Anti cancer drugs pharma notes
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I have comprehensive content. Now let me compile the full pharmacology notes.
Anti-Cancer Drugs - Pharmacology Notes
Sources: Lippincott Illustrated Reviews: Pharmacology; Schwartz's Principles of Surgery, 11th Ed.
I. OVERVIEW
Cancer affects >25% of the population. Less than a quarter of patients are cured by surgery/radiation alone - most require systemic chemotherapy. Only ~10% achieve cure or prolonged remission from chemotherapy. The overall 5-year survival rate is ~68%.
Types of chemotherapy by intent:
- Adjuvant chemotherapy - given after surgery/radiation to attack micrometastases
- Neoadjuvant chemotherapy - given before surgery to shrink the tumor
- Maintenance chemotherapy - lower doses to prolong remission
- Palliative chemotherapy - to reduce tumor burden and symptoms when cure is not possible
II. CELL CYCLE & DRUG CLASSIFICATION
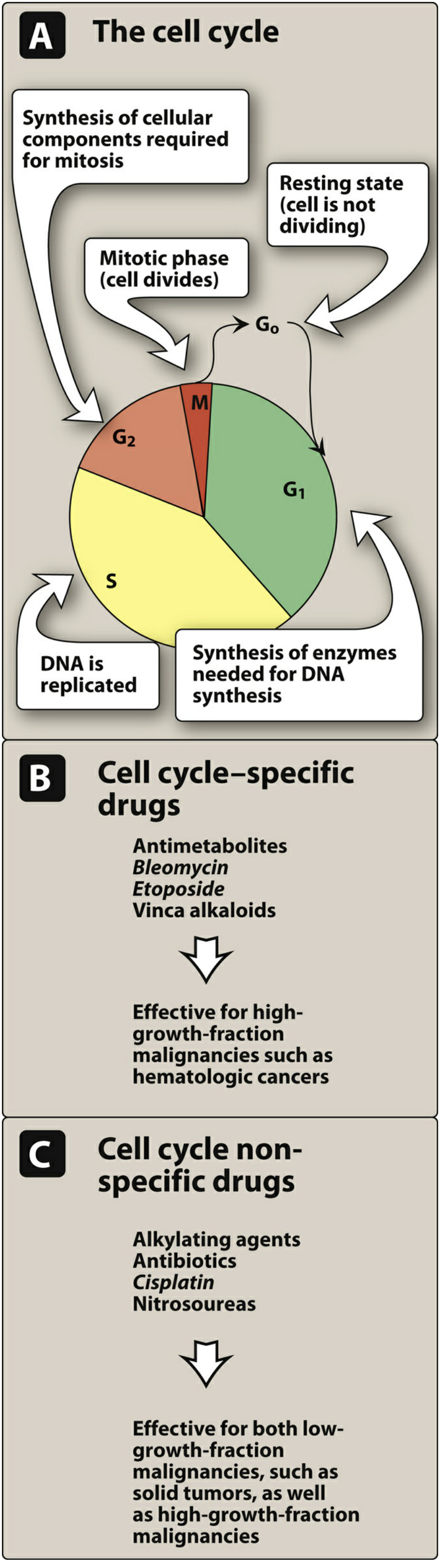
Figure: Effects of chemotherapeutic agents on the cell cycle. Cell cycle-specific drugs (antimetabolites, bleomycin, etoposide, vinca alkaloids) are effective for high-growth-fraction malignancies. Cell cycle non-specific drugs (alkylating agents, antibiotics, cisplatin, nitrosoureas) work in any phase.
Cell Cycle Phases
| Phase | Activity |
|---|---|
| G1 | Synthesis of enzymes needed for DNA synthesis |
| S | DNA replication |
| G2 | Synthesis of cellular components for mitosis |
| M | Mitosis - cell divides |
| G0 | Resting state - resistant to many chemotherapy agents |
Cell Cycle Specificity
- Cell cycle-specific (CCS): Act in a specific phase; most effective in tumors with high growth fraction (e.g., hematologic malignancies)
- Examples: antimetabolites (S phase), vinca alkaloids (M phase), bleomycin, etoposide
- Cell cycle-nonspecific (CCNS): Kill cells in any phase; effective for solid tumors and hematologic cancers
- Examples: alkylating agents, antitumor antibiotics, cisplatin, nitrosoureas
III. LOG KILL PHENOMENON
Chemotherapy follows first-order kinetics - a given dose destroys a constant fraction of cells (not a fixed number). A "5-log kill" = 99.999% cell destruction. When ~10^9 leukemic cells are reduced sufficiently, the patient enters remission (asymptomatic), but residual cells remain and require further treatment.
IV. DRUG RESISTANCE
A. Mechanisms of Resistance
- Inherent resistance: Melanoma is intrinsically resistant to most agents
- Acquired resistance: Cells mutate, especially with prolonged suboptimal dosing
B. Multidrug Resistance (MDR)
- Caused by amplification of the P-glycoprotein gene (transmembrane efflux pump)
- ATP-dependent pump removes drugs from the cell
- Cross-resistance: cells resistant to vinca alkaloids are also resistant to dactinomycin, anthracyclines, and colchicine (all share a hydrophobic aromatic ring + positive charge at neutral pH)
- Verapamil (at high concentrations) can inhibit the pump and reverse MDR
V. COMBINATION CHEMOTHERAPY
Combining drugs with different mechanisms and nonoverlapping toxicities is superior to monotherapy. Advantages:
- Maximal cell killing within tolerated toxicity
- Effective against a broader range of cells in heterogeneous tumors
- Delays or prevents emergence of resistant cell lines
Example regimen - R-CHOP (for non-Hodgkin lymphoma):
- R = Rituximab
- C = Cyclophosphamide
- H = Hydroxydaunorubicin (doxorubicin)
- O = Oncovin (vincristine)
- P = Prednisone
VI. DRUG CLASSES
A. ALKYLATING AGENTS (Cell Cycle Non-Specific)
Mechanism: Cross-link the two DNA strands (interstrand or intrastrand) or cause direct DNA damage → prevents cell division → apoptosis.
Subgroups:
1. Classic Alkylating Agents (Nitrogen Mustards)
| Drug | Key Use/Notes |
|---|---|
| Cyclophosphamide | Lymphomas, breast cancer; prodrug activated by CYP450; causes hemorrhagic cystitis (prevented by mesna) |
| Ifosfamide | Sarcomas; also causes hemorrhagic cystitis - requires mesna |
| Chlorambucil | CLL (chronic lymphocytic leukemia) |
| Melphalan | Multiple myeloma |
| Mechlorethamine (nitrogen mustard) | Hodgkin lymphoma |
| Busulfan | CML (conditioning for bone marrow transplant); causes pulmonary fibrosis |
2. Nitrosoureas (lipid soluble - cross blood-brain barrier)
| Drug | Key Use/Notes |
|---|---|
| Carmustine (BCNU) | Brain tumors (glioblastoma); also Hodgkin lymphoma |
| Lomustine (CCNU) | Brain tumors |
| Streptozocin | Pancreatic islet cell tumors |
3. Platinum Compounds (Miscellaneous DNA-Binding Agents)
| Drug | Key Use/Notes |
|---|---|
| Cisplatin | Testicular, ovarian, bladder, lung cancers; causes nephrotoxicity, ototoxicity, peripheral neuropathy, severe nausea/vomiting |
| Carboplatin | Similar to cisplatin; less nephrotoxic/neurotoxic but more myelosuppressive |
| Dacarbazine | Melanoma, Hodgkin lymphoma |
| Procarbazine | Hodgkin lymphoma |
Key toxicities of alkylating agents: Myelosuppression, nausea/vomiting, mucositis, secondary leukemias
B. ANTIMETABOLITES (Cell Cycle Specific - S Phase)
Mechanism: Structural analogs of normal metabolites (purines, pyrimidines, folates) → interfere with DNA/RNA synthesis by inhibiting key enzymes or incorporating into nucleic acids.
1. Folate Antagonists
Methotrexate (MTX)
- Inhibits dihydrofolate reductase (DHFR) → blocks folate reduction → depletes tetrahydrofolate → blocks thymidylate and purine synthesis
- Uses: ALL (acute lymphoblastic leukemia), choriocarcinoma, osteosarcoma, breast cancer, NHL; also used for RA and psoriasis
- Toxicity: Myelosuppression, mucositis, hepatotoxicity, nephrotoxicity
- Leucovorin (folinic acid) rescue is used after high-dose MTX to rescue normal cells
- Not given intrathecally without preservative-free formulation
Pemetrexed - Inhibits multiple folate-dependent enzymes; used for mesothelioma and NSCLC; requires folic acid + B12 supplementation to reduce toxicity
Pralatrexate - Used for peripheral T-cell lymphoma
2. Pyrimidine Antagonists
5-Fluorouracil (5-FU)
- Converted to FdUMP → irreversibly inhibits thymidylate synthase (TS) → blocks dTMP synthesis → "thymineless death"
- Also incorporated into RNA → disrupts RNA processing
- Uses: Colorectal cancer, breast cancer, gastric cancer, head and neck cancers
- Toxicity: Myelosuppression, mucositis/stomatitis, hand-foot syndrome (palmar-plantar erythrodysesthesia), cerebellar toxicity
- Leucovorin enhances 5-FU cytotoxicity by stabilizing FdUMP-TS complex
Capecitabine (Xeloda)
- Oral prodrug of 5-FU; converted to 5-FU preferentially in tumor tissue by thymidine phosphorylase
- Uses: Colorectal cancer, breast cancer
- Toxicity: Hand-foot syndrome (prominent)
Cytarabine (Ara-C)
- Pyrimidine antagonist; analog of deoxycytidine
- Activated to Ara-CTP → inhibits DNA polymerase and incorporated into DNA causing chain termination
- Major use: AML (acute myelogenous leukemia)
- Given IV (oral route inactive due to deamination in gut); intrathecal for meningeal leukemia
- S phase specific
Gemcitabine
- Deoxycytidine analog; activated by deoxycytidine kinase
- Uses: Pancreatic cancer, NSCLC (non-small cell lung cancer), bladder cancer, breast cancer
- Route: IV
Azacitidine (Vidaza)
- Pyrimidine nucleoside analog; used for myelodysplastic syndromes (MDS) and AML
- Acts by DNA hypomethylation and incorporation into DNA/RNA
3. Purine Antagonists
6-Mercaptopurine (6-MP)
- Activated by HGPRT → inhibits purine synthesis
- Use: ALL in children (maintenance therapy)
- Metabolized by xanthine oxidase → dose must be reduced by 75% with allopurinol (which inhibits XO)
6-Thioguanine (6-TG)
- Similar to 6-MP; used in AML and ALL
Fludarabine
- Used in CLL (chronic lymphocytic leukemia); also B-cell lymphomas
- Can cause severe immunosuppression
Cladribine
- Used for hairy cell leukemia
C. ANTITUMOR ANTIBIOTICS (Cell Cycle Non-Specific)
Mechanism: Products of microbial fermentation; interfere with DNA/RNA synthesis.
Anthracyclines
Doxorubicin (Adriamycin)
- Mechanism: Intercalates into DNA; inhibits topoisomerase II; generates free radicals
- Uses: Breast cancer, lymphomas, leukemias, sarcomas (broadest-spectrum anticancer antibiotic)
- Toxicity: Cardiotoxicity (dose-related cardiomyopathy; cumulative dose limit ~550 mg/m²), myelosuppression, alopecia, mucositis, red urine (not hematuria)
- Dexrazoxane is a cardioprotective agent used to reduce cardiotoxicity
- Vesicant (causes tissue necrosis if extravasated)
Daunorubicin (Cerubidine) - AML and ALL; similar cardiotoxicity
Epirubicin (Ellence) - Breast cancer; less cardiotoxic than doxorubicin
Idarubicin (Idamycin) - AML
Non-Anthracycline Antibiotics
Bleomycin
- Causes single- and double-strand DNA breaks by generating free radicals
- Uses: Testicular cancer, Hodgkin lymphoma (ABVD regimen)
- Unique toxicity: Pulmonary fibrosis (dose-limiting); skin reactions
- Minimal myelosuppression (useful in combination protocols)
- Cell cycle specific (G2/M phase)
Mitomycin C
- Alkylating antibiotic; used for gastric and colorectal cancers
- Toxicity: Myelosuppression, hemolytic uremic syndrome
Dactinomycin (Actinomycin D)
- Intercalates into DNA; inhibits RNA synthesis
- Uses: Wilms tumor, rhabdomyosarcoma, gestational trophoblastic neoplasia, Ewing sarcoma
D. MICROTUBULE INHIBITORS (Cell Cycle Specific - M Phase)
1. Vinca Alkaloids (Inhibit Microtubule Polymerization)
Derived from the periwinkle plant (Vinca rosea).
Mechanism: Bind to tubulin → block microtubule polymerization → impair mitotic spindle formation → arrest at M phase
| Drug | Uses | Key Toxicity |
|---|---|---|
| Vincristine | ALL (children), Wilms tumor, rhabdomyosarcoma, Ewing sarcoma, Hodgkin/NHL; the "O" in R-CHOP | Peripheral neuropathy (dose-limiting), constipation; minimal myelosuppression |
| Vinblastine | Metastatic testicular carcinoma (with bleomycin + cisplatin), Hodgkin lymphoma, Kaposi sarcoma | Myelosuppression (dose-limiting), neurotoxicity |
| Vinorelbine | Breast cancer, NSCLC | Granulocytopenia |
Important: All vinca alkaloids are vesicants (IV only). Intrathecal administration may result in death.
Drug interactions: CYP3A4 inhibitors (azole antifungals, clarithromycin, ritonavir) increase toxicity.
2. Taxanes (Inhibit Microtubule Depolymerization)
Mechanism: Opposite of vinca alkaloids - cause excess polymerization and stabilization of microtubules → block cell cycle in M phase
| Drug | Uses | Key Toxicity |
|---|---|---|
| Paclitaxel (Taxol) | Breast, ovarian, NSCLC, KS | Neutropenia, peripheral neuropathy, alopecia; hypersensitivity reactions (premedicate with corticosteroids + antihistamines) |
| Docetaxel (Taxotere) | Breast, NSCLC, prostate, gastric | Neutropenia, fluid retention syndrome, peripheral neuropathy |
E. TOPOISOMERASE INHIBITORS
Mechanism: Inhibit DNA topoisomerase enzymes that relieve torsional strain during DNA replication.
| Drug | Topoisomerase Target | Uses | Toxicity |
|---|---|---|---|
| Etoposide (VP-16) | Topo II (stabilizes DNA-Topo II complex → cannot religate → DNA strand breaks) | Testicular cancer, SCLC, lymphomas | Myelosuppression, secondary leukemia |
| Teniposide | Topo II | ALL | Myelosuppression |
| Irinotecan | Topo I | Colorectal cancer | Diarrhea (acute: cholinergic; delayed: secretory) |
| Topotecan | Topo I | Ovarian cancer, SCLC | Myelosuppression |
F. HORMONAL AGENTS
Used for hormone-responsive tumors (breast, prostate, endometrial cancers).
1. Antiestrogens (for Breast Cancer)
| Drug | Mechanism | Use |
|---|---|---|
| Tamoxifen | Competitive ER antagonist in breast tissue | ER+ breast cancer (adjuvant and treatment); increases risk of endometrial cancer and thromboembolism |
| Fulvestrant | Selective estrogen receptor downregulator (SERD) | ER+ metastatic breast cancer |
| Raloxifene | SERM; ER antagonist in breast, partial agonist in bone | Breast cancer prevention; osteoporosis |
2. Aromatase Inhibitors (for Breast Cancer)
- Block conversion of androgens to estrogens by inhibiting aromatase
- Anastrozole, letrozole (nonsteroidal) - postmenopausal ER+ breast cancer
- Exemestane (steroidal) - similar use
3. Antiandrogens (for Prostate Cancer)
| Drug | Mechanism |
|---|---|
| Leuprolide, goserelin | GnRH agonists → initial surge then down-regulation of LH/FSH → castration-level testosterone |
| Flutamide, bicalutamide | Androgen receptor antagonists |
| Enzalutamide | 2nd-generation AR antagonist; castration-resistant prostate cancer |
| Abiraterone | CYP17 inhibitor → blocks androgen synthesis; requires concurrent prednisone |
G. TARGETED THERAPY
1. Tyrosine Kinase Inhibitors (TKIs) - Oral
Mechanism: Mimic ATP to prevent ATP binding to kinase → block phosphorylation of downstream signaling proteins → inhibit proliferation.
| Drug | Kinase Target | Primary Use | Key Notes |
|---|---|---|---|
| Imatinib (Gleevec) | BCR-ABL | CML (first TKI approved) | Monitor for heart failure |
| Dasatinib | BCR-ABL, SRC family | CML (imatinib-resistant) | Avoid with PPIs; monitor bone density |
| Erlotinib | EGFR | NSCLC, pancreatic cancer | Rash correlates with clinical response |
| Gefitinib | EGFR | NSCLC with EGFR mutations | |
| Afatinib | EGFR family | NSCLC | Take on empty stomach |
| Crizotinib | ALK, ROS1 | NSCLC with ALK rearrangements | Give with antiemetics |
| Vemurafenib | BRAF V600E | Melanoma with BRAF mutation | |
| Sorafenib | VEGF family | HCC, RCC, thyroid cancer | Wound healing complications |
| Ibrutinib | BTK (Bruton's tyrosine kinase) | CLL, mantle cell lymphoma | Monitor for heart failure; secondary malignancies |
| Ruxolitinib | JAK family | Myelofibrosis, polycythemia vera | Increased VTE risk |
| Midostaurin | FLT3 | AML with FLT3 mutation | |
| Lapatinib | EGFR/HER2 | HER2+ breast cancer | Severe hepatotoxicity, diarrhea |
Resistance: Acquired resistance common (mutations in ATP-binding site). KRAS mutations cause primary resistance to upstream EGFR inhibitors.
2. Monoclonal Antibodies (mAbs)
| Drug | Target | Use |
|---|---|---|
| Trastuzumab (Herceptin) | HER2/neu (ErbB2) | HER2+ breast cancer, gastric cancer; cardiotoxicity |
| Rituximab (Rituxan) | CD20 | B-cell NHL, CLL; infusion reactions |
| Bevacizumab (Avastin) | VEGF | Colorectal, NSCLC, glioblastoma; risk of bleeding, hypertension, wound healing impairment |
| Cetuximab | EGFR | Colorectal cancer, head and neck cancer; requires KRAS wild-type |
| Pertuzumab | HER2 dimerization domain | HER2+ breast cancer (with trastuzumab) |
H. MISCELLANEOUS AGENTS
Hydroxyurea
- Inhibits ribonucleotide reductase → blocks conversion of ribonucleotides to deoxyribonucleotides → S phase specific
- Used in CML, polycythemia vera, sickle cell disease
L-Asparaginase
- Depletes serum asparagine → tumor cells (that lack asparagine synthetase) cannot synthesize protein
- Used for ALL in children
- Toxicity: Hypersensitivity, pancreatitis, coagulopathy, hepatotoxicity
Thalidomide / Lenalidomide
- Antiangiogenic + immunomodulatory properties
- Used for multiple myeloma; thalidomide also for erythema nodosum leprosum
- Teratogenic (Category X)
Bortezomib (Velcade)
- Proteasome inhibitor → accumulation of misfolded proteins → apoptosis
- Used for multiple myeloma and mantle cell lymphoma
VII. ADVERSE EFFECTS SUMMARY
| Toxicity | Key Drugs |
|---|---|
| Myelosuppression | Most cytotoxics; worst with alkylating agents, anthracyclines |
| Cardiotoxicity | Doxorubicin (dose-related, cumulative), trastuzumab (reversible), cyclophosphamide (high-dose) |
| Pulmonary fibrosis | Bleomycin, busulfan, carmustine |
| Nephrotoxicity | Cisplatin, methotrexate (high-dose), ifosfamide |
| Hemorrhagic cystitis | Cyclophosphamide, ifosfamide (prevented by mesna + hydration) |
| Peripheral neuropathy | Vincristine (dose-limiting), paclitaxel, cisplatin |
| Ototoxicity | Cisplatin |
| Hepatotoxicity | Methotrexate, lapatinib, 6-MP with allopurinol |
| Secondary malignancies | Alkylating agents (AML after ~5-10 years), etoposide |
| Alopecia | Doxorubicin, cyclophosphamide, paclitaxel |
| Hand-foot syndrome | Capecitabine, 5-FU infusion, sorafenib |
| GI toxicity (diarrhea) | Irinotecan, 5-FU, capecitabine |
VIII. HIGH-YIELD MNEMONICS
Remember vesicants (extravasation → tissue necrosis):
- Vinca alkaloids, anthracyclines (doxorubicin, daunorubicin), nitrogen mustards, mitomycin
Drugs requiring dose reduction with renal failure:
- Methotrexate, cisplatin, bleomycin, carboplatin
Drugs NOT requiring dose reduction for renal failure:
- Vincristine, doxorubicin (hepatic elimination)
ABVD regimen (Hodgkin lymphoma):
- A = Doxorubicin (Adriamycin), B = Bleomycin, V = Vinblastine, D = Dacarbazine
References: Lippincott Illustrated Reviews: Pharmacology, 8th Ed., Chapter 37 (pp. 1208-1267) | Schwartz's Principles of Surgery, 11th Ed. (pp. 367-368) | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.