Injuries of the lower limb
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching Images
lower limb fractures hip knee ankle classification
I now have comprehensive information to provide a thorough overview. Let me compile the response:
Injuries of the Lower Limb
A systematic overview covering fractures, dislocations, soft tissue injuries, and muscle injuries of the lower extremity, drawn from Rockwood and Green's Fractures in Adults (10th ed., 2025) and Gray's Anatomy for Students.
1. Proximal Femur Fractures
Femoral Neck Fractures
These are predominantly fragility fractures of the elderly (average age ~80 years, 64% female). The majority (80%) result from a simple fall from standing height.
| Subtype | Prevalence | Average Age | M/F |
|---|---|---|---|
| Displaced | 63% | 81.1 yr | 34/66 |
| Minimally displaced | 25% | 78.5 yr | 34/66 |
| Basiocervical | 12% | 80.2 yr | 42/58 |
Key complications:
- 1-year mortality in elderly: ~30%
- 15–20% cannot return to previous residence
Trochanteric (Intertrochanteric/Subtrochanteric) Fractures
Also predominantly fragility fractures (84% from standing falls, average age >81 years, 69–78% female).
| Subtype | Prevalence | 1-yr Mortality |
|---|---|---|
| Intertrochanteric | 78% | ~26% |
| Subtrochanteric | 22% | ~26% |
The femoral head fracture is rare and strongly associated with hip dislocation (25% of hip dislocations have a concomitant femoral head fracture).
2. Femoral Diaphysis Fractures
Historically considered a "young person's fracture" from high-energy trauma (road traffic accidents), the epidemiology has shifted. Today the femoral diaphyseal fracture is a fragility fracture, increasingly seen in elderly patients, particularly elderly women. Periprosthetic fractures are now 17% of cases (average age 78 years). The annual overall incidence is approximately 14.3 per 100,000 population.
3. Distal Femur Fractures
Regarded as the classic fracture of elderly women — rare in young males, rising in incidence with age in both sexes, with a marked female predominance. 27.9% are periprosthetic (70% around knee prostheses).
| Type | Prevalence | Avg Age | M/F |
|---|---|---|---|
| Extra-articular | 38.6% | 64.6 yr | 33/67 |
| Partial articular | 17.6% | 60.2 yr | 55/45 |
| Complete articular | 6.4% | 63.1 yr | 45/55 |
| Periprosthetic | 27.9% | 77.4 yr | 18/82 |
1-year mortality is approximately 21%.
4. Patella Fractures
Relatively rare, with a bimodal distribution (type F curve). About two-thirds result from a standing fall in older patients; in younger males, motorcycle injuries account for two-thirds of cases. Transverse fractures are most common.
5. Proximal Tibia (Tibial Plateau) Fractures
Account for 2% of all fractures. Show a bimodal distribution (type H): high-energy injuries in younger males (>60% occur in men under 50), and fragility-type injuries in older women (>77% of women are over 50).
| Type | Prevalence | Avg Age | M/F |
|---|---|---|---|
| Partial articular | 64% | 54 yr | 38/62 |
| Extra-articular | 18% | 56 yr | 50/50 |
| Complete articular | 18% | 53 yr | 47/53 |
Key complications:
- Compartment syndrome: 8.3%
- Post-traumatic arthritis: 9–27%
- Open fractures: 1.6%
6. Tibial Diaphysis Fractures
Now account for only ~1.1% of fractures treated by orthopaedic surgeons (declining incidence, likely reflecting improved road safety). The distribution remains type A (bimodal, but shifting). About 35% result from high-energy mechanisms.
7. Ankle Fractures
One of the most common lower limb fractures, accounting for 10.3% of all fractures. Annual incidence: 137–158 per 100,000 population (rising trend).
Classification (OTA/Weber):
| Type | Prevalence | Avg Age | M/F |
|---|---|---|---|
| Transsyndesmotic (B) | 63.6% | 57 yr | 38/62 |
| Infrasyndesmotic (A) | 24.3% | 53 yr | 36/64 |
| Suprasyndesmotic (C) | 12.1% | 52 yr | 52/48 |
- 65.7% are caused by a standing fall
- Bimalleolar and trimalleolar fractures should be regarded as fragility fractures in the elderly
- Open ankle fractures in elderly women carry mortality comparable to proximal femoral fractures
8. Calcaneal Fractures
The most common tarsal fracture. The dominant mechanism is a fall from a height (69%). Two main types:
- Articular (type C): younger males, high-energy — more commonly bilateral, with associated lumbar spine fractures (8–17%) and contralateral calcaneal fracture (3–8%)
- Non-articular: older patients
9. Midfoot & Metatarsal Fractures
- Metatarsal fractures are common (6.6% of all fractures; incidence ~124/100,000). The 5th metatarsal is most frequently fractured. Bimodal distribution: young males and older females.
- Midfoot (navicular, cuboid, cuneiform) fractures are rare; navicular is the most frequently injured midfoot bone (42% of midfoot fractures).
10. Dislocations
Hip Dislocations
- Rare, typically high-energy (motor vehicle accidents, contact sport)
- Annual incidence: 0.8 per 100,000 (adults)
- 96% are posterior dislocations
- 75% associated with fractures (acetabular rim, femoral head)
- Prosthetic hip dislocations are far more common (22/100,000 in adults)
Knee Dislocations
- Very rare (tibiofemoral): ~0.6/100,000; require high-energy trauma; associated with multiligament injury and vascular injury risk
- Patellofemoral dislocations: much more common (21.6/100,000 overall); peak in adolescents and young adults, especially females aged 10–17; 22.7% risk of recurrence. Annual incidence in Finnish/Danish studies: 30–43/100,000.
Ankle & Foot Dislocations
- Typically associated with high-energy trauma or fracture-dislocations
- Isolated dislocations are rare
11. Soft Tissue (Ligamentous & Tendon) Injuries
Major lower limb soft tissue injuries by incidence (per 100,000/year):
| Injury | Incidence | M/F | Avg Age |
|---|---|---|---|
| Meniscal tear | 23.8 | 75/25 | 33–35 yr |
| Achilles tendon rupture | 11.3 | 68/32 | 43–47 yr |
| Anterior cruciate ligament (ACL) | 8.1 | 76/24 | ~28 yr |
| Medial collateral ligament (MCL) | 5.2 | 75/25 | 31–39 yr |
| Posterior cruciate ligament (PCL) | — | male > female | younger |
| Lateral collateral ligament (LCL) | — | male > female | younger |
ACL injuries: type C distribution (young adults). Swedish MRI-based studies report much higher incidence (~77/100,000), likely reflecting improved diagnostics.
12. Muscle Injuries
Muscle injuries result from direct trauma or overuse. They range from minor fiber tears (focal fluid on imaging) to complete muscle tears.
Hamstring Injuries
The most clinically important lower limb muscle injury. Common in athletes requiring power and speed (sprinting, football, track and field).
- Mechanism: sudden acceleration/deceleration or rapid change of direction
- Usual site: musculotendinous junction in adults
- In adolescents: ischial apophysis avulsion (the apophysis is the weakest link in the proximal hamstring unit)
- Diagnosed with ultrasound or MRI — MRI also gives prognostic information (re-tear risk, functional loss)
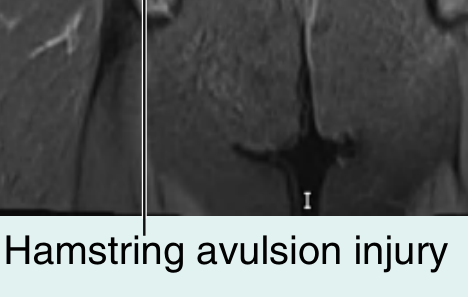
Coronal MRI showing hamstring avulsion injury at the ischial tuberosity — Gray's Anatomy for Students
Soleus & Lower Leg Muscles
Below the knee, the soleus is the most common site of muscle tears, though other muscles of the posterior compartment may be affected.
Summary: Key Clinical Pearls
| Injury | Typical Patient | Mechanism | Key Complication |
|---|---|---|---|
| Femoral neck fracture | Elderly woman | Low fall | 30% 1-yr mortality, AVN |
| Intertrochanteric fracture | Elderly woman | Low fall | 26% 1-yr mortality |
| Femoral shaft fracture | Historically young male; now also elderly | RTA / fragility | Fat embolism, blood loss |
| Distal femur fracture | Elderly woman / post-TKR | Low fall | Periprosthetic (28%) |
| Tibial plateau fracture | Young male / elderly female | High energy / low fall | Compartment syndrome (8.3%) |
| Ankle fracture | All ages | Twisting fall | Bimalleolar = fragility in elderly |
| Calcaneal fracture | Young to middle-aged male | Fall from height | Spinal fracture (8–17%) |
| ACL tear | Young adult | Sports | Meniscal injury, instability |
| Achilles rupture | Active middle-aged male | Eccentric load | Re-rupture |
| Hamstring avulsion | Adolescent athlete | Sudden hip flexion | Chronic pain, weakness |
Sources: Rockwood and Green's Fractures in Adults, 10th ed. (2025), pp. 205–219 | Gray's Anatomy for Students, pp. 702–703
Explain each of them
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.