I have my university exam of 1 st year of subject physiology These are the important long answer give me answer of this question "Chemical regulation of respiration, periodic breathing" and remeber it's a long question
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content and diagrams needed. Let me write the comprehensive exam answer.
Chemical Regulation of Respiration and Periodic Breathing
Sources: Guyton & Hall Textbook of Medical Physiology; Ganong's Review of Medical Physiology
INTRODUCTION
The primary goal of respiration is to maintain proper concentrations of O2, CO2, and H+ in the tissues. The respiratory center in the medulla does not work blindly - it is constantly monitored and adjusted by chemical signals in the blood and cerebrospinal fluid (CSF). This chemical regulation operates through two systems:
- Central chemoreceptors - located in the medulla, mainly sensitive to CO2 and H+
- Peripheral chemoreceptors - carotid and aortic bodies, mainly sensitive to O2
PART 1: CHEMICAL CONTROL OF RESPIRATION
A. Role of CO2 and H+ - Central Chemoreceptors
Location of the Chemosensitive Area
The most important central chemical control site is the retrotrapezoid nucleus (chemosensitive area), located bilaterally just 0.2 mm beneath the ventral surface of the rostral medulla. Neurons throughout the brain stem, including the dorsal and ventral respiratory groups, also show chemosensitivity.
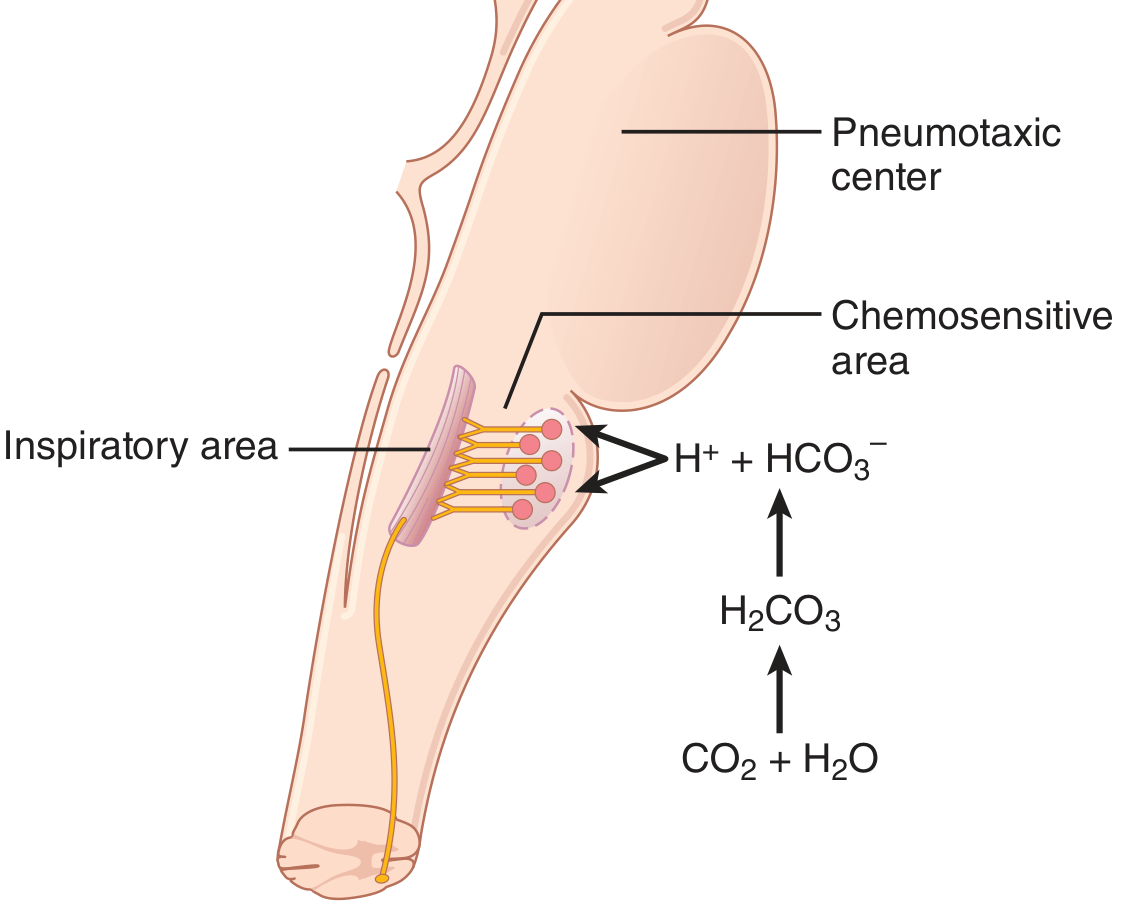
Figure 1: CO2 diffuses into the CSF, reacts with water to form H+, which then directly stimulates the chemosensitive neurons of the medulla, ultimately exciting the inspiratory area. (Guyton & Hall)
How H+ Stimulates the Chemosensitive Neurons
The sensor neurons are primarily excited by H+ ions. However, H+ does NOT easily cross the blood-brain barrier, so changes in blood H+ have a relatively weak effect compared to CO2.
How CO2 Indirectly Stimulates the Chemosensitive Neurons
Although CO2 has little direct effect on chemosensitive neurons, it has a very potent indirect effect. When blood PCO2 rises, CO2 crosses the blood-brain barrier easily and reacts with water in the CSF and brain interstitial fluid:
CO2 + H2O → H2CO3 → H+ + HCO3-
This H+ then directly excites the chemosensitive neurons. This is why blood CO2 produces a much stronger respiratory response than blood H+:
- CO2 crosses the blood-brain barrier freely
- Blood H+ cannot cross it effectively
Quantitative Effect
- A rise in arterial PCO2 from 35 to 75 mm Hg causes a marked increase in alveolar ventilation
- A fall in blood pH from 7.5 to 7.3 (normal range) causes less than 10% the effect that CO2 causes
Adaptation After 1-2 Days
When CO2 remains chronically elevated, the stimulatory effect diminishes to about 1/5 of its initial level. This occurs because:
- Kidneys compensate by increasing blood HCO3-, reducing H+
- HCO3- slowly diffuses across the blood-brain barrier, neutralising H+ near the respiratory neurons
- So CO2 has a powerful acute effect but only a weak chronic effect on respiration
B. Role of Oxygen - Peripheral Chemoreceptors
Why O2 is Not the Primary Controller
Due to the haemoglobin-oxygen buffering system, adequate O2 delivery to tissues is maintained even when alveolar PO2 varies widely (from ~60 to >1000 mm Hg). CO2, in contrast, changes inversely with ventilation and directly affects every tissue. For this reason, evolution has made CO2 the primary controller of respiration, not O2.
O2 has virtually no direct effect on the medullary respiratory centre. Instead, it acts through peripheral chemoreceptors.
Structure and Location of Peripheral Chemoreceptors
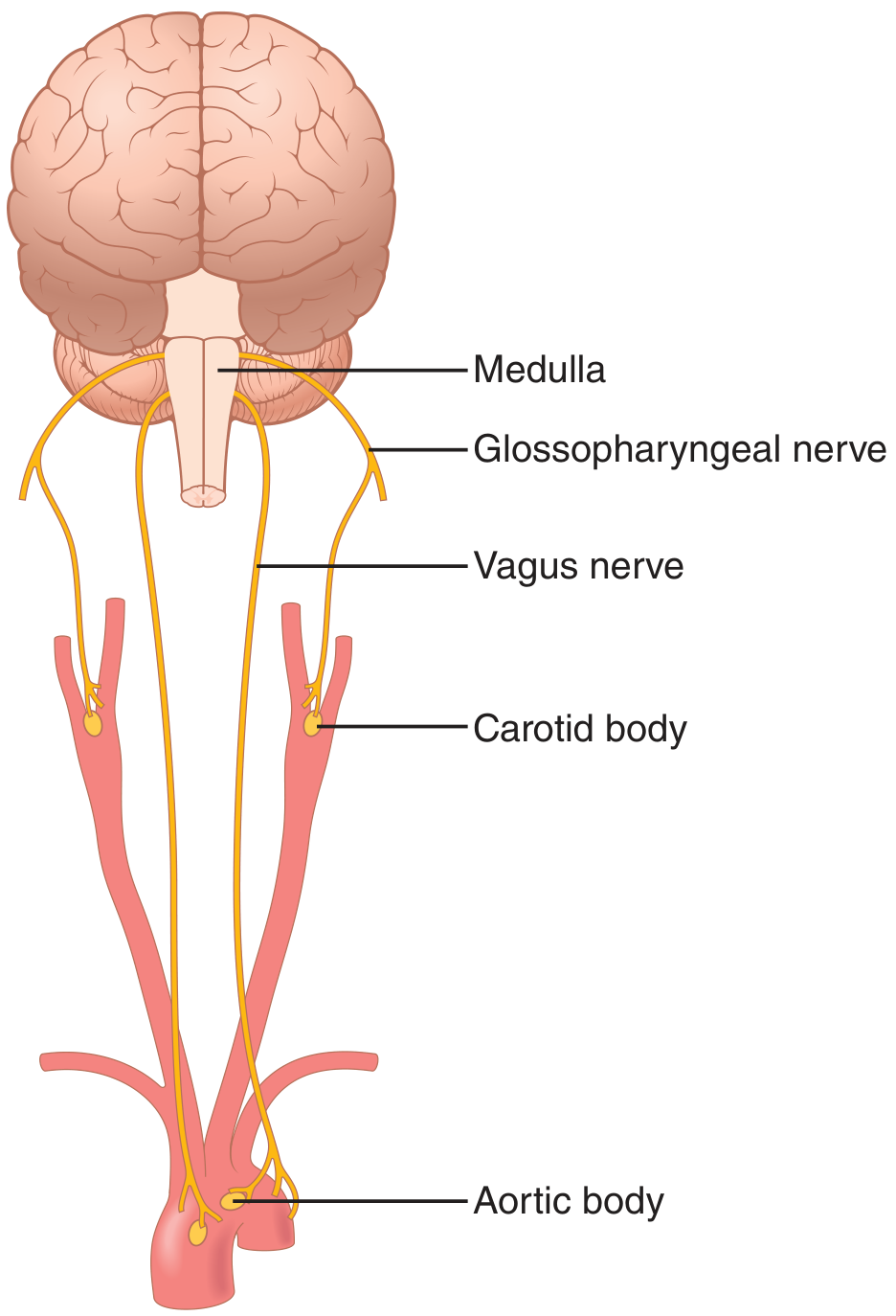
Figure 2: Peripheral chemoreceptors in the carotid and aortic bodies. Carotid body signals travel via the glossopharyngeal nerve; aortic body signals via the vagus nerve. Both project to the dorsal respiratory area of the medulla. (Guyton & Hall)
| Chemoreceptor | Location | Afferent Nerve |
|---|---|---|
| Carotid bodies (most important) | Bifurcation of common carotid arteries (bilateral) | Hering's nerve → Glossopharyngeal nerve (CN IX) |
| Aortic bodies | Arch of the aorta | Vagus nerve (CN X) |
Special blood supply: These bodies receive blood flow 20 times their own weight per minute, so the chemoreceptors always sense arterial blood, not venous blood.
How Glomus Cells Sense Hypoxia (Mechanism)
The carotid and aortic bodies contain glomus cells (Type I cells) which function as the actual O2 sensors:
- When arterial PO2 falls below ~60 mm Hg, K+ channels in glomus cells close
- This causes membrane depolarization
- Voltage-gated Ca2+ channels open → intracellular Ca2+ rises
- Increased Ca2+ triggers release of neurotransmitters (mainly ATP, also dopamine and acetylcholine)
- These activate afferent nerve fibers → signals sent to the medullary respiratory centre → increased ventilation
Threshold for O2 Response: Peripheral chemoreceptors show little response until PO2 falls below 100 mm Hg. Ventilation approximately doubles at PO2 = 60 mm Hg and can increase 5-fold at very low PO2 values.
Effect of CO2 and H+ on Peripheral Chemoreceptors
Peripheral chemoreceptors also respond to increases in CO2 and H+, but the effect is about 7 times less powerful than the central (medullary) response. However, the peripheral response is 5 times faster - making peripheral chemoreceptors important for rapid responses, such as at the onset of exercise.
Summary Table: Central vs Peripheral Chemoreceptors
| Feature | Central Chemoreceptors | Peripheral Chemoreceptors |
|---|---|---|
| Location | Retrotrapezoid nucleus, ventrolateral medulla | Carotid and aortic bodies |
| Primary stimulus | CO2 (via H+), H+ | O2 (low PO2 < 60 mmHg) |
| Secondary stimulus | - | CO2 and H+ (weaker) |
| O2 sensitivity | None (O2 has no direct effect) | Primary function |
| Speed of response | Slower | 5x faster for CO2 response |
| Potency for CO2/H+ | 7x more powerful | Less powerful |
| Afferent pathway | Intrinsic (within brainstem) | CN IX (carotid), CN X (aortic) |
PART 2: PERIODIC BREATHING
Definition
Periodic breathing is an abnormal pattern of breathing characterized by alternating cycles of hyperpnea (increased breathing) and apnea (cessation of breathing). The classic form is Cheyne-Stokes respiration.
A. Physiological Demonstration (Hyperventilation Model)
This illustrates how the chemical regulation system can become oscillatory:
- A normal subject voluntarily hyperventilates for 2-3 minutes
- Hyperventilation "washes out" CO2 → arterial PCO2 falls below threshold
- When voluntary effort stops, apnea occurs (due to low CO2)
- During apnea, alveolar PO2 falls and alveolar PCO2 rises
- When PO2 falls low enough, the carotid/aortic chemoreceptors are stimulated by hypoxia
- Breathing resumes with a few shallow breaths
- These breaths restore O2 but the CO2 is not yet normal → another apnea
- The cycle repeats until PCO2 gradually returns to normal → normal breathing resumes
Key fact: The apnea is due to lack of CO2, not lack of O2 - because it does NOT occur if hyperventilation is done with 5% CO2 mixtures.
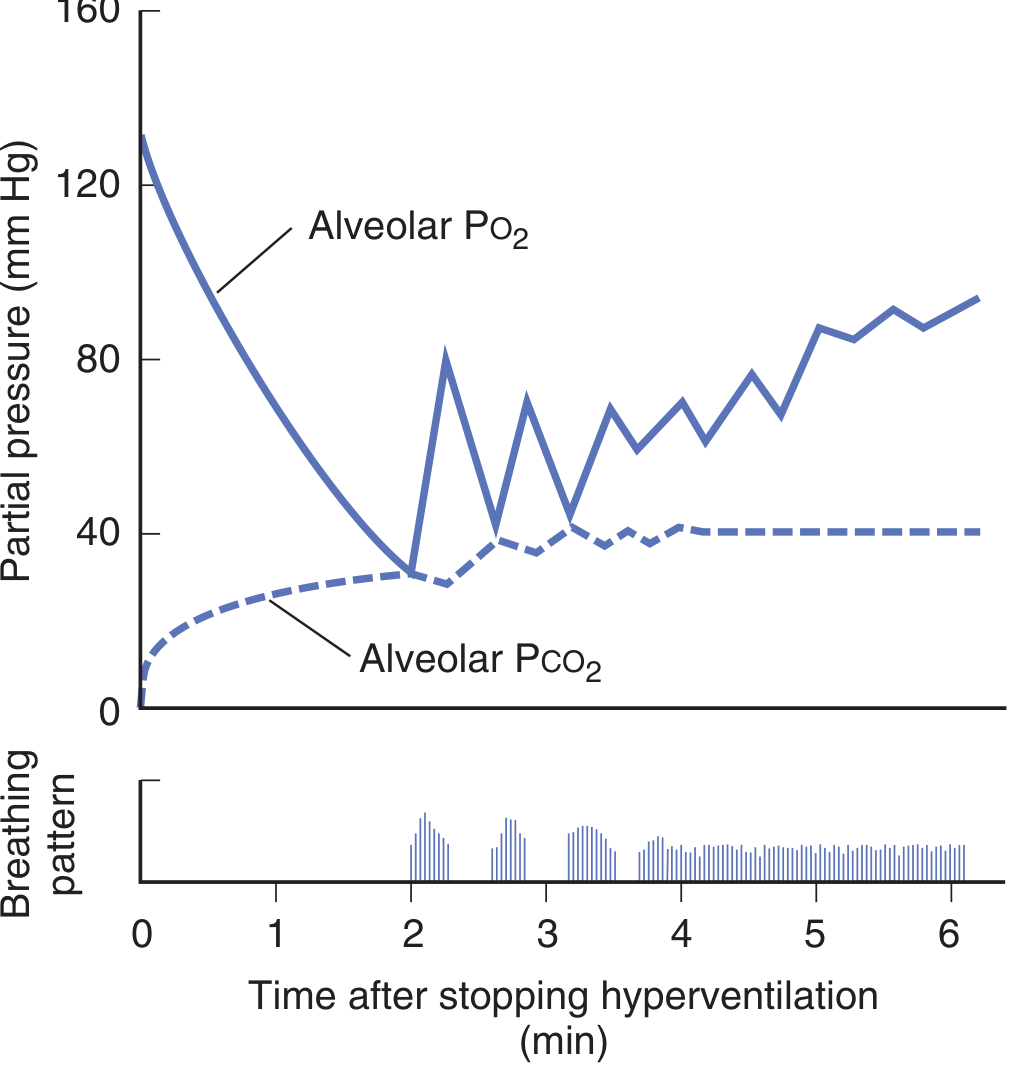
Figure 3: After forced hyperventilation, the graph shows alveolar PO2 dropping (triggering intermittent breaths) while PCO2 slowly rises back to normal. The bars at the bottom show the pattern of breathing alternating with apnea - classic periodic breathing. (Ganong's Review)
B. Cheyne-Stokes Respiration (Periodic Breathing in Disease)
Pattern: Gradual crescendo increase in depth of breathing → peak hyperpnea → gradual decrescendo → apnea → cycle repeats. Each cycle lasts approximately 30 seconds to 2 minutes.
Conditions Associated:
- Congestive heart failure (most common)
- Uremia (renal failure)
- Brain diseases (strokes, head injury, increased ICP)
- During sleep in some normal individuals (especially at altitude)
Mechanisms of Cheyne-Stokes Respiration
Mechanism 1 - Increased CO2 Sensitivity:
Some patients (especially with brain disease) have enhanced sensitivity to CO2:
- CO2 triggers relative hyperventilation (overshooting)
- Arterial PCO2 drops too low → apnea
- During apnea, PCO2 rises back to normal
- But the respiratory centre again overresponds to this normal CO2 → repeat cycle
Mechanism 2 - Prolonged Lung-to-Brain Circulation Time (Heart Failure):
In heart failure, cardiac output is reduced and the lung-to-brain circulation time is prolonged:
- Hyperventilation lowers PCO2 in pulmonary blood
- But this low-PCO2 blood takes longer than normal to reach the brain
- During transit, pulmonary capillary blood continues to lose more CO2
- When this very-low-PCO2 blood finally reaches the medulla → inhibits breathing → apnea
- During apnea, PCO2 builds up in arterial blood, but again takes extra time to reach the brain
- When high-PCO2 blood reaches the medulla → excessive stimulation → hyperventilation
- This oscillatory delay in feedback creates the waxing-and-waning pattern
C. Sleep Apnea
A related form of periodic breathing during sleep:
Central Sleep Apnea: Failure of neural discharge to respiratory muscles - the brain simply does not send the signal to breathe.
Obstructive Sleep Apnea (OSA): Upper airway obstruction due to relaxation of pharyngeal muscles and hypotonia of the genioglossus muscle (which normally pulls the tongue forward during inspiration). Most common during REM sleep.
Features of OSA:
- Loud snoring
- Morning headaches
- Daytime fatigue and sleepiness
- 7x increased risk of motor vehicle accidents
- Associated with hypertension, arrhythmia, stroke, and heart failure
Treatment: Weight loss, positional therapy, avoidance of muscle relaxants/alcohol, dental appliances, CPAP (Continuous Positive Airway Pressure) - the standard of care for moderate-to-severe OSA.
QUICK SUMMARY FOR REVISION
| Stimulus | Receptor | Mechanism | Effect |
|---|---|---|---|
| ↑ CO2 | Central (medulla) | CO2 → H+ in CSF → stimulates retrotrapezoid nucleus | ↑ Ventilation |
| ↑ H+ | Central (medulla) | Direct H+ stimulation (less potent than CO2) | ↑ Ventilation |
| ↓ PO2 (<60 mmHg) | Peripheral (carotid/aortic bodies) | K+ channel closure → depolarization → Ca2+ influx → ATP release | ↑ Ventilation |
| ↓ PO2 + ↑ CO2 | Both | Synergistic interaction | Strong ↑ Ventilation |
Periodic Breathing key points:
- Caused by instability in the feedback loop of chemical regulation
- Physiological cause: post-hyperventilation (CO2 washout)
- Pathological cause: Cheyne-Stokes respiration (heart failure, brain disease, uremia)
- Mechanism: either hypersensitivity to CO2 or delayed circulation time (long feedback loop)
- Sleep apnea = a form of periodic breathing during sleep (central or obstructive)
References: Guyton & Hall Textbook of Medical Physiology (14th Ed.), pp. 534-536; Ganong's Review of Medical Physiology (26th Ed.), pp. 665-666
This is a shared conversation. Sign in to Orris to start your own chat.