Types of perforation of the tympanic membrane
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative ENT textbooks. Let me compile the full answer.
Types of Perforation of the Tympanic Membrane
Tympanic membrane (TM) perforations are classified by location, size, etiology, and activity. The most clinically important classification is by location, as this determines the risk of complications.
1. Classification by Location
A. Central Perforation
- Located in the pars tensa, with a rim of intact TM surrounding the perforation on all sides - the annulus is not involved
- The margins do not reach the bony annular sulcus
- Associated with tubotympanic (mucosal) chronic otitis media (COM)
- Also called "safe" perforation - complications are rare
- Discharge (when present): profuse, mucoid, odorless, responds to conservative treatment
- Hearing loss is usually mild and purely conductive
Sub-types by quadrant:
- Anterior
- Posterior
- Inferior
- Subtotal (involving most of pars tensa but sparing the annulus)
B. Marginal Perforation
- The edge of the perforation involves or reaches the bony annulus (fibrocartilaginous rim)
- Most commonly in the posterior or posterosuperior quadrant of the pars tensa, or in the pars flaccida (attic)
- Associated with atticoantral (squamous) COM and cholesteatoma
- Called "unsafe" - high risk of complications (brain abscess, facial palsy, labyrinthitis, etc.)
- Discharge: thick, scanty, foul-smelling, resistant to conservative treatment
Important sub-types:
- Attic (pars flaccida) perforation - superiorly located; in reality often a retraction pocket; associated with pars flaccida cholesteatoma; causes erosion of scutum and medialization of ossicular chain on CT
- Posterosuperior marginal perforation - of the pars tensa; associated with pars tensa cholesteatoma; erodes the long process of incus/stapes; lateralization of ossicular chain on CT (scutum intact)
Shambaugh notes that these "perforations" in the pars flaccida and posterosuperior quadrant are in reality retraction pockets - comparable to the inverted finger of a surgical glove - with the blind distal end lying deep in the middle ear space, hidden by overlying bone.
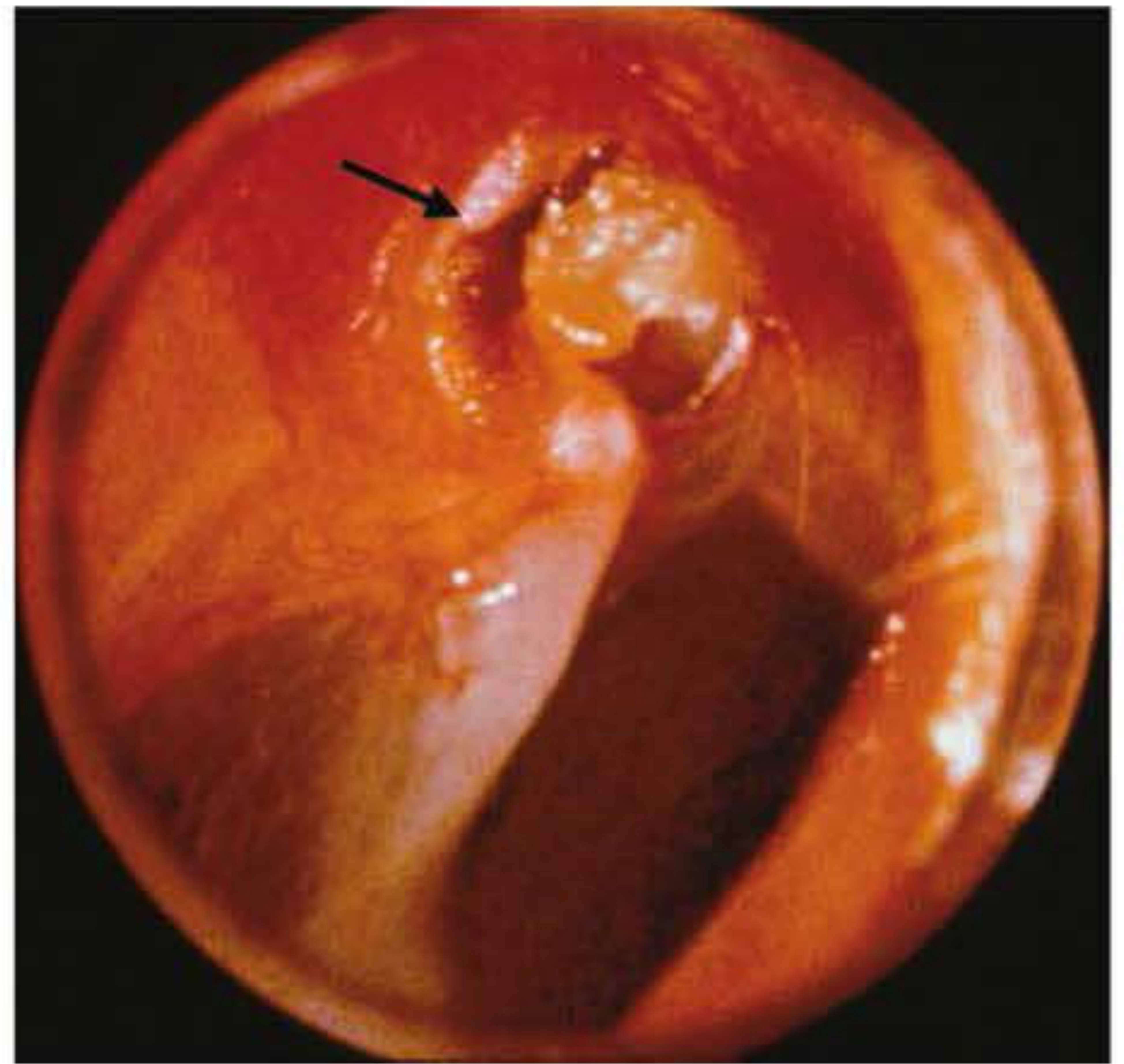
FIGURE 26-13: "Perforation" of the pars flaccida (arrow). - Shambaugh Surgery of the Ear
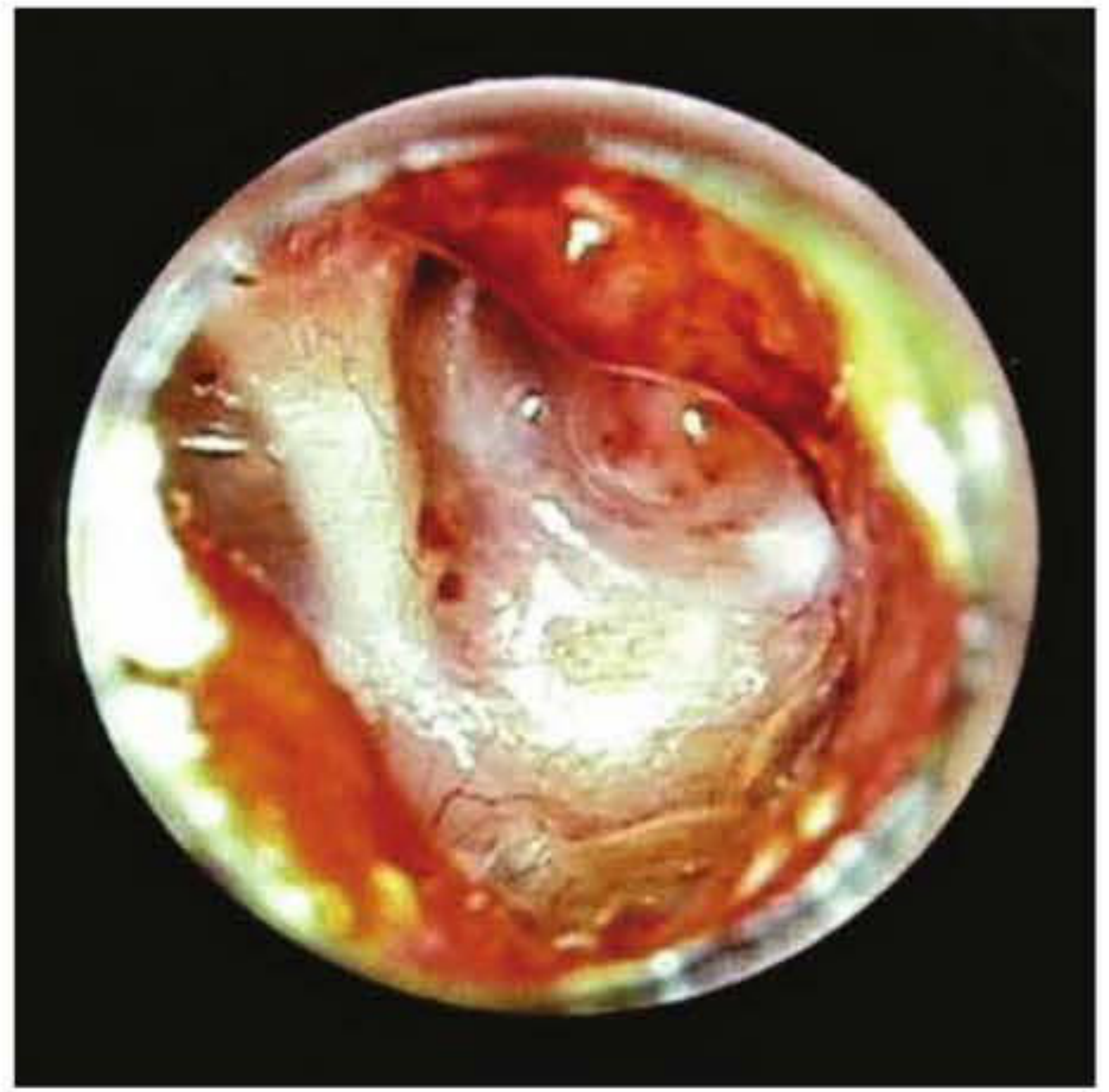
FIGURE 26-14: "Perforation" of pars tensa, posterosuperior quadrant. - Shambaugh Surgery of the Ear
2. Classification by Size
| Size | Approximate Area of TM Involved |
|---|---|
| Small | <25% |
| Medium | 25-50% |
| Large | 50-75% |
| Subtotal | >75% (annulus intact) |
| Total | Entire pars tensa including annulus |
Hearing loss increases with perforation size and is greatest at low frequencies. A large perforation can cause up to 40-50 dB air-bone gap. The degree of hearing loss also depends on middle ear/mastoid air volume - a sclerotic mastoid with small air volume produces a larger gap than a well-pneumatized one (Shambaugh Surgery of the Ear).
3. Classification by Etiology
A. Traumatic Perforation
- Blunt trauma (slap, blast), barotrauma, penetrating injury, lightning strike, iatrogenic (syringing, foreign body removal)
- Almost always in the pars tensa, typically anteriorly or inferiorly
- Pars tensa is only a few cell layers thick and easily torn
- Symptoms: acute pain, hearing loss, ± bloody otorrhoea, vertigo, tinnitus
- Most heal spontaneously; ~90% close without intervention (Tintinalli's Emergency Medicine)
- Posterosuperior or penetrating trauma perforations carry higher risk of ossicular chain damage
B. Infective Perforation
- Secondary to acute otitis media (AOM): spontaneous rupture occurs in ~5% of AOM cases; nontypeable H. influenzae most common pathogen in children; typically heals without additional intervention (K.J. Lee's Essential Otolaryngology)
- Secondary to chronic otitis media (COM): hallmark of chronic disease; repair depends on healthy Eustachian tube function
4. Classification by Activity (Scott-Brown's COM Classification)
| Type | Synonym | Otoscopic Finding |
|---|---|---|
| Healed COM | Tympanosclerosis | Thinning/opacification of pars tensa, no perforation |
| Inactive (mucosal) COM | Perforation | Permanent perforation of pars tensa; middle ear mucosa not inflamed |
| Inactive (squamous) COM | Retraction | Retraction of pars flaccida or posterosuperior pars tensa; potential for debris retention |
| Active (mucosal) COM | - | Pars tensa defect with inflamed mucosa producing mucopus |
| Active (squamous) COM | Cholesteatoma | Pars flaccida or tensa retraction with retained squamous debris and inflammation |
(Scott-Brown's Otorhinolaryngology, Table 83.1)
5. "Safe" vs. "Unsafe" - The Classic Clinical Dichotomy
| Feature | Tubotympanic (Safe) | Atticoantral (Unsafe) |
|---|---|---|
| Perforation location | Pars tensa (central) | Pars flaccida / posterosuperior pars tensa (marginal) |
| Discharge | Profuse, mucoid, odorless | Scanty, thick, foul-smelling |
| Cholesteatoma | Extremely rare | Common |
| Complications | Rare | Frequent (meningitis, brain abscess, facial palsy, labyrinthitis) |
| Hearing loss | Mild conductive | Larger conductive ± SNHL |
| CT findings | Middle ear haziness | Scutum erosion (pars flaccida type); lateralized ossicular chain (pars tensa type) |
(Shambaugh Surgery of the Ear, Table 26-2)
Key Clinical Points
- Perforations should be described by clock face position and whether they involve the annulus (central vs. marginal) - Cummings Otolaryngology
- Marginal perforations (especially posterosuperior) have a greater likelihood of ossicular chain damage and should be referred to an otolaryngologist within 24 hours - Tintinalli's Emergency Medicine
- The volume of the middle ear and mastoid air space is an important determinant of the degree of hearing loss - identical perforations can cause 20-30 dB different air-bone gaps if mastoid pneumatization differs - Shambaugh Surgery of the Ear
This is a shared conversation. Sign in to Orris to start your own chat.