What is the treatment of Joint stiffness
"joint stiffness" treatment management
Treatment of Joint Stiffness
1. Prevention (Most Important First Step)
- Splints and casts should be used only for the minimum time required for healing.
- For minor injuries, immobilization should rarely exceed 5-7 days.
- Fractures or dislocations requiring >7 days of splinting need orthopedic follow-up.
- Patients should be told explicitly that prolonged immobilization is detrimental.
- Internal fixation of fractures has the major advantage of enabling early mobilization, thereby reducing stiffness risk.
2. Non-Operative (Conservative) Treatment
| Exercise Type | Purpose |
|---|---|
| Range-of-motion (ROM) & flexibility exercises | Maintain/restore joint mobility; always included in any protocol |
| Strengthening exercises | Restore muscle control and support around the joint |
| Aerobic exercise (land or aquatic) | Improve overall function; should be integrated with strengthening |
| Neuromuscular training (balance, stability, movement retraining) | Improve proprioception and movement patterns lost due to stiffness |
- ROM exercises alone are insufficient for pain and function improvement and should be combined with strengthening.
- Aquatic exercise is particularly useful: water reduces joint load, allows larger ROM with less pain.
- Neuromuscular training is valuable as it addresses multiple aspects of muscle impairments and neural control.
- When stiffness is present, splinting between exercise sessions and at night helps maintain gains in ROM.
- A splint relaxes muscles, maintains correct position, and immobilizes - but should be used correctly to avoid worsening stiffness or skin breakdown. (Campbell's Operative Orthopaedics, 15th ed)
| Drug Class | Indication |
|---|---|
| NSAIDs (oral) | Reduce pain and inflammation enabling exercise; first-line for inflammatory-type stiffness (OA, spondyloarthritis, tendinitis); use for 10-14 days for acute conditions |
| Intra-articular corticosteroids | Second-line when NSAIDs insufficient (e.g., enteropathic arthritis) |
| NSAIDs + anti-TNF agents | Rheumatoid/ankylosing spondylitis - reduce morning stiffness |
| Modified-release prednisone | Shown to reduce duration of morning stiffness in RA vs. standard prednisone (CAPRA-1 trial) |
| Colchicine | Useful in CPP crystal arthritis-related stiffness |
- Heat therapy (hot compresses, warm water): reduces pain and relaxes periarticular structures, commonly used for shoulder and axillary stiffness post-surgery.
- Massage therapy: for post-surgical stiffness (e.g., cording and shoulder stiffness after axillary surgery).
- Continuous Passive Motion (CPM): used post-contracture release, typically for ~12 hours/day for 1 week, though evidence is mixed. (Campbell's Operative Orthopaedics, 15th ed)
3. Operative Treatment
- Indicated when physiotherapy fails to achieve adequate ROM.
- Useful for proximal joint stiffness, especially post-amputation contractures. (Rockwood and Green's, 10th ed)
- Minimally invasive release of capsular contracture.
- Improves ROM effectively.
- Risk: delayed ulnar neuritis (11% in elbow arthroscopy), especially with severe flexion contractures - prophylactic ulnar nerve decompression is recommended. (Campbell's Operative Orthopaedics, 15th ed)
- For severe/refractory contractures not amenable to arthroscopic treatment.
- Steps include anterior and posterior capsulectomy, debridement of osteophytes/scar tissue, and restoration of functional ROM.
- Postoperatively: CPM + hourly ROM exercises + splinting at night for up to 12 weeks. (Campbell's Operative Orthopaedics, 15th ed)
- Joint replacement (arthroplasty) for severe OA or RA-related stiffness causing significant functional loss.
- Arthrodesis (joint fusion) in selected cases (e.g., index MCP joint in RA). (Miller's Review of Orthopaedics, 9th ed)
4. Special Situations
| Scenario | Key Treatment Consideration |
|---|---|
| Post-fracture stiffness | Early mobilization with internal fixation; physiotherapy immediately post-healing |
| Morning stiffness in RA | NSAIDs, DMARDs, anti-TNF therapy, modified-release corticosteroids |
| Frozen shoulder (adhesive capsulitis) | Physiotherapy, intra-articular steroids, hydrodilatation, manipulation, or arthroscopic release |
| Burn/scar contracture | Aggressive physiotherapy + splinting despite pain; surgery (scar excision, grafting) if severe |
| Sudeck's atrophy (CRPS) | Vigorous movement encouraged despite pain; thyrocalcitonin injections may shorten course |
| Adjacent joint stiffness (post external fixation) | PT first; surgical management in refractory cases |
Key Principles
- Early mobilization beats prolonged rest - the earlier physiotherapy begins, the better the outcome.
- Exercise is the foundation - ROM + strengthening + neuromuscular training.
- Pharmacotherapy enables exercise - use NSAIDs to control pain so patients can participate in therapy.
- Surgery is escalated stepwise: MUA → arthroscopic release → open release → arthroplasty.
- Older patients and those with pre-existing joint disease (RA, OA) are at higher risk and need earlier intervention.
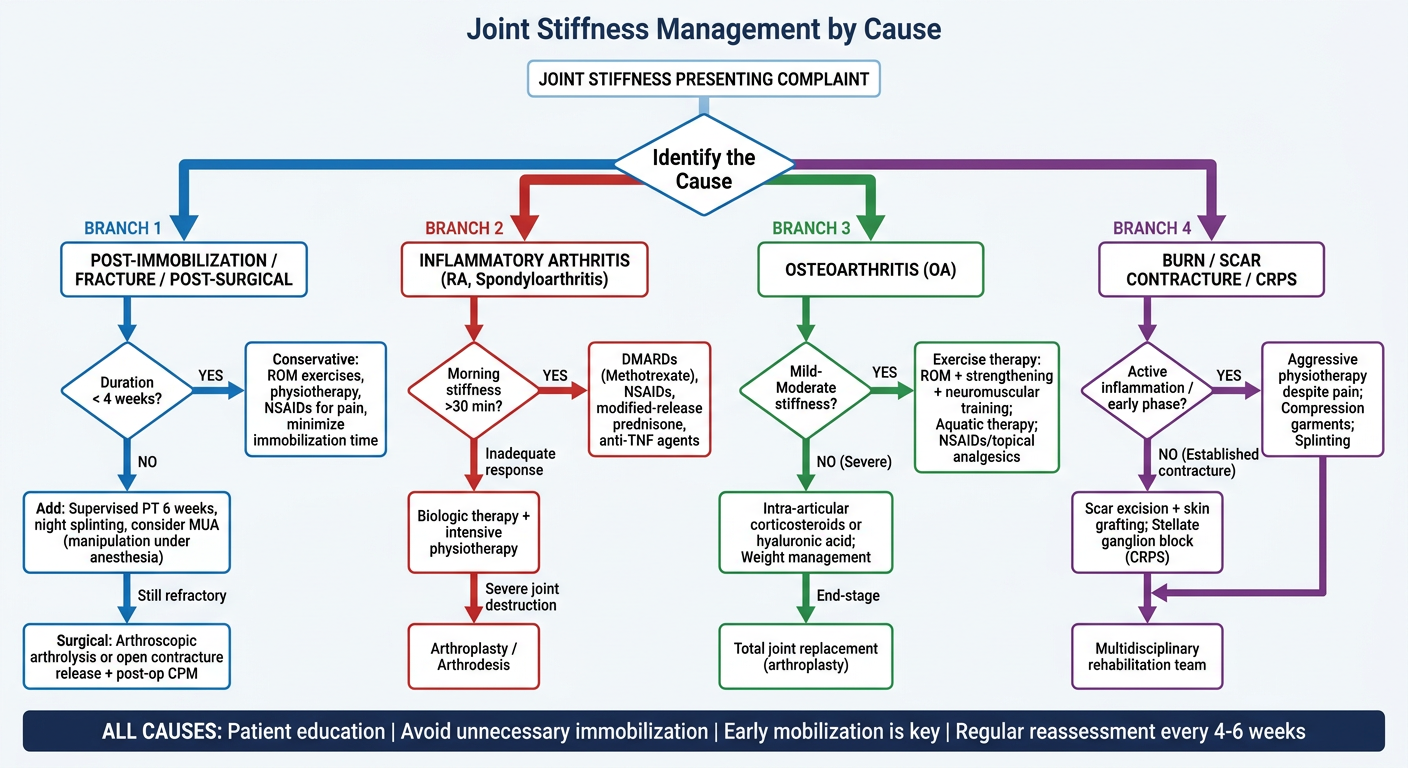
Create a clinical decision flowchart for stiffness management based on cause
A clinical decision flowchart titled "Joint Stiffness Management by Cause" on a clean white medical background. The flowchart starts at the top with a box "JOINT STIFFNESS PRESENTING COMPLAINT". Below it, a diamond decision box asks "Identify the Cause". From this diamond, 4 main branches flow downward: BRANCH 1 (far left, blue): "POST-IMMOBILIZATION / FRACTURE / POST-SURGICAL" → Box: "Duration < 4 weeks?" → YES → "Conservative: ROM exercises, physiotherapy, NSAIDs for pain, minimize immobilization time" → NO → "Add: Supervised PT 6 weeks, night splinting, consider MUA (manipulation under anesthesia)" → Still refractory → "Surgical: Arthroscopic arthrolysis or open contracture release + post-op CPM" BRANCH 2 (center-left, red): "INFLAMMATORY ARTHRITIS (RA, Spondyloarthritis)" → Box: "Morning stiffness >30 min?" → YES → "DMARDs (Methotrexate), NSAIDs, modified-release prednisone, anti-TNF agents" → Inadequate response → "Biologic therapy + intensive physiotherapy" → Severe joint destruction → "Arthroplasty / Arthrodesis" BRANCH 3 (center-right, green): "OSTEOARTHRITIS (OA)" → Box: "Mild-Moderate stiffness?" → YES → "Exercise therapy: ROM + strengthening + neuromuscular training; Aquatic therapy; NSAIDs/topical analgesics" → NO (Severe) → "Intra-articular corticosteroids or hyaluronic acid; Weight management" → End-stage → "Total joint replacement (arthroplasty)" BRANCH 4 (far right, purple): "BURN / SCAR CONTRACTURE / CRPS" → Box: "Active inflammation / early phase?" → YES → "Aggressive physiotherapy despite pain; Compression garments; Splinting" → NO (Established contracture) → "Scar excision + skin grafting; Stellate ganglion block (CRPS)" → All cases → "Multidisciplinary rehabilitation team" At the bottom, a shared footer box in dark navy: "ALL CAUSES: Patient education | Avoid unnecessary immobilization | Early mobilization is key | Regular reassessment every 4-6 weeks" Use color-coded boxes per branch, clean arrows, medical sans-serif font, professional clinical style.