I have pain in my ankle joint and its more intense when I invert my foot
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ankle sprain"[MeSH Terms] AND "lateral ligament"
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Here is a thorough breakdown of your ankle pain based on authoritative medical sources:
Ankle Pain Worsened by Inversion
Pain in the ankle joint that intensifies with inversion of the foot is the classic hallmark of lateral ankle ligament injury (sprain). This is the most common ankle injury, accounting for 85% of all ankle sprains. - Campbell's Operative Orthopaedics 15th Ed 2026
Anatomy of the Lateral Ankle
The lateral side of your ankle is stabilized by three ligaments:
| Ligament | Abbreviation | Function | Strength |
|---|---|---|---|
| Anterior talofibular ligament | ATFL | Resists forward sliding of the talus; restricts inversion when ankle is plantarflexed | Weakest - most commonly torn |
| Calcaneofibular ligament | CFL | Restricts inversion when ankle is in neutral/dorsiflexed position | Moderate |
| Posterior talofibular ligament | PTFL | Resists backward translation of the talus | Strongest - rarely torn alone |
The ATFL is the most commonly injured because most ankle sprains happen when the foot rolls inward while slightly pointed down (plantarflexed). - Campbell's Operative Orthopaedics 15th Ed 2026
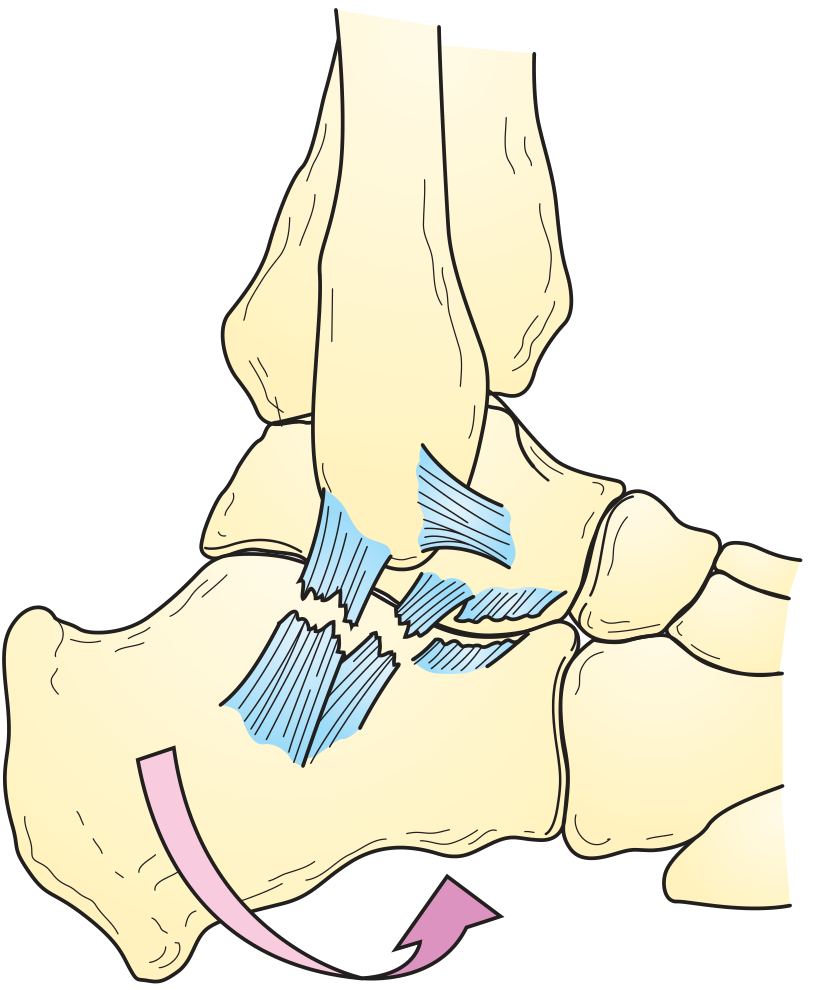
Forceful inversion causing tearing of the lateral ankle ligaments (ATFL and CFL shown in blue)
Grading of the Sprain
| Grade | What Happened | Symptoms |
|---|---|---|
| Grade I | No actual ligament tearing (stretching only) | Mild pain, minimal swelling, able to bear weight |
| Grade II | Partial tear | Moderate pain, swelling, bruising, difficulty bearing weight |
| Grade III | Complete tear | Severe pain, major swelling, bruising, unable to bear weight, ankle feels unstable |
- Tintinalli's Emergency Medicine - A Comprehensive Study
Clinical Tests Your Doctor Will Perform
- Anterior drawer test - foot slightly plantarflexed, the talus is pulled forward to test ATFL integrity
- Talar tilt test (inversion stress test) - ankle in neutral position, talus tilted inward to test CFL
- Both tests compare movement and "end-point feel" with your other ankle to gauge severity
- Textbook of Family Medicine 9e
Do You Need an X-Ray? (Ottawa Ankle Rules)
An X-ray is recommended if you have any of the following:
- Age under 18 or over 55
- Unable to take 4 steps immediately after injury or in the clinic
- Tenderness over the back edge (posterior 6 cm) or tip of the fibula (outer ankle bone)
- Tenderness over the medial malleolus (inner ankle bone)
- Tenderness at the base of the 5th metatarsal (outer midfoot) - Rosen's Emergency Medicine; Textbook of Family Medicine 9e
Treatment - PRICE Protocol
Immediate management follows the PRICE protocol:
- Protection - ankle brace or splint to prevent further inversion
- Rest - reduce weight-bearing activity (up to 72 hours)
- Ice - apply ice packs to reduce swelling
- Compression - elastic bandage wrap
- Elevation - keep the ankle raised above heart level
After 48-72 hours, a 3-phase rehabilitation approach is recommended:
- Phase 1: Continue PRICE
- Phase 2: Range-of-motion and strengthening exercises
- Phase 3: Balance/proprioception training, sport-specific conditioning
Research favors early functional treatment (getting moving early) over prolonged immobilization - patients mobilize 4-7 days sooner with functional treatment. - Tintinalli's Emergency Medicine
Other Conditions to Consider
If pain is chronic or didn't follow a specific injury, other causes include:
- Peroneal tendon injury - pain slightly posterior to the lateral malleolus, worsens with resisted eversion
- Sinus tarsi syndrome - lateral heel pain, feeling of instability, often after recurrent sprains
- Osteochondral lesion of the talus - deep joint pain, especially if associated with catching or locking
- Fracture - avulsion fracture of the 5th metatarsal base or lateral process of the talus can mimic a sprain (Ottawa rules help rule this out)
When to See a Doctor Urgently
- Significant swelling and bruising within hours
- Inability to bear weight at all
- Visible deformity
- Numbness or tingling in the foot
- Pain that is not improving after several days of rest
Disclaimer: This information is educational and based on authoritative medical textbooks. It is not a substitute for an in-person clinical evaluation. Please see a doctor or physiotherapist for a proper diagnosis and individualized treatment plan.
I have no swelling and bruising the pain has veen there for months and it also hurts when yhe foot is relaxed like when am in bed or in the car
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
The updated symptom picture is very helpful. Here is a refined analysis:
Revised Assessment: Chronic Ankle Pain (Months Duration, No Swelling, Rest Pain)
Your updated symptoms change the picture significantly:
- No swelling or bruising - rules against active ligament sprain
- Months of duration - this is a chronic condition, not acute injury
- Pain at rest (in bed, in a car) - this is an important "red flag" feature that points beyond simple mechanical/soft-tissue causes
Most Likely Diagnoses
1. Sinus Tarsi Syndrome (High probability)
The sinus tarsi is a small canal on the outer side of the ankle between the talus and calcaneus. Pain here often persists for months to years after an ankle sprain, even when swelling has completely resolved.
Key features:
- Persistent lateral ankle/hindfoot pain without obvious swelling
- Feeling of ankle instability or giving way
- Pain localized to the outer front of the heel/ankle area
- Worsened by inversion and weight-bearing
- Often develops from scarring, fat atrophy, or ligament damage inside the sinus tarsi canal
- MRI arthrogram can identify tears of the interosseous talocalcaneal and cervical ligaments
Diagnosis confirmed if injection of local anesthetic + cortisone into the sinus tarsi relieves the pain - this is both diagnostic and often curative. - Campbell's Operative Orthopaedics 15th Ed 2026
2. Osteochondral Lesion of the Talus (OLT) - Important to exclude
This is a very common cause of persistent deep ankle pain that is frequently missed, particularly after trauma.
- Damage to the cartilage and underlying bone of the talar dome
- Can cause rest pain and night pain because the bone is involved
- Often no visible swelling externally despite significant internal damage
- Most occur after trauma, but some medial lesions arise without any injury history
- Easily missed on plain X-rays - MRI is required for diagnosis
- MRI shows subchondral cysts, bone marrow edema, and whether the lesion is stable or loose
"Osteochondral lesions (OCLs) of the talar dome are a common cause of persisting deep ankle pain... OCLs are easily missed on plain radiographs, but MRI is very sensitive." - Grainger & Allison's Diagnostic Radiology
3. Peroneal Tendon Pathology (Moderate probability)
The peroneal tendons run just behind and below the outer ankle bone (lateral malleolus).
- Chronic subluxation or tendon tears are frequently misdiagnosed as ankle sprain
- Only 60% are correctly diagnosed at the first visit - Campbell's Operative Orthopaedics 15th Ed 2026
- Pain is lateral, posterior to the fibula
- Can develop without a specific traumatic event
- More common in younger athletic individuals
4. Tarsal Coalition (Worth considering, especially if younger)
Abnormal bony or cartilaginous fusion between two hindfoot bones (e.g. calcaneus and talus). This causes a rigid, painful hindfoot that is made worse by inversion and can produce chronic, background aching.
5. Ankle/Subtalar Impingement
Bony spurs or soft-tissue pinching inside the joint, causing pain in certain positions - including at rest when the ankle is in a relaxed plantarflexed position (exactly as when lying in bed or sitting in a car). - Grainger & Allison's Diagnostic Radiology
Why Rest Pain Matters
Pain that persists when the foot is completely relaxed and non-weight-bearing is an important feature. It suggests one of:
| Cause | Why Rest Pain Occurs |
|---|---|
| Osteochondral lesion / bone damage | Bone contains pain nerve fibers active even at rest |
| Intra-articular pathology (synovitis, impingement) | Joint fluid pressure and inflammation persist at rest |
| Nerve irritation | Nerve pain does not require movement |
| Rarely: bone tumor/infection | Constant pain, especially at night |
What You Need
Given months of pain with rest symptoms, you need a proper clinical workup:
- MRI of the ankle - this is the most important investigation. It will identify OLT, sinus tarsi changes, peroneal tendon tears, synovitis, and ligament damage that X-rays will miss.
- X-ray (weight-bearing) - can show bone spurs, coalition, or fractures
- Physical examination by an orthopaedic surgeon or sports medicine doctor - including palpation of the sinus tarsi, peroneal tendons, and stress testing
Important: Rest pain lasting months without prior injury investigation is a reason to see a doctor promptly. While most causes are benign mechanical conditions, persistent bone pain at rest should always be properly evaluated to exclude rarer but serious causes. Please consult an orthopaedic specialist or musculoskeletal physician for a formal assessment and imaging.
I went for xray and nothing was seen and sometimes I feel the same issues in the opposite side of the joint
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
This new information is a major turning point in your symptom picture. Here is a clear, updated assessment:
Critical Update: This Is Likely a Systemic Condition
Your complete picture now is:
- Bilateral ankle pain (both feet)
- Multiple other joints affected
- Months of duration
- Rest pain (night/car)
- Normal X-rays
- Worsened by inversion
This combination does not fit a mechanical ankle problem. It points strongly toward inflammatory arthritis - a condition where the immune system attacks the joints.
Why Normal X-Rays Don't Rule It Out
X-rays show bone damage, but in early inflammatory arthritis, the bones look completely normal for months to years. Joint inflammation (synovitis) lives in the soft tissue - the joint lining - which is invisible on X-ray. This is one of the most common reasons early arthritis is missed or delayed in diagnosis.
Top Diagnoses to Consider
1. Seronegative Spondyloarthritis (SpA) - Top Suspect
This is a family of inflammatory conditions that have a strong predilection for the ankles, hindfoot, and lower limb joints. The key types include:
| Type | Key Feature |
|---|---|
| Reactive Arthritis | Triggered by a recent infection (gut or urinary/genital) |
| Psoriatic Arthritis (PsA) | Associated with psoriasis skin/nail changes (can come before skin signs) |
| Ankylosing Spondylitis | Back pain + peripheral joints; more in young men |
| IBD-associated Arthritis | Linked to Crohn's or ulcerative colitis |
SpA specifically targets entheses - the points where tendons and ligaments attach to bone - which explains why inversion (stressing the lateral ligament attachments) hurts. The ankle and hindfoot are among the most commonly affected sites. - Rheumatology, 2-Volume Set (Elsevier)
Red flags that would support SpA:
- Morning stiffness lasting more than 30-60 minutes
- Back or buttock pain (especially at night or at rest, improving with movement)
- Skin rash or psoriasis patches (even small ones on scalp, elbows, nails)
- Recent diarrhea, urinary infection, or STI before the joint pain started
- Eye redness or pain (uveitis)
2. Early Rheumatoid Arthritis (RA)
RA classically affects smaller joints (hands, wrists, feet) but can present in the ankles, and bilateral, symmetrical joint involvement is a hallmark. Early RA has:
- Normal X-rays (erosions only appear later)
- Rest pain and morning stiffness
- Multiple joint involvement
3. Viral or Post-Infectious Arthritis
Some viral infections (e.g. parvovirus, hepatitis B/C, chikungunya, COVID-19) can trigger bilateral, multi-joint arthritis that persists for months with normal X-rays.
4. Gout / Pseudogout (Less Likely Without Swelling)
Crystal arthritis typically causes acute flares with swelling and redness, but chronic low-grade crystal deposition can cause persistent bilateral joint aching. Less likely given your absence of swelling.
What the Next Steps Should Be
You need to see a Rheumatologist - this is beyond a general or orthopaedic workup now.
Blood tests your doctor should order:
| Test | What It Checks |
|---|---|
| RF (Rheumatoid Factor) | Marker for RA (negative in early or seronegative disease) |
| Anti-CCP antibody | More specific marker for RA |
| HLA-B27 | Genetic marker strongly linked to spondyloarthritis |
| ESR / CRP | General markers of inflammation |
| Uric acid | Screen for gout |
| FBC (Full Blood Count) | Rule out infection, anemia of inflammation |
| ANA | Screen for lupus/connective tissue disease |
Imaging:
- MRI of ankles - detects synovitis, bone marrow edema, enthesitis, and early erosions invisible on X-ray
- Ultrasound of affected joints - can directly visualize joint inflammation and enthesitis in real-time
Summary
| Feature | Significance |
|---|---|
| Bilateral ankles | Suggests systemic, not mechanical |
| Multiple other joints | Confirms systemic inflammatory process |
| Months of duration | Chronic inflammatory arthritis |
| Rest/night pain | Inflammatory (not mechanical - mechanical pain improves with rest) |
| Normal X-ray | Expected in early inflammatory arthritis |
| Worse with inversion | Enthesitis at lateral ligament insertions |
The distinction between mechanical pain (gets better with rest) and inflammatory pain (persists or is worse at rest, worse in the morning) is one of the most important in medicine - and your symptoms clearly fit the inflammatory pattern.
Please see a rheumatologist. Early treatment of inflammatory arthritis significantly prevents joint damage and disability.
Disclaimer: This is educational information only and cannot replace a clinical evaluation. The conditions described require formal examination, blood tests, and imaging to diagnose accurately.
This is a shared conversation. Sign in to Orris to start your own chat.