BED SORE CLASSIFICATION MANAGEMENT IN PARAPLEGIA PATIENT 5+5 MARKS MS ORTHO THEORY STRUCTED ANSWER
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pressure ulcer" OR "pressure injury" classification management spinal cord injury
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information. Let me compose the full structured MS Ortho answer.
BED SORE (PRESSURE ULCER) - CLASSIFICATION & MANAGEMENT IN PARAPLEGIA
MS Orthopaedics Structured Answer | 5+5 Marks
PART 1 - CLASSIFICATION (5 Marks)
Definition
A pressure sore (decubitus ulcer / bedsore / pressure injury) is tissue necrosis caused by sustained pressure, shear forces, friction, or moisture over a bony prominence, leading to ischemia and cell death. Paraplegia dramatically increases risk due to immobility, loss of sensation, neurogenic bladder/bowel, and muscle wasting.
Pathophysiology (Brief)
Prolonged pressure over a bony prominence → occlusion of blood vessels and lymphatics → ischemia → endothelial swelling → plasma leak into interstitium → inflammatory cell accumulation → tissue necrosis. The four contributing forces are:
- Pressure (primary) - >32 mmHg for >2 hours causes irreversible ischemia
- Shear forces - when patient slides down in bed, deeper tissues torn from superficial layers
- Friction - abrasion of superficial skin
- Moisture - maceration from urine/sweat (incontinence increases risk ×5)
NPUAP/EPUAP Classification (4-Stage System + 2 Additional Categories)
| Stage | Description | Clinical Appearance |
|---|---|---|
| Stage I | Non-blanchable erythema of intact skin | Skin intact; localized redness that does not blanch on pressure; may be warm, indurated |
| Stage II | Partial-thickness skin loss involving epidermis ± dermis | Shallow open ulcer with red/pink wound bed; may appear as intact or ruptured serum-filled blister |
| Stage III | Full-thickness tissue loss extending to deep fascia; subcutaneous tissue visible | Deep crater; may show undermining/tunneling; bone, tendon, muscle NOT exposed |
| Stage IV | Full-thickness tissue loss with exposed bone, tendon, or muscle | Eschar or slough often present; often shows undermining and sinus tracts |
Additional NPUAP 2016 categories:
- Unstageable: Full-thickness loss; base covered by slough/eschar - true depth unknown until debrided
- Deep Tissue Pressure Injury (DTPI): Persistent non-blanchable, deep red/maroon/purple discoloration of intact skin - indicates underlying muscle injury (important in spinal cord injury patients where sensation is absent)
Common Sites in Paraplegia (in order of frequency)
- Sacrum (most common - ~30%)
- Ischial tuberosities (especially wheelchair-bound patients)
- Greater trochanter
- Heels / calcaneum
- Lateral malleolus, medial condyle of tibia
Risk Assessment Tools
- Braden Scale - scores 6 domains: sensory perception, moisture, activity, mobility, nutrition, friction/shear (score ≤18 = at risk; ≤9 = very high risk - paraplegics almost always score ≤9)
- Norton Scale - physical/mental condition, activity, mobility, incontinence
PART 2 - MANAGEMENT (5 Marks)
Principles of Management (DIMES Framework)
Debridement | Infection control | Moisture balance | Edge/wound care | Surgery when needed
A. General/Preventive Measures
- Repositioning every 2 hours - alternating supine, 30-degree lateral tilt positions to offload bony prominences
- Pressure-relieving devices:
- Static/alternating air mattresses, gel mattresses, water mattresses (superior efficacy proven)
- Specialized wheelchair cushions for ischial ulcers
- Air-fluidized beds and low-air-loss beds for Stage III/IV
- Avoid: sheepskins, 2-inch foam pads (insufficient pressure reduction)
- Nutritional optimisation:
- High protein diet (1.25-1.5 g/kg/day)
- Vitamin C supplementation (84% reduction in ulcer area shown)
- Correct hypoalbuminemia (target serum albumin >3.5 g/dL)
- Zinc, iron supplementation
- Skin care: Keep skin clean and dry; avoid incontinence contact; avoid therapeutic massage of at-risk areas (causes tissue degeneration); use moisture barriers
- Multidisciplinary team approach - significant reduction in incidence demonstrated
B. Local Wound Care (by Stage)
| Stage | Local Treatment |
|---|---|
| Stage I | Transparent film dressing; relieve pressure; protect area |
| Stage II | Foam island dressing; hydrocolloid dressing; transparent film; maintain moist environment |
| Stage III | Saline-soaked gauze dressings (wet-to-dry); hydrocolloid for exudative wounds; alginates for heavy drainage; debridement |
| Stage IV | Saline-soaked gauze; aggressive debridement; rule out osteomyelitis; consider surgical reconstruction |
Wound Cleansing: Normal saline is agent of choice. Avoid povidone-iodine, hypochlorite, acetic acid, hydrogen peroxide - all inhibit wound healing.
C. Debridement Methods
- Surgical debridement - sharp excision; indicated for infected necrotic tissue threatening septicaemia
- Mechanical debridement - wet-to-dry saline dressings
- Enzymatic debridement - topical collagenase; used until wound bed is clean
- Autolytic debridement - synthetic occlusive dressings allow self-digestion by wound enzymes
- Biosurgery (maggot therapy) - larvae selectively debride necrotic tissue; option for patients unfit for surgery
D. Infection Control / Antibiotic Therapy
Pressure sore infections are polymicrobial - Pseudomonas aeruginosa, Providencia spp., Proteus spp., S. aureus, Bacteroides fragilis are the most common organisms.
| Severity | Antibiotic Regimen | Duration |
|---|---|---|
| Mild | Cephalexin, or Amoxicillin/clavulanate, or Clindamycin + Ciprofloxacin | 2 weeks |
| Moderate | Clindamycin + Ciprofloxacin, or Ceftriaxone IV, or Vancomycin (MRSA) | 2-4 weeks |
| Severe / Osteomyelitis | Piperacillin/Tazobactam, or Imipenem/Meropenem, or Clindamycin + Gentamicin IV | 2-12 weeks |
E. Surgical Management
Indications: Stage III/IV non-healing ulcers, exposed bone, osteomyelitis, or ulcers not responding to conservative care.
Steps:
- Excision of ulcer and underlying bursae
- Excision of underlying bony prominence (ischiectomy/trochanteric reduction) to reduce recurrence
- Debridement of osteomyelitic bone if present
- Flap reconstruction - the definitive surgical option
Common Flap Choices in Paraplegia:
| Ulcer Site | Preferred Flap |
|---|---|
| Sacral | Gluteus maximus myocutaneous flap |
| Ischial | Posterior thigh (hamstring) advancement flap; gracilis flap |
| Trochanteric | Tensor fascia lata (TFL) myocutaneous flap |
Note: In paraplegics, muscle flaps are preferred as the denervated muscle provides well-vascularised tissue bulk; sensation is already lost so a sensate flap is not mandatory.
F. Complications to Watch For
- Septicaemia - most serious and common complication; in-hospital mortality 23-36%
- Osteomyelitis - diagnose with MRI/bone biopsy; prolonged antibiotic therapy required
- Cellulitis / necrotising fasciitis
- Amyloidosis - secondary (AA) amyloidosis from chronic infection
- Squamous cell carcinoma (Marjolin's ulcer) - rare malignant change in chronic non-healing ulcers
- Autonomic dysreflexia - triggered by wound pain in high-level spinal cord injury patients; can be life-threatening
Summary Table
| Component | Key Point |
|---|---|
| Classification | 4 NPUAP stages + Unstageable + DTPI |
| Most common site | Sacrum; ischium in wheelchair users |
| Primary cause | Pressure + shear + moisture + friction |
| Prevention | 2-hourly repositioning + pressure-relieving mattress |
| Wound cleaning | Normal saline only |
| Stage I/II dressing | Transparent film / hydrocolloid |
| Stage III/IV dressing | Saline-soaked gauze + debridement |
| Surgical reconstruction | Myocutaneous flaps based on site |
| Antibiotic combination | Clindamycin + Gentamicin (severe) |
| Most serious complication | Septicaemia |
Source: Swanson's Family Medicine Review, 10e; Geriatric Review Syllabus (American Geriatrics Society, 2019); NPUAP/EPUAP Pressure Injury Classification System
TENDON SUTURING TECHNIQUES PRINCIPLES OF TENDON TRANSFER
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive data from Campbell's Operative Orthopaedics 2026 and Roberts & Hedges. Let me compose the full structured MS Ortho answer.
TENDON SUTURING TECHNIQUES & PRINCIPLES OF TENDON TRANSFER
MS Orthopaedics Structured Answer
PART 1 - TENDON SUTURING TECHNIQUES
A. General Principles of Tendon Repair
Before choosing a suture technique, certain principles apply universally:
- Atraumatic handling - minimise crush injury to tendon ends; use sharp instruments
- Adequate exposure - Brunner zigzag / Bruner incisions to visualise the repair site
- Tension-free coaptation - ends should be brought together without bunching or gapping
- Preserve blood supply - avoid excessive dissection around the vincular system
- Preserve annular pulleys - at minimum A2 and A4 must be maintained to prevent bowstringing
- Strong repair permitting early mobilisation - four or more strand core sutures allow early active motion, reducing adhesion formation
B. Suture Material
- Core suture: Non-absorbable suture (3-0 or 4-0 Ethibond / Prolene / Nylon)
- Peripheral/epitendinous suture: 5-0 or 6-0 non-absorbable (Prolene/nylon)
- The epitendinous suture contributes up to 50% of load-to-failure strength and reduces bulk at the repair site, minimising triggering
C. Timing of Repair
| Type | Timing |
|---|---|
| Primary repair | Within 12 hours (clean wounds); up to 24 hours |
| Delayed primary | 24 hours to ~10 days |
| Secondary repair | 10 days to ~4 weeks |
| Late secondary repair | After 4 weeks (often needs tendon graft) |
Primary repair is indicated for clean lacerations. Secondary repair is chosen when complicated by crushing, bony comminution, severe neurovascular or joint injury, or skin loss requiring flap/graft coverage.
D. Flexor Tendon Zones (Bunnell's Classification)
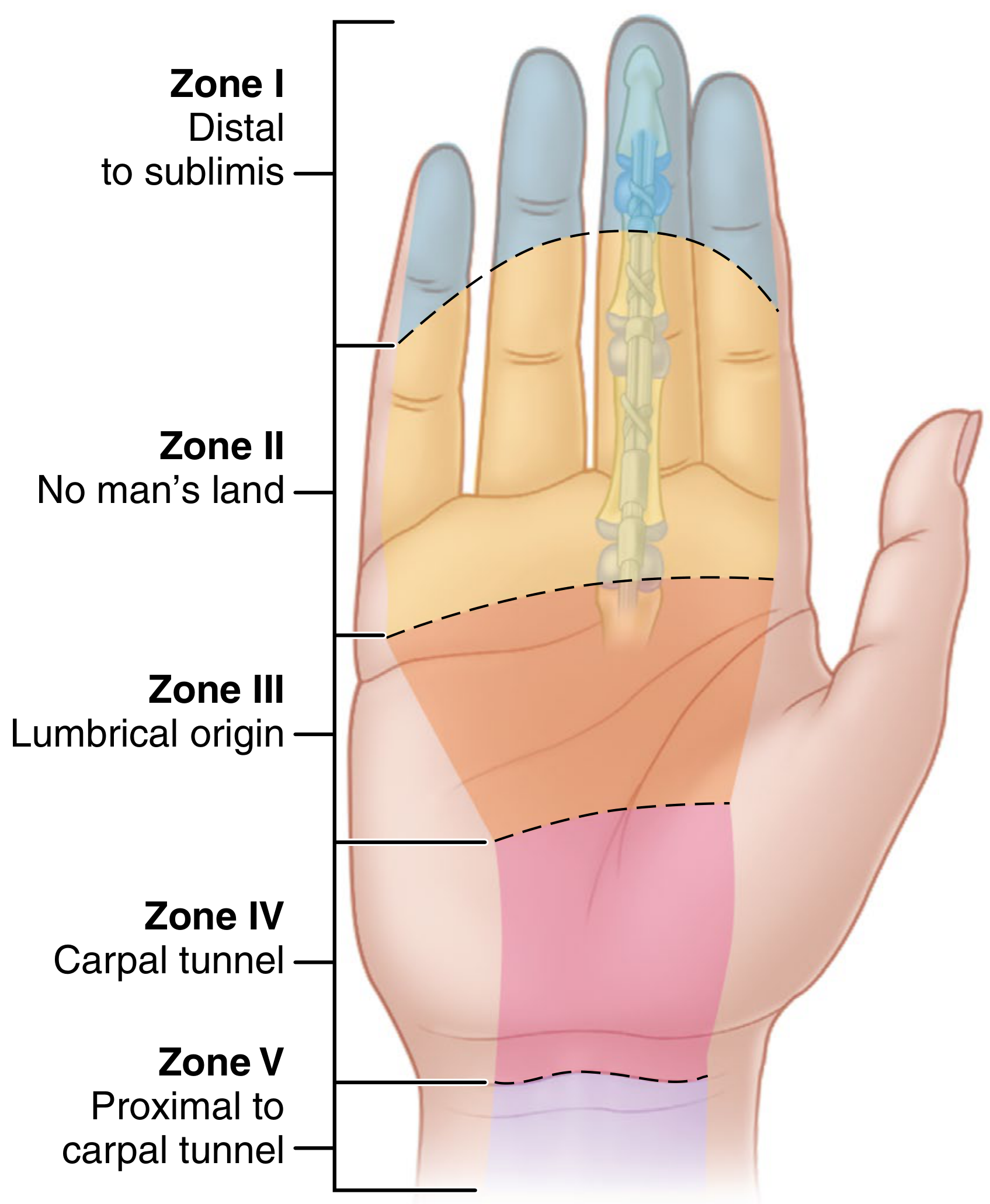
| Zone | Location | Notes |
|---|---|---|
| Zone I | Distal to FDS insertion → FDP insertion | FDP only; repair or advancement |
| Zone II | Distal palmar crease → FDS insertion | "No man's land" (Bunnell); most challenging; both tendons in fibro-osseous sheath |
| Zone III | Distal edge of carpal tunnel → Zone II | Lumbrical origin area |
| Zone IV | Under transverse carpal ligament | Carpal tunnel |
| Zone V | Proximal to carpal tunnel in forearm | Prognosis best |
E. Core Suture Techniques
1. Bunnell Stitch (Historical - now less preferred)
- Crisscross (zigzag) pattern through tendon substance
- Problem: Jeopardises intratendinous vascularity; strangulates tendon fibres; increased adhesion risk
- Two-strand repair - inadequate strength for early active motion
2. Kessler / Modified Kessler (Tajima) Stitch - Most Widely Used
- Needle enters the cut end of the tendon and exits laterally
- Suture runs longitudinally, then crosses transversely across the cut surface
- Modified Kessler (Tajima) adds a grasping loop at each lateral exit, locking tendon fibres
- Two-strand repair - forms the basis of multi-strand adaptations
- Single knot buried at the repair site
3. Four-Strand Techniques
- Lee technique: Two separate Kessler-type sutures placed 90° apart = four strands cross the repair
- Modified Tsuge: Loop suture looped through each half with a transverse bite; four strands
- Chung (Modified Tsuge): Loop inserted laterally into proximal tendon, run longitudinally across repair, transverse bite in distal half - creates four to six strands
- Advantage: Significantly stronger than two-strand; allows early active mobilisation; reduces gap formation
4. Six-Strand Techniques
- Savage / Adelaide Technique: Three grasping stitches placed sequentially in each tendon end using 4-0 Ethibond, giving six strands crossing the repair
- Grasping stitches placed 5-10 mm from cut end, avoiding the vincular area
- Strongest configuration for active motion protocols
5. Eight-Strand Repairs
- Further modifications of the Savage technique
- Provide maximum tensile strength but technically demanding in the narrow sheath of Zone II
Summary of Strand Strength
| Technique | Strands | Relative Strength | Suitable for |
|---|---|---|---|
| Bunnell | 2 | Low | Historical only |
| Modified Kessler | 2 | Moderate | Immobilisation protocols |
| Four-strand (Lee, Tsuge) | 4 | High | Early passive/active motion |
| Savage/Adelaide | 6 | Very high | Active motion protocols |
| Eight-strand | 8 | Highest | Selected cases |
F. Epitendinous (Peripheral) Suture - Mandatory Addition
- Placed circumferentially around the repair site after core suture
- Suture material: 5-0 or 6-0 Prolene/nylon
- Functions:
- Smooths the repair site, reducing bulk (prevents triggering on pulley)
- Adds ~50% of total load-to-failure strength
- Resists gap formation significantly
- The epitendon-first technique (placing peripheral suture before core suture) has been shown to be 22% stronger than modified Kessler alone
- Types: running horizontal mattress, interlocking mattress (highest load-to-failure), running cross-stitch
G. Extensor Tendon Repair
- Zone 6 (dorsum of hand): Modified Kessler, modified Bunnell, Augmented Becker (MGH technique), or Krackow-Thomas
- MGH (augmented Becker) technique showed superior resistance to gap formation compared to Krackow-Thomas and four-strand Bunnell in cadaveric studies
- Flat, thin extensor tendons in distal zones (I-III) repaired with figure-of-eight or horizontal mattress sutures
- Juncturae tendinum may mask complete tendon division - thorough wound exploration under tourniquet is essential
H. Special Situations
| Situation | Technique |
|---|---|
| FDP avulsion (Jersey finger) | Suture anchor repair in distal phalanx (placed dorsal-volar at 45° for maximum pull-out strength) |
| Partial laceration >60% | Repair as for complete; repairs <60% may be monitored if no triggering |
| Neglected rupture | Tendon graft (e.g., plantaris/palmaris longus) or tendon transfer (FHL for Achilles) |
| Contaminated wound | Delayed primary or secondary repair |
PART 2 - PRINCIPLES OF TENDON TRANSFER
(Source: Campbell's Operative Orthopaedics 15e 2026, Chapter 76)
Definition
A tendon transfer is the rerouting of a musculotendinous unit from its original insertion to a new insertion to restore a lost motor function caused by nerve injury, paralysis, or muscle loss.
Campbell's Key Principles (Mnemonic: "ESSEE" or the 7 Principles)
1. EXPENDABILITY
- The donor muscle must be expendable - its transfer must not create an equal or worse deficit
- Restoring finger extension is contraindicated if it sacrifices finger flexion
- Example: Extensor carpi radialis longus (ECRL) is more expendable than ECRB because ECRB is the primary wrist extensor
2. STRENGTH / MUSCLE POWER
- Muscle power graded 0-5 (MRC scale):
- 0 = No contraction; 1 = Trace; 2 = Active movement without gravity; 3 = Against gravity; 4 = Against gravity and resistance; 5 = Normal
- Donor muscle must be grade 4 or 5 (good to normal)
- A muscle loses one grade of power on transfer - therefore a grade 3 muscle will be useless post-transfer
- Transfer muscle must have adequate physiological cross-sectional area (force = 3.65 × cm² of cross-section)
3. SOFT TISSUE EQUILIBRIUM (Tissue Bed)
- The recipient bed must be pliable, well-vascularised, and free from active infection
- Scarred or fibrotic tissue bed prevents tendon gliding and leads to adhesion formation
- Timing: Transfer is best performed after favorable soft-tissue conditions have been achieved (no swelling, no severe scarring)
- The transferred tendon should be routed subcutaneously whenever possible; passing through tunnels without adequate openings leads to failure
4. SUPPLE JOINTS / PASSIVE RANGE OF MOTION
- Transferred tendon cannot overcome a fixed joint contracture
- Pre-operative requirement: full passive range of motion of all joints across which the transfer will act
- Serial splinting, physiotherapy, or joint releases must precede the transfer if contracture is present
5. EXCURSION / AMPLITUDE
- The tendon must have sufficient amplitude to produce functional joint motion
- Amplitude of common tendons (Curtis):
| Tendon | Amplitude (mm) |
|---|---|
| Wrist tendons | 33 |
| Flexor digitorum profundus | 70 |
| Flexor digitorum superficialis | 64 |
| Extensor digitorum communis | 50 |
| Flexor pollicis longus | 52 |
| Extensor pollicis longus | 58 |
- Rule of amplitude matching: Transferred tendon amplitude should ideally approximate that of the tendon it replaces
- Amplitude can be augmented by freeing the muscle proximal to its fibrous origin ("amplitude gain")
- The brachioradialis has limited amplitude (short excursion) but can still be useful for selected transfers (e.g., FPL restoration)
6. INTEGRITY / ONE FUNCTION PER TRANSFER
- Each transferred tendon should perform only one function
- When a tendon is split and attached to two points, the muscle acts primarily on the slip under greatest tension - equalising tension at attachment is critical
- Multiple functions overload the donor and compromise the result
7. SYNERGY
- Synergistic muscles are those that normally function together in a coordinated movement pattern
- Example: Wrist flexors and finger extensors act synergistically (wrist flexion automatically extends fingers)
- Transferring a synergistic muscle is technically easier to rehabilitate - the patient can re-educate the transfer more naturally
- Non-synergistic transfers require intensive motor re-education but can still succeed with training
Planning a Tendon Transfer
Step-by-step assessment:
- Identify function lost - list the absent motor functions
- Identify available donors - list expendable muscles with adequate strength and amplitude
- Match functions to donors - create a table pairing deficits with available muscles
- Ensure soft-tissue readiness - joints supple, wound healed, oedema resolved
- Select synergistic donors where possible
- Route selection - direct (in-line) routing is preferred; subcutaneous tunnels preferred over intermuscular
Common Tendon Transfers (Examples)
| Paralysis | Function Lost | Common Transfer |
|---|---|---|
| Radial nerve | Wrist/finger extension | FCU or ECRL → EDC (Boyes); PT → ECRB |
| Median nerve | Thumb opposition | FDS ring finger → APB (Bunnell); EIP → APB; ADM (Huber) |
| Ulnar nerve | Finger abduction / intrinsic function | FDS → lateral band (Zancolli lasso for claw) |
| Combined | Gross hand function | Multiple staged transfers |
| Cerebral palsy | Thumb-in-palm | BR → APL/EPB; FCU → ECRB |
Fixation of Transferred Tendon
- Weave-and-sew (Pulvertaft weave) - most common; donor woven through recipient 3-4 times and sutured
- End-to-end anastomosis - when tendons are similar calibre
- Bony attachment - suture anchor or pull-through technique to bone
- Tension setting: Set tension with the wrist and joints in the position that will produce the best functional balance - typically slightly overtightened as some stretch occurs during rehabilitation
Post-Operative Rehabilitation
- Immobilisation phase: 3-4 weeks in protective splint
- Re-education phase: Active motor re-education with physiotherapy starting at 4-6 weeks
- Synergistic transfers can be re-educated more rapidly
- Biofeedback and electrical stimulation may assist re-education of non-synergistic transfers
- Full rehabilitation: 3-6 months
Summary Table
| Principle | Minimum Requirement |
|---|---|
| Expendability | No equal or greater deficit created |
| Strength | MRC grade 4 or 5 |
| Soft tissue | Pliable, infection-free, good vascularity |
| Joints | Full passive ROM pre-operatively |
| Amplitude | Sufficient to produce functional excursion |
| Integrity | One transfer = one function |
| Synergy | Synergistic preferred; re-education easier |
Source: Campbell's Operative Orthopaedics 15th Edition 2026 (Chapter 71 - Flexor Tendon Repair; Chapter 76 - Tendon Transfers); Roberts and Hedges' Clinical Procedures in Emergency Medicine 7e
This is a shared conversation. Sign in to Orris to start your own chat.