta-lactamases in the periplasmic space provide maximal protection.
- ESBL (extended-spectrum beta-lactamases): hydrolize most penicillins AND cephalosporins.
- Carbapenemases (KPC, NDM, OXA-48): hydrolize carbapenems too - organisms carrying these may resist virtually all beta-lactams in clinical use.
Adverse Effects
Hypersensitivity (most important)
- ~5-8% of patients report penicillin allergy, but only a small fraction have true type I hypersensitivity.
- Antigenic determinants: degradation products (penicilloic acid and alkaline hydrolysis products) bound to host proteins.
- Anaphylaxis: very rare (0.05% of recipients) but potentially fatal.
- Serum sickness: urticaria, fever, joint swelling, angioedema, occurs 7-12 days after exposure (now rare).
- Skin rashes, eosinophilia, interstitial nephritis, hemolytic anemia, vasculitis.
- Skin testing for type I hypersensitivity: negative result allows safe re-administration in most patients.
- Desensitization possible when penicillin is absolutely needed (e.g., enterococcal endocarditis, neurosyphilis).
Cephalosporin cross-reactivity
- Risk of cross-reactivity with penicillins is low (historically overestimated at ~10%; actual rate ~1-2%).
- Highest risk when the R1 side chain is identical (e.g., amoxicillin-cefadroxil, ampicillin-cefaclor).
- Aztreonam has NO cross-reactivity with penicillins but does cross-react with ceftazidime (shared R1 side chain).
Other toxicities
- Seizures: high-dose IV penicillin in renal failure.
- Nafcillin: neutropenia, interstitial nephritis.
- Oxacillin: hepatitis.
- Ampicillin/amoxicillin: maculopapular rash (especially with concurrent EBV infection).
- Piperacillin-tazobactam + vancomycin: increased risk of acute kidney injury vs. other beta-lactams combined with vancomycin.
- C. difficile colitis: all antibiotics including beta-lactams can predispose.
- Secondary candidiasis: oropharyngeal and vaginal thrush.
PK/PD Principle
Beta-lactams exhibit time-dependent killing - bactericidal effect depends on the time the free drug concentration remains above the MIC (%T>MIC), NOT on peak concentration. This drives dosing strategies such as extended infusions of carbapenems and piperacillin-tazobactam in critically ill patients.
Quick Clinical Reference
| Indication | Preferred Beta-Lactam |
|---|---|
| Strep throat, syphilis | Penicillin G / benzathine penicillin |
| MSSA skin/soft tissue | Dicloxacillin (oral), nafcillin/oxacillin (IV) |
| MRSA | None (beta-lactams ineffective; use vancomycin, linezolid) - except ceftaroline |
| Community-acquired pneumonia | Amoxicillin-clavulanate or ceftriaxone + macrolide |
| Bacterial meningitis | Ceftriaxone (cefotaxime for neonates) |
| Pseudomonal infections | Piperacillin-tazobactam, cefepime, ceftazidime, carbapenems |
| Intra-abdominal/pelvic | Piperacillin-tazobactam, ertapenem; cefoxitin/cefotetan for mild |
| ESBL-producing organisms | Carbapenems |
| KPC carbapenemase organisms | Ceftazidime-avibactam, meropenem-vaborbactam |
| Penicillin allergy (gram-neg) | Aztreonam (safe in PCN allergy) |
| Surgical prophylaxis | Cefazolin |
Sources: Katzung's Basic and Clinical Pharmacology 16e, Ch. 43; Goodman & Gilman's Pharmacological Basis of Therapeutics, Ch. 58
This is a shared conversation. Sign in to Orris to start your own chat.