Penicillins
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information to write a thorough answer on penicillins. Let me compile everything.
Penicillins
1. Chemistry and Structure
Penicillins share a core nucleus - 6-aminopenicillanic acid (6-APA) - consisting of a thiazolidine ring fused to a beta-lactam ring, with a side chain (R group) attached via an amide bond at position 6. The R group determines the antibacterial spectrum, acid stability, and beta-lactamase susceptibility of each agent.
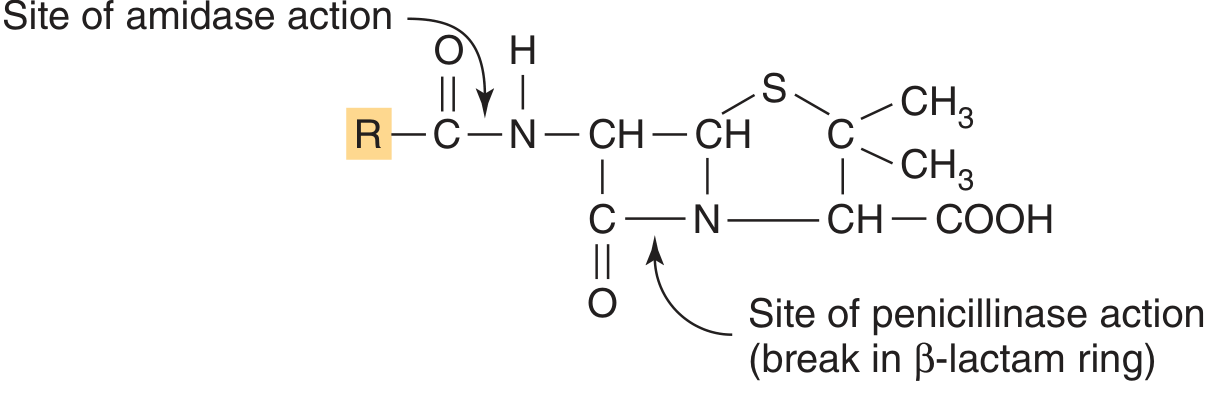
Two enzymatic vulnerabilities:
-
Amidase cleaves the side-chain amide bond (removing the R group)
-
Penicillinase (beta-lactamase) cleaves the beta-lactam ring C-N bond, inactivating the drug
-
Jawetz, Melnick & Adelberg's Medical Microbiology 28th Ed.
-
Goodman & Gilman's Pharmacological Basis of Therapeutics
2. Mechanism of Action
Beta-lactams inhibit the final step of bacterial peptidoglycan cell wall synthesis - the transpeptidation reaction.
The bacterial cell wall is built from glycan chains of alternating N-acetylglucosamine (NAG) and N-acetylmuramic acid (NAM) cross-linked by short peptide bridges. Cross-linking is catalyzed by transpeptidase enzymes (penicillin-binding proteins, PBPs) located outside the plasma membrane.
Penicillins acylate the active-site serine of PBPs by mimicking the D-Ala-D-Ala terminus of the peptidoglycan precursor. This irreversibly inhibits transpeptidation. The result:
- Cell wall synthesis stops
- Existing walls weaken under osmotic stress
- Autolytic enzymes (murein hydrolases) are activated
- Bactericidal lysis occurs (both lytic and non-lytic mechanisms contribute)
Bacteria can produce multiple PBP variants with differing affinities for individual beta-lactams - this underpins some resistance.
Goodman & Gilman's, pp. 1167-1168
3. Classification and Spectrum
Penicillins fall into five principal groups based on side chain modifications:
| Group | Agents | Key Spectrum | Notes |
|---|---|---|---|
| Natural penicillins | Penicillin G (IV), Penicillin V (oral) | Gram-positive cocci (strep, pneumococci), Neisseria meningitidis, spirochetes, anaerobic gram-positives | Acid-labile (pen G), beta-lactamase susceptible, 60% protein-bound |
| Antistaphylococcal (beta-lactamase-resistant) | Oxacillin, Nafcillin, Dicloxacillin, Cloxacillin | MSSA, penicillinase-producing staph | Resistant to staphylococcal beta-lactamase; NOT active vs. MRSA, enterococci, Listeria |
| Aminopenicillins | Ampicillin, Amoxicillin | Extended gram-positive + limited gram-negatives (H. influenzae, E. coli, Proteus mirabilis, Enterococcus, Listeria) | Better absorbed orally (amoxicillin); beta-lactamase susceptible; combined with inhibitors |
| Carboxypenicillins | Ticarcillin (discontinued in USA), Carbenicillin | Anti-Pseudomonal activity added | No longer available in US |
| Ureidopenicillins | Piperacillin (as pip-tazo only) | Gram-negatives incl. Pseudomonas, Klebsiella, E. coli + gram-positive activity | Available only with tazobactam (piperacillin-tazobactam) |
Katzung's Basic and Clinical Pharmacology 16th Ed., pp. 1244-1245
4. Pharmacokinetics
- Distribution: Widely distributed; achieves therapeutic levels in joint fluid, pleural fluid, pericardial fluid, bile
- Poor penetration: Prostate secretions, brain tissue, intraocular fluid, intracellular (phagocytes)
- CSF: <1% of plasma when meninges normal; up to 5% with meningeal inflammation - adequate for treating meningitis at high IV doses
- Elimination: Primarily by renal tubular secretion + glomerular filtration; half-lives typically 30-90 min; high urinary concentrations
- Probenecid blocks renal tubular secretion, raising and prolonging penicillin blood levels
- Food: Most oral penicillins should be taken 1-2 hours before or after meals (amoxicillin is the exception - can be taken with food)
- Dose adjustment: Required in renal failure (high-dose pen G can cause seizures in renal failure)
Goodman & Gilman's, p. 1170
5. Clinical Uses by Agent
Penicillin G (IV)
Drug of choice for:
- Streptococcal infections (4-24 million units/day IV in 4-6 divided doses or continuous infusion)
- Meningococcal meningitis
- Neurosyphilis
- Actinomycosis
- Clostridial infections
- Some enterococcal infections (synergy with aminoglycosides)
Penicillin V (oral)
- Minor streptococcal infections only
- Poor bioavailability; narrow spectrum; amoxicillin often preferred
Benzathine Penicillin G (IM depot)
- Single dose 1.2 million units IM: treats beta-hemolytic strep pharyngitis
- 1.2 million units IM every 3-4 weeks: rheumatic fever prophylaxis
- 2.4 million units IM weekly x 1-3 weeks: syphilis treatment
Procaine Penicillin G
- Intermediate-acting IM depot; largely replaced by newer agents
Oxacillin / Nafcillin (IV)
- MSSA serious infections (endocarditis, bacteremia): 8-12 g/day IV
- Drug of choice for methicillin-susceptible staphylococci
Dicloxacillin / Cloxacillin (oral)
- Mild-moderate MSSA infections (skin/soft tissue): 0.25-0.5 g PO q4-6h
Ampicillin (IV/oral)
- Enterococcal infections, Listeria meningitis, susceptible gram-negatives
- 4-12 g/day IV for serious infections
Amoxicillin (oral)
- Otitis media, sinusitis, community-acquired pneumonia (strep), H. pylori (triple therapy)
- 250-500 mg TID
Amoxicillin-clavulanate / Ampicillin-sulbactam / Piperacillin-tazobactam
- Beta-lactamase inhibitor combinations that restore activity against many beta-lactamase-producing organisms
Katzung's Basic and Clinical Pharmacology 16th Ed.
6. Mechanisms of Resistance
Three main mechanisms:
(a) Beta-lactamase Production (most common)
- Enzymes that hydrolyze the beta-lactam ring
- Gram-positives (e.g., S. aureus): secrete large amounts of narrow-spectrum penicillinase; gene carried on plasmid, transferable by bacteriophage, expression inducible
- Gram-negatives: produce beta-lactamases in smaller amounts but strategically located in the periplasmic space - maximally protecting the cell
- ESBL (extended-spectrum beta-lactamases): hydrolyze most penicillins AND cephalosporins
- Carbapenemases (e.g., KPC): hydrolyze nearly all beta-lactams
(b) Altered Penicillin-Binding Proteins
- PBPs acquire mutations reducing beta-lactam affinity
- Key example: MRSA expresses PBP2a (encoded by mecA gene) - very low affinity for all beta-lactams
- Penicillin-resistant pneumococci: altered PBPs
(c) Reduced Permeability / Efflux Pumps
- Gram-negatives reduce outer membrane porin channels (e.g., OprD loss in Pseudomonas)
- Active efflux pumps remove drug before it can act
Goodman & Gilman's, pp. 1168-1170
7. Adverse Effects
| Adverse Effect | Details |
|---|---|
| Hypersensitivity (most important) | Antigenic determinants = penicillinic acid + alkaline hydrolysis products bound to host protein |
| Anaphylaxis | Very rare (0.05% of recipients); IgE-mediated; requires immediate epinephrine |
| Serum sickness | Urticaria, fever, joint swelling, angioedema 7-12 days post-exposure (now rare) |
| Skin rashes | Maculopapular; notably with ampicillin/amoxicillin in EBV infection |
| Interstitial nephritis | Autoimmune reaction to penicillin-protein complex; particularly with nafcillin |
| Seizures | High-dose penicillin G in renal failure |
| Neutropenia | Nafcillin |
| Hepatitis | Oxacillin |
| Hypokalemia | Large doses of piperacillin (contains sodium load) |
| GI upset | Large oral doses - nausea, vomiting, diarrhea |
| C. difficile colitis | As with all antibiotics |
| Acute kidney injury | Piperacillin-tazobactam combined with vancomycin (higher risk vs. other beta-lactams + vancomycin) |
Allergy notes:
- ~5-8% of patients report penicillin allergy, but only a small fraction have true IgE-mediated allergy
- Penicillin skin testing can evaluate type I (immediate) hypersensitivity
- Negative skin test = most patients can safely receive penicillin
- If penicillin is essential (e.g., enterococcal endocarditis, neurosyphilis in a penicillin-allergic patient): desensitization with gradually increasing doses is possible
- Cross-reactivity with cephalosporins is real but low (~1-2% in patients with penicillin allergy)
Katzung's Basic and Clinical Pharmacology 16th Ed., pp. 1245-1246
8. Beta-Lactamase Inhibitors
When combined with penicillins, these agents inhibit beta-lactamases without significant antibacterial activity themselves:
| Combination | Route | Key added coverage |
|---|---|---|
| Amoxicillin + clavulanate | PO | Beta-lactamase-producing S. aureus, H. influenzae, Moraxella, oral anaerobes |
| Ampicillin + sulbactam | IV | As above + Acinetobacter |
| Piperacillin + tazobactam | IV | Broad gram-negatives incl. Pseudomonas, anaerobes, gram-positives |
Summary: Spectrum at a Glance
Narrow (Pen G/V) → Gram-positives, spirochetes, some anaerobes
Anti-staph (oxacillin) → MSSA only
Aminopenicillins → Above + limited gram-negatives (but no Pseudomonas)
Pip-tazo → Broad spectrum incl. Pseudomonas
Key rule: Penicillins are bactericidal, time-dependent killers - efficacy correlates with the percentage of time the free drug concentration exceeds the MIC (T>MIC). This is why extended/continuous infusions are used for serious infections.
Sources: Katzung's Basic and Clinical Pharmacology 16th Ed. | Goodman & Gilman's Pharmacological Basis of Therapeutics | Jawetz, Melnick & Adelberg's Medical Microbiology 28th Ed.

Give me the All of this topic Answer in the MUHS bpth pharmacology level
Finding Sources
Finding Sources
I have all the content needed from the previous detailed session plus these additional ADR snippets. Here is the complete MUHS BPTh exam-level answer:
Penicillins - MUHS 2nd Year B.P.Th. Pharmacology
Exam Pattern (as per MUHS analysis): Classification | Mechanism of Action | Clinical Indications | ADRs This topic appears in Winter & Winter exam cycles - expect 10-mark long answers or 5-mark short notes.
CLASSIFICATION OF PENICILLINS
Penicillins are classified based on their spectrum of activity and resistance to beta-lactamases:
Group 1 - Natural Penicillins
| Drug | Route | Key Feature |
|---|---|---|
| Penicillin G (Benzylpenicillin) | Injection (IV/IM) | Narrow spectrum, acid-labile, beta-lactamase susceptible |
| Penicillin V (Phenoxymethyl penicillin) | Oral | Acid-stable form of Pen G |
| Benzathine Penicillin G | IM depot | Long-acting (2-4 weeks) |
| Procaine Penicillin G | IM depot | Intermediate-acting |
Group 2 - Beta-Lactamase Resistant (Anti-Staphylococcal) Penicillins
| Drug | Route |
|---|---|
| Methicillin | Obsolete (caused nephritis) |
| Nafcillin | IV |
| Oxacillin | IV |
| Cloxacillin | Oral/IV |
| Dicloxacillin | Oral |
Group 3 - Aminopenicillins (Extended Spectrum)
| Drug | Route |
|---|---|
| Ampicillin | Oral/IV |
| Amoxicillin | Oral |
| Amoxicillin + Clavulanate (Augmentin) | Oral |
| Ampicillin + Sulbactam (Unasyn) | IV |
Group 4 - Antipseudomonal Penicillins (Ureidopenicillins)
| Drug | Route |
|---|---|
| Piperacillin + Tazobactam (Pip-Tazo) | IV |
| Ticarcillin + Clavulanate | IV (discontinued in USA) |
Memory tip: N-A-C-D for anti-staph penicillins: Nafcillin, Ampicillin (no - that's amino), actually: Nafcillin, Oxacillin, Cloxacillin, Dicloxacillin = NOCD
MECHANISM OF ACTION
Basic Concept
Penicillins are bactericidal and act by inhibiting bacterial cell wall synthesis.
Step-by-Step Mechanism
Step 1 - Normal bacterial cell wall synthesis:
- Bacterial cell wall is made of peptidoglycan - a mesh of NAG (N-acetylglucosamine) and NAM (N-acetylmuramic acid) strands cross-linked by short peptide bridges
- The final cross-linking step is done by an enzyme called transpeptidase (also called Penicillin-Binding Protein / PBP)
Step 2 - How penicillin works:
- Penicillin structurally mimics D-Ala-D-Ala, the terminal end of the peptide precursor
- It binds irreversibly to PBPs (transpeptidase) and blocks cross-linking
- Without cross-linking, the cell wall becomes structurally weak
Step 3 - Cell death:
- Weak cell wall cannot withstand osmotic pressure
- Bacterial autolytic enzymes (murein hydrolases) are activated
- Cell undergoes lysis and death
Important Pharmacodynamic Point
Penicillins are time-dependent antibiotics - their killing depends on the time the drug concentration remains above the MIC (Minimum Inhibitory Concentration), not on peak concentration.
Mechanism of Resistance (MUHS may ask this as part of MOA)
Three mechanisms:
-
Beta-lactamase production (most common)
- Bacteria produce enzymes that break open the beta-lactam ring
- Example: MRSA, beta-lactamase-producing H. influenzae
- Overcome by: combining with beta-lactamase inhibitors (clavulanate, sulbactam, tazobactam)
-
Altered PBPs
- PBPs mutate to have low affinity for penicillin
- Key example: MRSA produces PBP2a (encoded by mecA gene) - resistant to ALL beta-lactams
-
Reduced permeability / Efflux pumps
- Gram-negative bacteria reduce porin channels, limiting drug entry
- Efflux pumps actively expel the drug
CLINICAL INDICATIONS (Uses)
Penicillin G and V (Natural Penicillins)
| Condition | Organism |
|---|---|
| Streptococcal pharyngitis / tonsillitis | Group A Streptococcus |
| Rheumatic fever prophylaxis | Group A Streptococcus |
| Bacterial meningitis | Neisseria meningitidis |
| Syphilis (primary, secondary, tertiary, neurosyphilis) | Treponema pallidum |
| Tetanus (adjunct to antitoxin) | Clostridium tetani |
| Gas gangrene | Clostridium perfringens |
| Actinomycosis | Actinomyces israelii |
| Leptospirosis | Leptospira spp. |
| Diphtheria (adjunct) | Corynebacterium diphtheriae |
Antistaphylococcal Penicillins (Oxacillin, Nafcillin, Cloxacillin, Dicloxacillin)
- Skin and soft tissue infections caused by MSSA (Methicillin-Susceptible S. aureus)
- Staphylococcal endocarditis (oxacillin/nafcillin IV)
- Staphylococcal osteomyelitis
- NOT used for MRSA (vancomycin is used for MRSA)
Aminopenicillins (Ampicillin, Amoxicillin)
| Condition | Notes |
|---|---|
| Otitis media | Amoxicillin - first line |
| Sinusitis | Amoxicillin |
| Community-acquired pneumonia | Ampicillin/amoxicillin |
| Urinary tract infections (susceptible E. coli) | Ampicillin |
| Typhoid fever (susceptible Salmonella) | Ampicillin |
| Listeria meningitis | Ampicillin (ONLY penicillin active vs Listeria) |
| Enterococcal infections | Ampicillin + aminoglycoside (synergy) |
| H. pylori eradication | Amoxicillin (part of triple therapy) |
| Mononucleosis | AVOID - causes rash |
Piperacillin-Tazobactam (Pip-Tazo)
- Hospital-acquired infections
- Ventilator-associated pneumonia
- Intra-abdominal infections (anaerobes + gram-negatives)
- Pseudomonal infections
- Febrile neutropenia (empiric)
ADVERSE DRUG REACTIONS (ADRs)
1. Hypersensitivity Reactions (Most Important)
The antigenic determinants are penicillinic acid and alkaline hydrolysis products that bind to host proteins.
| Type | Reaction | Time of Onset |
|---|---|---|
| Type I (IgE-mediated) | Anaphylaxis, urticaria, angioedema, bronchospasm | Immediate (within 1 hour) |
| Type II (Cytotoxic) | Hemolytic anemia, thrombocytopenia | Days |
| Type III (Immune complex) | Serum sickness - fever, joint pain, rash, angioedema | 7-12 days post-exposure |
| Type IV (Delayed/T-cell) | Maculopapular rash, contact dermatitis | 48-72 hours |
Key facts for exam:
- Anaphylaxis incidence = very rare (0.05% of recipients) - but potentially fatal
- ~5-8% of patients claim penicillin allergy, but most do NOT have true allergy
- Penicillin skin test is used to evaluate Type I hypersensitivity before giving the drug
- If allergic but penicillin essential (e.g., neurosyphilis): perform desensitization with gradually increasing doses
- Cross-reactivity with cephalosporins - exists but is low (~1-2%)
2. Ampicillin / Amoxicillin - Specific Rash
- Non-immune maculopapular skin rash
- Notably seen in Epstein-Barr virus (EBV) / Infectious Mononucleosis - avoid ampicillin/amoxicillin in these patients
- Also seen in CLL patients and with allopurinol co-administration
3. CNS Toxicity
- Seizures with high-dose Penicillin G in patients with renal failure (due to drug accumulation)
- Mechanism: GABA receptor antagonism at very high drug levels
4. Organ-Specific Toxicities
| Drug | Specific ADR |
|---|---|
| Nafcillin | Neutropenia, interstitial nephritis |
| Oxacillin | Hepatitis (elevated liver enzymes) |
| Methicillin | Interstitial nephritis (reason it was withdrawn) |
| Piperacillin-tazobactam | Acute kidney injury (especially with vancomycin) |
| Ampicillin + Vancomycin | Hypokalemia with large sodium loads |
5. GI Effects
- Nausea, vomiting, diarrhea (especially with large oral doses)
- Clostridium difficile (C. diff) pseudomembranous colitis - associated with broad-spectrum penicillins disrupting gut flora
6. Superinfections
- Secondary oral candidiasis (thrush)
- Vaginal candidiasis
- Due to disruption of normal microbial flora
SEMI-SYNTHETIC PENICILLINS - Key Points (MUHS specifically asks this)
Semi-synthetic penicillins are produced by chemically modifying the 6-APA nucleus of natural penicillin. The side chain (R group) is changed to achieve:
| Goal | Example |
|---|---|
| Acid stability (oral use) | Amoxicillin, Ampicillin |
| Beta-lactamase resistance | Cloxacillin, Dicloxacillin, Oxacillin, Nafcillin |
| Broader gram-negative spectrum | Ampicillin, Amoxicillin |
| Anti-pseudomonal activity | Piperacillin |
All semi-synthetic penicillins still share the same core mechanism of action (PBP inhibition) and the same type of hypersensitivity reactions as natural penicillins.
QUICK REVISION TABLE - MUHS Exam Ready
| Feature | Natural Pen G | Anti-Staph (Cloxacillin) | Aminopenicillin (Amoxicillin) | Piperacillin-Tazo |
|---|---|---|---|---|
| Gram-positive | +++ | +++ | ++ | ++ |
| Gram-negative | + (limited) | - | ++ (no pseudomonas) | ++++ (incl. pseudomonas) |
| Beta-lactamase resistant | No | Yes | No (unless + inhibitor) | Yes (tazobactam present) |
| Oral bioavailability | Poor (Pen V oral) | Moderate | Good | No (IV only) |
| Key use | Strep, syphilis | MSSA infections | Otitis, pneumonia, UTI | Severe hospital infections |
| Important ADR | Anaphylaxis | Neutropenia (nafcillin) | EBV rash, ampicillin rash | AKI with vancomycin |
EXAM TIPS FOR MUHS BPTh
-
Long answer (10 marks): Write Classification + MOA + Clinical Uses + ADRs with headings. Draw the beta-lactam ring and label where penicillinase acts.
-
Short note (5 marks): Focus on MOA alone - explain PBP inhibition in steps, or write ADRs with hypersensitivity types clearly tabulated.
-
Always mention: Time-dependent killing, bactericidal nature, and that they do NOT cover MRSA (except ceftaroline among cephalosporins, but not penicillins).
-
Clinical correlation for physiotherapy context: Penicillins may be given to BPTh patients with post-surgical wound infections, cellulitis, or pneumonia - know their ADRs to counsel patients about rash, GI upset, and allergic warning signs.
Sources: Katzung's Basic and Clinical Pharmacology 16th Ed. | Goodman & Gilman's Pharmacological Basis of Therapeutics | Jawetz, Melnick & Adelberg's Medical Microbiology 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.