Explain 10 heart dease and ecg emage with example
Reading File
Finding Sources
Searching the Web
ECG patterns 10 heart diseases examples images explained
Finding Sources
Loading Image
Loading Image
Finding Sources
Searching the Web
STEMI atrial fibrillation ventricular tachycardia heart block ECG images examples
Loading Image
Loading Image
Searching the Web
STEMI ECG example image site:litfl.com OR site:ecgwaves.com
Loading Image
Loading Image
Searching the Web
atrial flutter complete heart block Wolff-Parkinson-White long QT syndrome ECG image litfl
Loading Image
Loading Image
Now I have enough material to write a thorough, well-illustrated answer. Let me compile everything.
10 Heart Diseases and Their ECG Patterns
An ECG records the heart's electrical activity across time. Each disease leaves a recognizable fingerprint on the tracing. Below are 10 important heart diseases with their ECG features and real ECG examples.
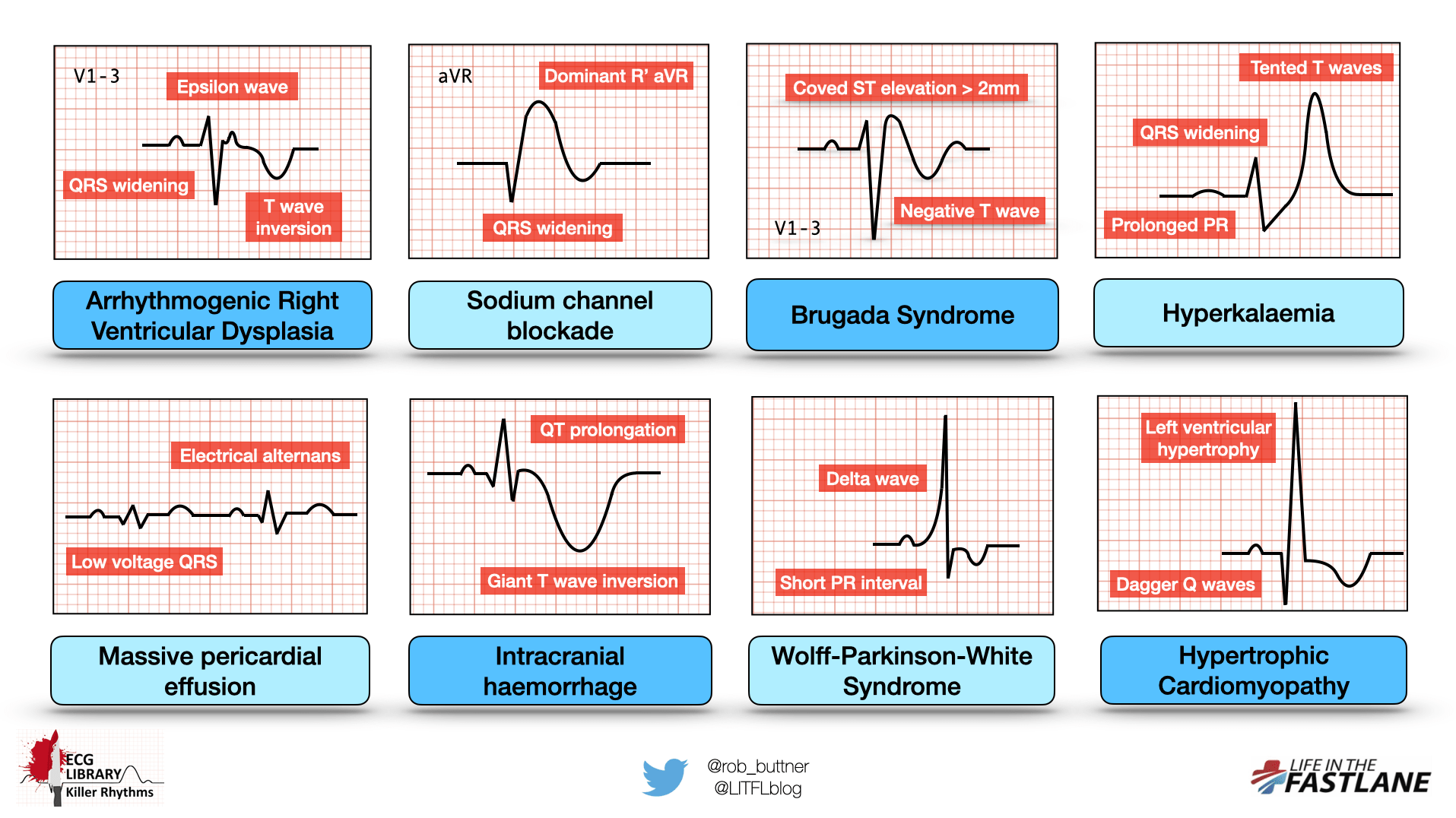
Quick Reference: Killer ECG Patterns
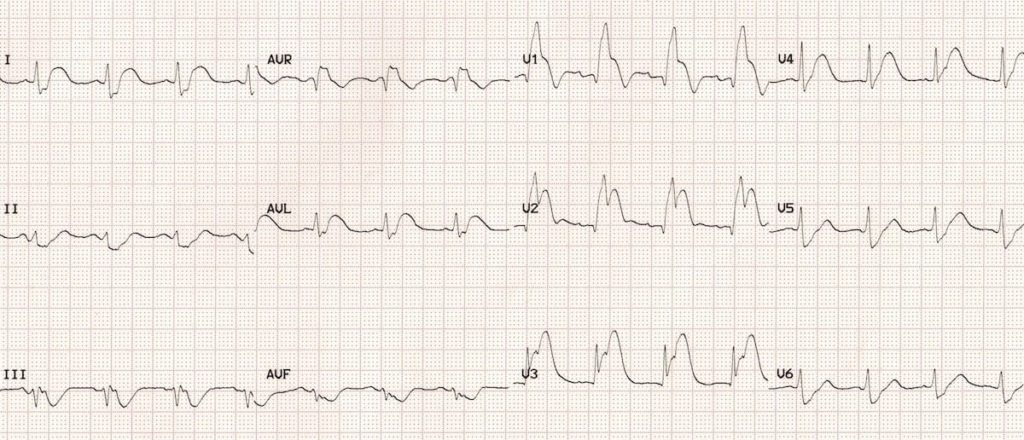
1. ST-Elevation Myocardial Infarction (STEMI)
What it is: A complete blockage of a coronary artery causing full-thickness (transmural) heart muscle death. The most time-critical cardiac emergency.
ECG findings:
- ST elevation ≥ 1 mm in 2 or more contiguous limb leads, or ≥ 2 mm in 2 or more contiguous precordial leads
- Hyperacute (tall, broad) T waves in the early phase
- Pathological Q waves develop later (sign of completed infarction)
- Reciprocal ST depression in opposite leads
Example: Anterior STEMI shows ST elevation in V2-V4, with reciprocal depression in inferior leads (II, III, aVF).
Clinical note: "Time is muscle" - every 30-minute delay in reperfusion leads to significant additional myocardial loss. Target door-to-balloon time is <90 minutes. - Tintinalli's Emergency Medicine
2. Atrial Fibrillation (AF)
What it is: Chaotic, disorganized electrical activity in the atria. The most common sustained cardiac arrhythmia, affecting ~2-3% of the general population.
ECG findings:
- No visible P waves (replaced by irregular fibrillatory baseline)
- Irregularly irregular RR intervals (the hallmark feature)
- Normal QRS complexes (unless aberrant conduction)
- Rate typically 100-160 bpm if uncontrolled

Risks: Stroke (5x increased risk), heart failure, hemodynamic compromise. Requires anticoagulation assessment using CHA₂DS₂-VASc score.
3. Atrial Flutter
What it is: A rapid, organized atrial circuit (usually in the right atrium) producing a regular atrial rate of ~300 bpm with variable conduction to the ventricles.
ECG findings:
- Classic "sawtooth" or "picket-fence" flutter waves at ~300 bpm in inferior leads (II, III, aVF)
- Flutter waves are upright in V1
- Ventricular rate is a regular fraction: 2:1 (150 bpm), 3:1 (100 bpm), or 4:1 (75 bpm)
- Regular QRS complexes
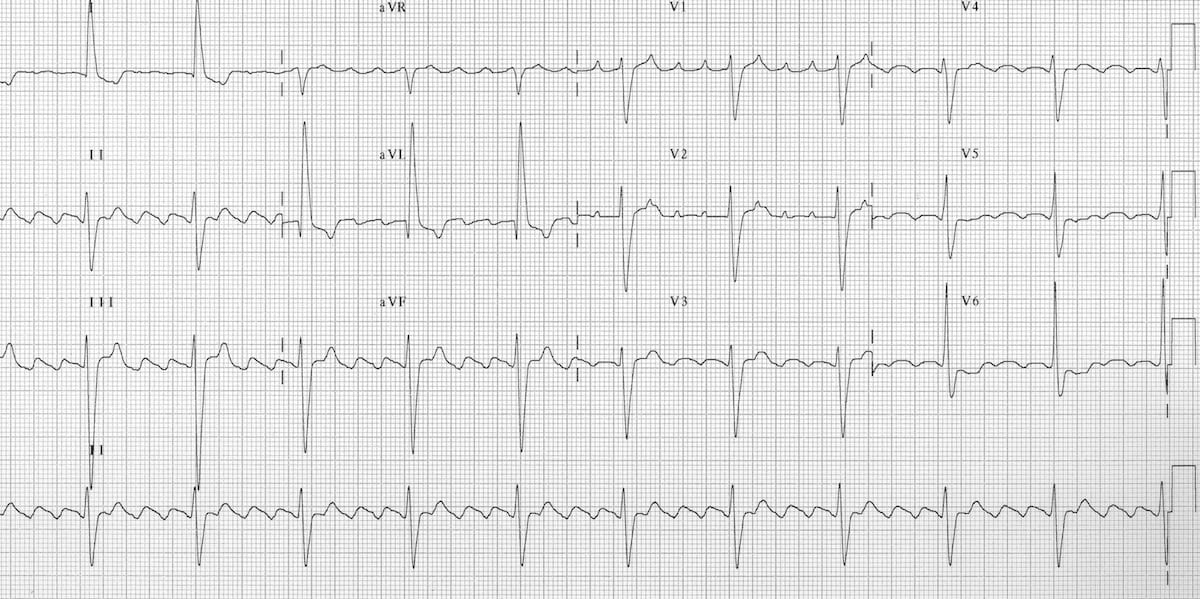
Tip: When you see a regular narrow-complex tachycardia at 150 bpm, always suspect 2:1 flutter until proven otherwise.
4. Ventricular Tachycardia (VT)
What it is: A life-threatening arrhythmia originating in the ventricles, running at ≥100 bpm. Can degenerate into ventricular fibrillation.
ECG findings:
- Wide QRS complexes (>120 ms) at rate 100-250 bpm
- AV dissociation (P waves independent of QRS - pathognomonic)
- Fusion beats and capture beats (when present, confirm VT)
- Concordance across all precordial leads
Example: A 45-year-old post-MI patient develops sudden palpitations and hypotension. ECG shows wide-complex tachycardia at 180 bpm with AV dissociation = VT until proven otherwise.
5. Ventricular Fibrillation (VF)
What it is: Chaotic, uncoordinated ventricular electrical activity - produces no effective cardiac output. Immediate cause of sudden cardiac death.
ECG findings:
- Completely chaotic, irregular waveforms with no identifiable P, QRS, or T waves
- Irregular amplitude and frequency
- No organized rhythm whatsoever
- Coarse VF (larger amplitude) vs. fine VF (smaller amplitude, worse prognosis)
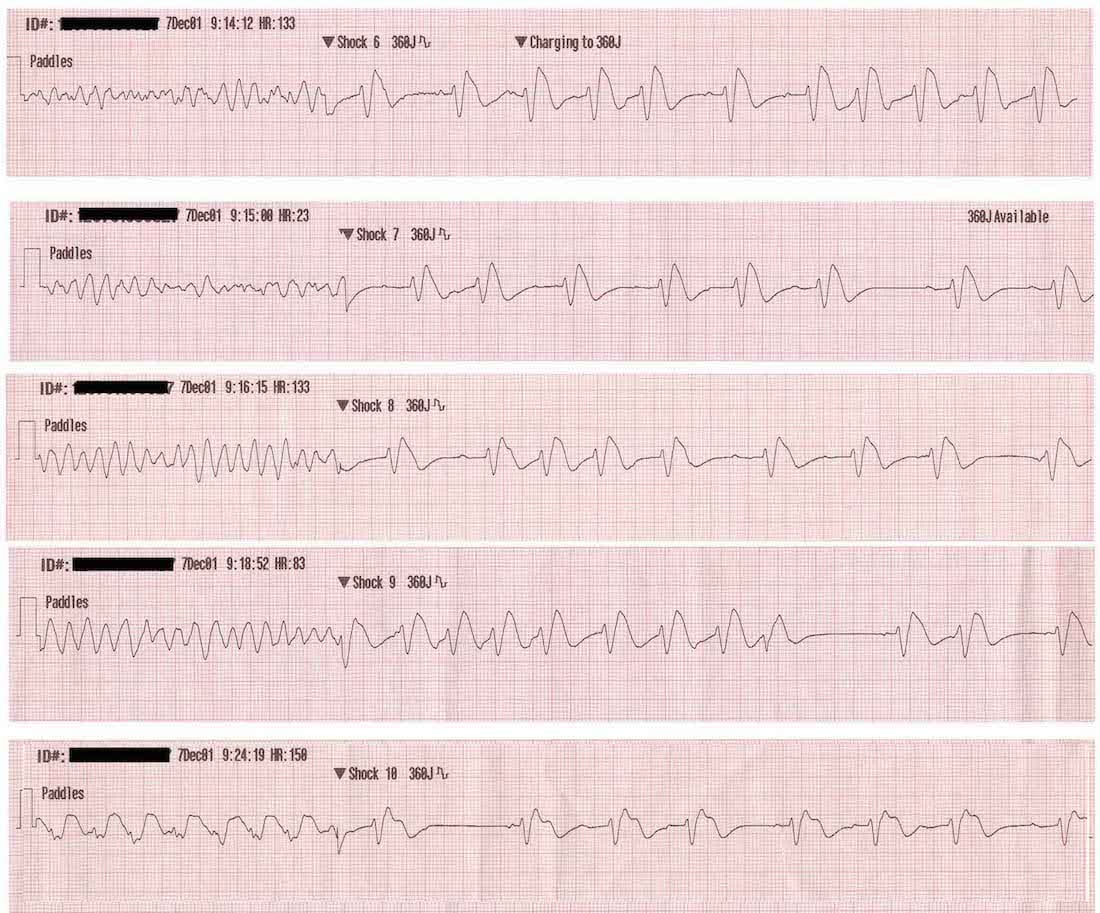
Management: Immediate defibrillation + CPR. Only shockable rhythm alongside pulseless VT. Survival falls ~10% per minute without defibrillation.
6. Complete (3rd Degree) Heart Block
What it is: Total failure of electrical conduction from atria to ventricles. The atria and ventricles beat independently of each other.
ECG findings:
- P waves present at normal atrial rate (~60-100 bpm)
- QRS complexes at a slower, independent ventricular escape rate (20-40 bpm if below His-Purkinje; 40-60 bpm if junctional)
- No relationship between P waves and QRS complexes (complete AV dissociation)
- Wide QRS if ventricular escape; narrow QRS if junctional escape
Example: An elderly patient presents with syncope. ECG shows P rate 80 bpm, QRS rate 35 bpm, with no relationship between them. Requires urgent pacemaker implantation.
7. Wolff-Parkinson-White (WPW) Syndrome
What it is: A congenital accessory pathway (Bundle of Kent) bypasses the AV node, causing ventricular pre-excitation and predisposing to tachyarrhythmias.
ECG findings (in sinus rhythm):
- Short PR interval (<120 ms) - fast conduction via accessory pathway
- Delta wave - slurred upstroke of the QRS (pre-excitation of ventricle)
- Wide QRS complex (>120 ms)
- ST-T wave changes secondary to abnormal depolarization
The infographic at the top of this article shows the classic delta wave and short PR interval pattern for WPW.
Danger: If AF develops with WPW, AV nodal blocking drugs (beta-blockers, verapamil, digoxin) are CONTRAINDICATED - they can precipitate VF. Use procainamide or cardioversion instead. - LITFL ECG Library
8. Brugada Syndrome
What it is: A genetic channelopathy (usually SCN5A sodium channel mutation) causing sudden cardiac death in young, otherwise healthy individuals with a structurally normal heart.
ECG findings (Type 1 - diagnostic):
- Coved-type ST elevation ≥2 mm in V1-V3
- Followed by a negative T wave (the "coved" pattern)
- QRS widening in right precordial leads
The top infographic clearly shows the classic coved ST elevation with negative T wave in V1-3 that defines Type 1 Brugada pattern.
Clinical pearls:
- May be unmasked by fever, sodium channel blockers (flecainide, procainamide), or tricyclic antidepressants
- Predominantly affects young Asian males
- Treatment for high-risk patients is an implantable defibrillator (ICD)
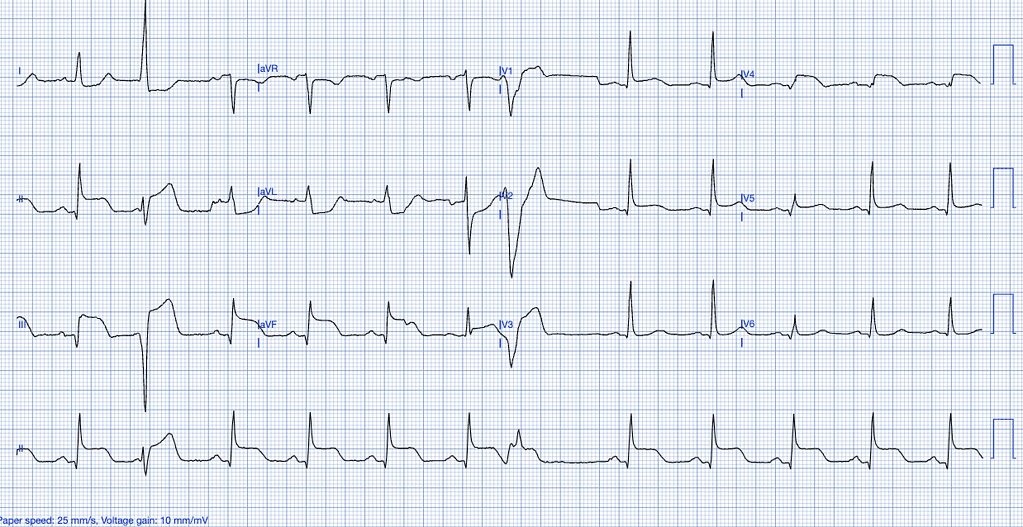
9. Left Ventricular Hypertrophy (LVH)
What it is: Thickening of the left ventricular muscle wall due to chronic pressure overload (e.g., hypertension, aortic stenosis).
ECG findings:
- Increased QRS voltage: S in V1 + R in V5 or V6 ≥35 mm (Sokolow-Lyon criteria)
- R in aVL ≥11 mm
- Left axis deviation
- "Strain pattern" - ST depression and T-wave inversion in lateral leads (I, aVL, V5-V6)
- Widened QRS (but usually <120 ms)
The first infographic shows LVH with "dagger Q waves" in hypertrophic cardiomyopathy - a more extreme form of hypertrophy.
Example: A 55-year-old hypertensive patient's ECG shows R+S voltage of 42 mm with ST depression in V5-V6 = LVH with strain.
10. Long QT Syndrome (LQTS)
What it is: Prolonged ventricular repolarization (congenital or acquired) that predisposes to a dangerous polymorphic VT called Torsades de Pointes.
ECG findings:
- Prolonged QT interval: corrected QTc >440 ms in males, >460 ms in females
- Abnormal T-wave morphology (notched, bifid, or biphasic T waves depending on subtype)
- QTc >500 ms carries highest risk of Torsades
- Torsades de Pointes: polymorphic VT with characteristic twisting of QRS axis around the baseline
Common causes of acquired LQTS:
| Cause | Examples |
|---|---|
| Drugs | Amiodarone, sotalol, haloperidol, erythromycin, methadone |
| Electrolytes | Hypokalemia, hypomagnesemia, hypocalcemia |
| Congenital | Romano-Ward syndrome (autosomal dominant), Jervell and Lange-Nielsen syndrome |
Rule of thumb: Always check QTc before prescribing QT-prolonging drugs. If QTc >500 ms, risk of Torsades is significant.
EKG Arrhythmia Reference
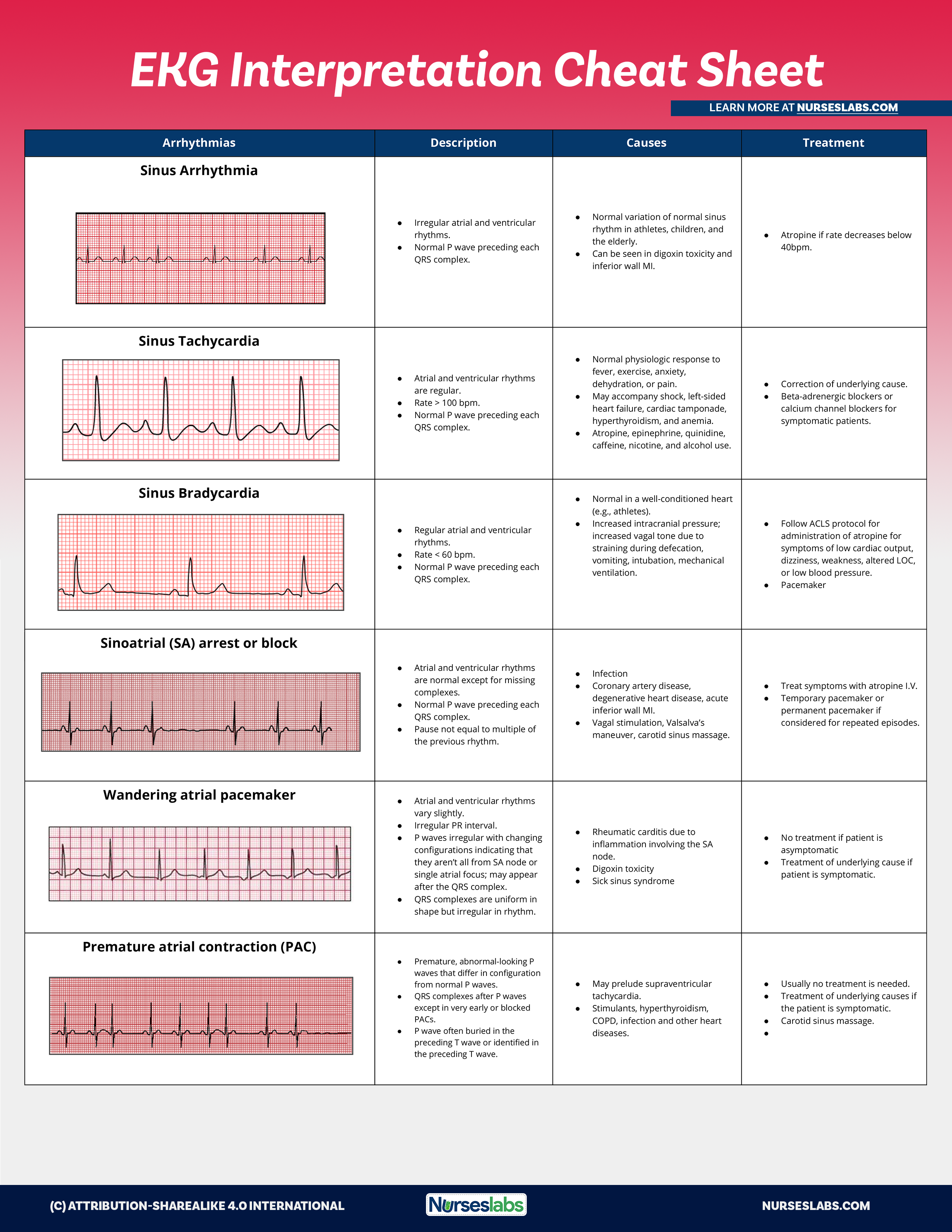
Summary Table
| # | Disease | Key ECG Feature | Rate | Rhythm |
|---|---|---|---|---|
| 1 | STEMI | ST elevation + Q waves | Normal/fast | Regular |
| 2 | Atrial Fibrillation | No P waves, irregular RR | 100-160 | Irregularly irregular |
| 3 | Atrial Flutter | Sawtooth flutter waves at 300 bpm | 75-150 | Regular |
| 4 | Ventricular Tachycardia | Wide QRS + AV dissociation | 100-250 | Regular |
| 5 | Ventricular Fibrillation | Chaotic, no identifiable complexes | Uncountable | None |
| 6 | Complete Heart Block | P waves & QRS independent | Atria 60-100, Ventricles 20-60 | Regular but dissociated |
| 7 | WPW Syndrome | Short PR + delta wave | Variable | Regular (in sinus) |
| 8 | Brugada Syndrome | Coved ST elevation V1-V3 | Normal | Regular |
| 9 | LVH | High voltage + strain pattern | Normal | Regular |
| 10 | Long QT Syndrome | Prolonged QTc >440 ms | Normal | Regular |
Sources: Braunwald's Heart Disease (Textbook of Cardiovascular Medicine), Tintinalli's Emergency Medicine, Goldman-Cecil Medicine, LITFL ECG Library, NursesLabs EKG Guide
This is a shared conversation. Sign in to Orris to start your own chat.