Thyroglossal cyst in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
thyroglossal duct cyst management surgery
Searching the Web
thyroglossal cyst RGUHS ENT 20 marks recent advances 2023 2024
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Here is your comprehensive RGUHS 20-mark answer on Thyroglossal Cyst:
THYROGLOSSAL DUCT CYST - A Comprehensive Review (20 Marks)
OUTLINE / SUBHEADINGS (RGUHS 20-mark pattern)
- Definition & Introduction
- Embryology & Applied Anatomy
- Pathology
- Classification
- Clinical Features
- Investigations
- Differential Diagnosis
- Treatment - Sistrunk's Operation (with steps)
- Complications
- Malignant Change
- Recent Advances
- Diagrams & Flowcharts
1. DEFINITION & INTRODUCTION
A thyroglossal duct cyst (TDC) is a congenital epithelium-lined cystic remnant of the thyroglossal duct, formed by incomplete obliteration of the duct through which the thyroid gland descends from the base of the tongue to its final position in the neck.
- Most common congenital cystic swelling of the neck (70% of all congenital neck masses)
- Incidence: ~7% of the general population have a persistent thyroglossal duct remnant
- Most commonly presents in children (first decade), but may present at any age
- Males = Females (slight male predominance in some series)
- Cummings Otolaryngology Head and Neck Surgery, p.3871; Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Vol 2, p.514
2. EMBRYOLOGY & APPLIED ANATOMY
Thyroid Descent Pathway
EMBRYOLOGICAL PATHWAY OF THYROID DESCENT
─────────────────────────────────────────────────────────────────
Week 3-4 of gestation:
Thyroid anlage forms at FORAMEN CECUM
(junction of anterior 2/3 and posterior 1/3 of tongue)
│
▼
Descends as a bilobed diverticulum
(= thyroglossal duct / tract)
│
▼
Passes ANTERIOR to hyoid bone (most common)
OR through/posterior to hyoid bone
(bifurcates extensively ABOVE hyoid bone)
│
▼
Reaches final position:
Isthmus at C5-C6 vertebral level
│
▼
Week 5-7: Duct NORMALLY OBLITERATES
│
▼
Failure of obliteration → THYROGLOSSAL DUCT CYST
─────────────────────────────────────────────────────────────────
Key anatomical points:
- The duct passes through or around the hyoid bone - this is WHY the central hyoid must be excised in Sistrunk's operation
- Extensive branching occurs above the hyoid bone - this explains why simple cystectomy leads to high recurrence
- The remnant tract elevates with tongue protrusion (attached to foramen cecum via muscle)
- Any abnormal cyst may arise anywhere along the tract and may contain thyroid tissue (Scott-Brown Vol 2, p.514)
- K.J. Lee's Essential Otolaryngology, p.1047; Scott-Brown Vol 2, p.514
3. SITES OF OCCURRENCE (Classification by Position)
SITES OF THYROGLOSSAL DUCT CYST (percentage distribution)
──────────────────────────────────────────────────────────
Intralingual / Lingual (base of tongue) — 2%
Suprahyoid — 25%
◄── AT THE LEVEL OF HYOID BONE — 15%
INFRAHYOID (most common) ◄──────────── — 65%
(Subhyoid to suprasternal notch)
Intratracheal (rare) — <1%
──────────────────────────────────────────────────────────
* 95% occur in MIDLINE; ~10% slightly to left side
| Site | Frequency |
|---|---|
| Infrahyoid (subhyoid) | Most common - 65% |
| At hyoid | 15% |
| Suprahyoid | 25% |
| Lingual / intralingual | Rare (2%) |
| Intratracheal / suprasternal | Very rare |
4. PATHOLOGY
Gross:
- Smooth, rounded, tense cystic swelling
- Usually 1-4 cm in diameter
- Contains mucoid/mucinous fluid (yellow or clear)
- Wall is thin and translucent
Microscopy:
- Lined by pseudostratified ciliated columnar epithelium (respiratory type) - most common
- Can also be stratified squamous, or cuboidal epithelium
- Wall contains thyroid follicles (in ~20-45% of cases)
- Chronic inflammation with fibrosis if previously infected
Pathological types:
- Simple thyroglossal cyst
- Thyroglossal sinus (opens to skin after spontaneous rupture/incision)
- Thyroglossal fistula (opening at both ends - rare)
- Cummings Otolaryngology, p.3871
5. CLINICAL FEATURES
Symptoms
- Painless midline neck swelling - most common presentation
- Becomes painful / tender when infected
- Dysphagia (if large or lingual type)
- Dyspnoea (rare, if large)
Signs - The Classic Triad:
CLASSIC SIGNS OF THYROGLOSSAL CYST
┌─────────────────────────────────────────────────────┐
│ 1. MIDLINE swelling (95%) / slightly left-sided │
│ (10%) in neck between hyoid & thyroid │
│ │
│ 2. Moves UPWARD on SWALLOWING │
│ (connected to pre-tracheal fascia & thyroid) │
│ │
│ 3. Moves UPWARD on TONGUE PROTRUSION │
│ ← PATHOGNOMONIC SIGN │
│ (tethered to foramen cecum via duct & muscle) │
└─────────────────────────────────────────────────────┘
Physical examination:
- Soft, cystic, non-tender (unless infected)
- Smooth, mobile, transilluminable
- Overlying skin normal (unless fistula present)
- Not attached to overlying skin (unless previously infected/drained)
- Moves superiorly with both swallowing AND tongue protrusion
Presentation variants:
- Infected cyst - red, tender, fluctuant; may rupture → thyroglossal sinus/fistula
- Lingual TDC - presents as base of tongue mass; dysphagia, snoring
- Infective episode often triggered by URI (upper respiratory tract infection)
- Scott-Brown Vol 2, p.514; Cummings, p.3871; K.J. Lee, p.1047
6. INVESTIGATIONS
INVESTIGATION ALGORITHM FOR THYROGLOSSAL CYST
──────────────────────────────────────────────────────────
CLINICAL DIAGNOSIS (midline cyst + tongue protrusion sign)
│
▼
ULTRASOUND NECK ◄─── FIRST-LINE INVESTIGATION
• Confirms diagnosis (anechoic/cystic mass, may show septa)
• Confirms NORMAL THYROID GLAND in orthotopic position
(Critical: if absent → cyst may be ONLY thyroid tissue!)
• Differentiates from dermoid (SIST score: septa, irregular
wall, solid components = TDC > dermoid)
│
▼
Normal thyroid seen?
┌─────YES──────┐ ┌──────NO──────────────┐
▼ │ ▼ │
Proceed to │ Radionuclide scan (Tc99m scan) │
surgery │ to confirm ectopic thyroid │
│ or absent thyroid │
└────────────────────────────────►┘
▼
TFTs (T3, T4, TSH)
Consider NOT excising
──────────────────────────────────────────────────────────
Other investigations:
| Investigation | Purpose |
|---|---|
| USG neck | First-line; confirms normal thyroid; cyst morphology |
| Tc-99m scan | Only if normal thyroid NOT seen on USG |
| FNAC | If malignancy suspected; cytology |
| CT/MRI neck | For recurrent or complex cysts; pre-revision surgery; intralingual TDC |
| TFTs | If orthotopic thyroid absent |
| Chest X-ray | Routine pre-op |
Note: Routine pre-operative TFTs or nuclear medicine are no longer routinely obtained if USG confirms normal thyroid. (Cummings, p.3871)
The SIST score (Sonographic Index of Sistrunk Technique): presence of septa, irregular wall, and solid components are more indicative of thyroglossal duct cyst than dermoid cyst. (K.J. Lee, p.9928)
- Scott-Brown Vol 2, p.514-515; Cummings, p.3871; K.J. Lee, p.1047
7. DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Feature |
|---|---|
| Dermoid cyst | Does NOT move with tongue protrusion; keratin-filled; does not transilluminate; doughy consistency |
| Subhyoid bursa | Directly in front of thyroid membrane; fluctuant |
| Enlarged delphian/pretracheal LN | Hard, multiple; associated with thyroid pathology |
| Ectopic thyroid | Solid; hypothyroidism; radionuclide uptake |
| Sebaceous cyst | Skin pit; foul-smelling; mobile with skin |
| Lipoma | Soft; lobulated; does not move with tongue protrusion |
| Branchial cyst | Lateral position (anterior to SCM); Baileys triangle |
| Ranula | Floor of mouth; plunging variety in submental region |
8. TREATMENT
A. Non-Surgical (temporary)
- For acutely infected cyst: antibiotics (amoxicillin-clavulanate), incision and drainage if needed
- Definitive surgery DEFERRED until infection resolves (6-8 weeks)
B. SISTRUNK'S OPERATION (Definitive Treatment)
Historical note: Described by Walter E. Sistrunk at the Mayo Clinic in 1920, published in Ann Surg 71(2):121-122, 1920. (Cummings, p.3879)
STEPS OF SISTRUNK'S OPERATION
SISTRUNK'S OPERATION - STEP BY STEP
═══════════════════════════════════════════════════════════════
PATIENT POSITION: Supine, neck extended, sandbag under shoulders
ANESTHESIA: GA with endotracheal intubation
INCISION: Transverse elliptical incision (Kocher/collar incision)
centered over the cyst in a skin crease
│
▼
STEP 1: Deepen incision through platysma
Raise superior and inferior flaps
│
▼
STEP 2: Identify and free the cyst
Handle gently - avoid rupture (increases recurrence)
│
▼
STEP 3: Trace duct SUPERIORLY toward hyoid bone
Stay in continuity with all tissue between strap muscles
│
▼
STEP 4: EXCISE CENTRAL PORTION OF HYOID BONE
← KEY STEP (rationale: duct passes through or around
hyoid; branches extensively at this level)
Divide hyoid on each side of midline
Preserve greater cornua bilaterally
│
▼
STEP 5: Continue dissection ABOVE hyoid
Follow core of tissue toward base of tongue
│
▼
STEP 6: Excise core of GENIOGLOSSUS MUSCLE
extending to FORAMEN CECUM
(ensures complete removal of all duct remnants)
│
▼
STEP 7: Suture tongue musculature (purse-string/interrupted)
Close in layers: muscle, platysma, skin
Suction drain placement (optional)
═══════════════════════════════════════════════════════════════
Rationale for hyoid excision: The thyroglossal duct passes through or is intimately related to the hyoid bone. Branches are extensively present at this level. Without hyoid excision, remnant duct tissue persists. (Scott-Brown Vol 2, p.514-515)
Recurrence rates:
- Simple excision alone: 46% recurrence
- Sistrunk's operation (modified): 5.8% recurrence (Cummings, p.3879)
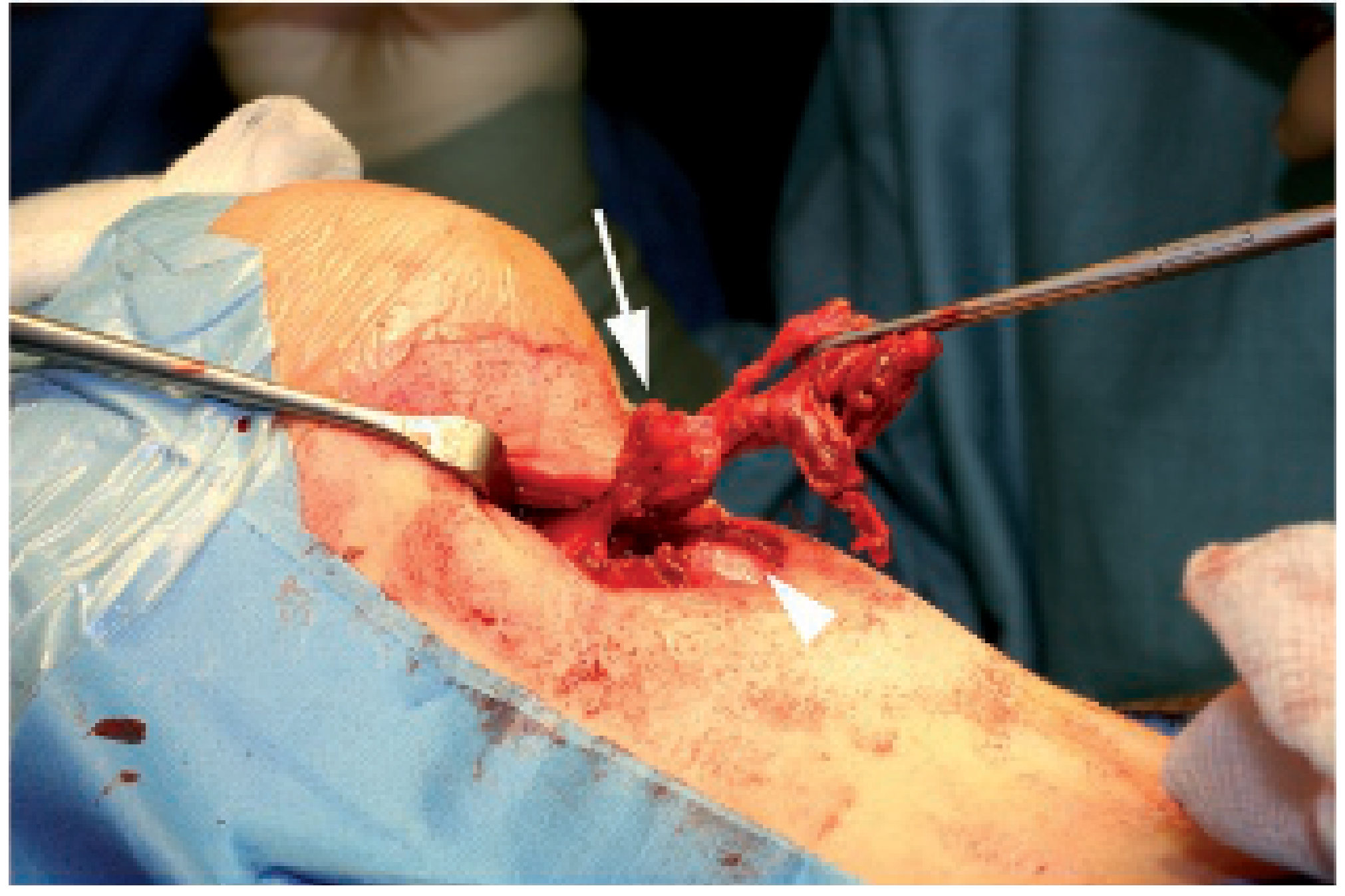
C. MODIFIED / EXTENDED SISTRUNK'S OPERATION
Developed for recurrent cases and now applied to all patients:
- Wider block dissection incorporating the infrahyoid region to thyroid isthmus
- Skin paddle excised if fistula present
- See intraoperative image below (Scott-Brown Fig 41.7)
9. COMPLICATIONS
Complications of the Disease:
- Infection - most common complication; may lead to abscess
- Sinus / Fistula formation - after spontaneous rupture or surgical drainage
- Malignant transformation - rare (see below)
Complications of Surgery (Sistrunk's):
| Complication | Notes |
|---|---|
| Recurrence | Most common (5-27% after modified Sistrunk; 46% after simple excision) |
| Haematoma | Early post-op |
| Seroma | Common |
| Salivary fistula | If pharyngotomy at foramen cecum not closed properly |
| Wound infection | |
| Hypoglossal nerve injury | Due to dissection above hyoid |
| Hypothyroidism | If cyst was the only thyroid tissue (not confirmed pre-op) |
| Scarring |
- Scott-Brown Vol 2, p.2374-2375
10. MALIGNANT CHANGE IN THYROGLOSSAL DUCT CYST
- Rare complication; incidence ~1% of all thyroglossal cysts
- Most common type: Papillary thyroid carcinoma (>85%)
- Also: follicular carcinoma, squamous cell carcinoma (from squamous epithelium)
- Associated 6.6% risk of microcarcinoma in the normal-appearing thyroid gland
Criteria for diagnosis (Batchelor-Bhatt criteria):
- Normal thyroid tissue in the cyst wall
- Smooth transition from normal to malignant tissue
- No similar lesion elsewhere (i.e., not a metastasis to the cyst)
Management of malignant TDC:
MANAGEMENT ALGORITHM - MALIGNANT THYROGLOSSAL DUCT CYST
─────────────────────────────────────────────────────────────
Diagnosed malignancy in TDC
│
▼
Sistrunk's operation (adequate local excision)
│
┌──────┴──────────────────────────────────┐
▼ ▼
PAPILLARY Ca (most common) FOLLICULAR Ca / SCC
│ │
▼ ▼
Evaluate normal thyroid Total thyroidectomy
by USG + FNAC + RAI therapy
│
▼
Thyroidectomy NOT automatically
required (Cummings 2023 guidelines)
Monitor thyroid for life
(6.6% microcarcinoma risk in thyroid)
─────────────────────────────────────────────────────────────
- Cummings Otolaryngology, p.3872-3873; Cummings block26 (TDC carcinoma)
Recent systematic review (Thimsen et al., Virchows Arch 2025, PMID 40347268): Thyroglossal duct cyst carcinomas have indolent behavior; Sistrunk's alone sufficient for most papillary carcinomas without high-risk features.
11. RECENT ADVANCES (2020-2026)
A. Sclerotherapy as Alternative to Surgery
- Systematic review (Talmor et al., Otolaryngol Head Neck Surg, 2021, PMID 33755513): Sclerotherapy with agents such as OK-432 (picibanil), bleomycin, or ethanol reported for benign cystic head and neck lesions including TDC
- Reserved for poor surgical candidates or recurrent cysts
- Overall success rates variable; not yet standard of care
B. Endoscopic / Minimally Invasive Approaches
- Endoscopic management of intralingual TDC (Pereira NM et al., Auris Nasus Larynx, 2023, PMID 35659788): Systematic review of case series; transoral endoscopic excision feasible for selected intralingual cysts
- Robotic-assisted and endoscopic remote-access Sistrunk's being explored in adults for better cosmesis (limited evidence)
C. SIST Score - Preoperative USG Scoring
- SIST score: Sonographic scoring system on ultrasound to differentiate TDC from dermoid cyst preoperatively
- Variables: septa, irregular wall, solid components - higher score = more likely TDC
- Guides surgical planning and consent (K.J. Lee, p.9928)
D. Role of Pre-op Imaging
- 2025 systematic review (Taishan W et al., J Med Life 2025, PMID 40757114): Thyroid scan and ultrasound are complementary; USG alone is sufficient in most cases; radionuclide scan reserved for when normal thyroid cannot be confirmed on USG
E. TDC Carcinoma - Updated Guidelines
- Thyroidectomy is NOT mandated for incidental papillary TDC carcinoma (Cummings 7th ed.)
- Active surveillance/monitoring protocol for thyroid gland post-Sistrunk's
- Systematic review (Thimsen 2025, Virchows Arch, PMID 40347268): Retrospective study and review confirms excellent prognosis; low-risk papillary TDC Ca managed by Sistrunk's alone
F. Multiple Thyroglossal Duct Cysts
- Rare entity reported (Bao YY et al., Ear Nose Throat J 2025, PMID 37194164): multiple simultaneous TDCs; may require modified extended Sistrunk's covering entire tract
G. Extended / Modified Sistrunk's - Now Standard
- Extended Sistrunk's (block dissection to thyroid isthmus) previously reserved for recurrent cases is now increasingly used as primary procedure to minimize recurrence
- [Scott-Brown's, p.2370-2375]
12. SUMMARY FLOWCHART - COMPLETE MANAGEMENT
THYROGLOSSAL CYST - MANAGEMENT FLOWCHART
══════════════════════════════════════════════════════════════
MIDLINE NECK SWELLING
│
▼
Moves UP with tongue protrusion?
YES ────────────────────────► NO → Consider dermoid,
│ subhyoid bursa,
▼ enlarged LN
CLINICAL DIAGNOSIS: TDC
│
▼
┌──────── INVESTIGATIONS ─────────┐
│ USG Neck (FIRST-LINE) │
│ → Is normal thyroid present? │
│ YES NO │
│ │ │ │
│ │ Tc99m scan + TFTs │
│ │ If only thyroid → │
│ │ Do NOT excise │
└─────────────────────────────────┘
│
▼
Currently INFECTED?
YES ──────────────────────────► Antibiotics ± I&D
│ Wait 6-8 weeks
│ NO (or after resolution)
▼
┌────────────────────────────────────┐
│ SISTRUNK'S OPERATION │
│ - Elliptical incision over cyst │
│ - Dissect cyst en bloc │
│ - Excise central hyoid bone │
│ - Core of genioglossus muscle │
│ up to foramen cecum │
│ - ± Extended dissection │
└────────────────────────────────────┘
│
▼
HISTOPATHOLOGY
│
┌──────────┴──────────┐
│ │
BENIGN MALIGNANT
│ │
▼ ▼
Discharge Papillary Ca → Monitor thyroid
+ Follow-up (Sistrunk's sufficient in most)
Follicular/SCC → Total thyroidectomy
══════════════════════════════════════════════════════════════
13. KEY ANATOMICAL DIAGRAM
ANATOMY OF THYROGLOSSAL DUCT - SCHEMATIC
════════════════════════════════════════════════════════
TONGUE (dorsum)
│
[FORAMEN CECUM] ◄── Origin of thyroglossal duct
│
│ Suprahyoid segment
│ (extensive branching ← reason for wide resection)
│
[HYOID BONE] ◄──── Central portion excised in Sistrunk's
│
│ Infrahyoid segment
│ ← MOST COMMON SITE OF CYST FORMATION
│
[THYROID ISTHMUS]
│
[PYRAMIDAL LOBE] ◄── Remnant of descent in 50%
Sites of cyst formation: ● = possible location of cyst
Lingual (rare) ●
Suprahyoid ●●
At hyoid ●●●
Infrahyoid ●●●●●●● (most common)
Suprasternal (rare) ●
════════════════════════════════════════════════════════
SOURCES CITED
| Textbook | Key Contribution |
|---|---|
| Cummings Otolaryngology HNS (7th ed.) | Sistrunk recurrence rates, malignancy management, TFT guidelines |
| Scott-Brown's Otorhinolaryngology HNS Vol 2 | Presentation, Sistrunk's steps, extended Sistrunk, intraoperative anatomy |
| K.J. Lee's Essential Otolaryngology (KJ Lee, equivalent to Stell & Maran level of detail) | Clinical features, SIST score, treatment algorithm |
| Bailey & Love's | Sistrunk's operation description |
| Sabiston Textbook of Surgery | Sistrunk procedure (first described 1928/1920) |
Recent Articles:
- Talmor et al. 2021 - Sclerotherapy for cystic head & neck lesions (PMID 33755513)
- Pereira et al. 2023 - Endoscopic management of intralingual TDC (PMID 35659788)
- Taishan et al. 2025 - Thyroid scan and USG in TDC management (PMID 40757114)
- Thimsen et al. 2025 - TDC carcinomas systematic review (PMID 40347268)
- Bao et al. 2025 - Multiple TDCs review (PMID 37194164)
EXAM TIPS FOR RGUHS 20 MARKS
Expected coverage (allocate marks roughly as follows):
| Section | Marks |
|---|---|
| Definition + Embryology + Anatomy | 3 |
| Pathology (gross + micro) + Classification | 2 |
| Clinical features (signs, symptoms, triad) | 3 |
| Investigations (algorithm, USG importance) | 2 |
| Differential diagnosis | 1 |
| Treatment (Sistrunk's operation in detail - steps, rationale for hyoid excision, recurrence data) | 5 |
| Complications (disease + surgery) | 2 |
| Malignancy in TDC | 1 |
| Recent advances | 1 |
| Total | 20 |
Do NOT miss these key examinable points:
- Sistrunk's operation - the central hyoid must be excised and why
- Recurrence 46% (simple excision) vs 5.8% (Sistrunk's)
- Tongue protrusion sign is pathognomonic
- USG must confirm normal thyroid before surgery
- Most common histology in malignant TDC = papillary carcinoma
- First described by Sistrunk in 1920 (Mayo Clinic)
- Most common site = infrahyoid (subhyoid)
This is a shared conversation. Sign in to Orris to start your own chat.