I want to master ophthalmology for overall concept as well as NEET PG preparation,you will tell me the full roadmap,like in phases divide then when I will tell you any particular phase write about that phase in full details in long format, explain everything in details start it from the basic so my concept become Crystal clear, so use easy and simple language, whenever you tell me some terminology like Hypopyon,or anything medical just write the simple meaning in the bracket so that I can understand what actually is this, arrange the phases in such sequence so that one after one I can understand the whole things, when you will tell me anything,if there is mention of any disease related to optha then just write the prescription note like a professional doctor like eye drops, ointment etc
NEET PG ophthalmology syllabus important topics 2025
https://www.prepladder.com/neet-pg-study-material/ophthalmol…
🏥 Complete Ophthalmology Mastery Roadmap
For Concept Clarity + NEET PG Preparation
How to use this roadmap: Tell me any Phase number (e.g., "Phase 1") and I will write it in full detail - with easy language, simple explanations in brackets, prescriptions, diagrams described, and NEET PG high-yield points clearly marked.
📌 OVERVIEW: Why Ophthalmology is Special in NEET PG
- Clinical (patient presenting with red eye, blurred vision, etc.)
- Image-based (fundus photos, instruments, slit-lamp findings)
- Instrument-based (what instrument is used for what)
- Prescription-based (which drop for which disease)
🗺️ THE COMPLETE PHASED ROADMAP
🔵 PHASE 1 — Foundation: Anatomy & Physiology of the Eye
- Layers of the eyeball (coat by coat - fibrous, uveal, nervous)
- Cornea, Sclera, Uvea (Iris, Ciliary body, Choroid)
- Lens anatomy and physiology
- Retina (10 layers - must know for NEET PG)
- Vitreous body
- Aqueous humor - production, drainage, and its role in pressure
- Extraocular muscles (6 muscles) - attachments, actions, nerve supply
- Blood supply of the eye - ophthalmic artery and its branches
- Lacrimal system (tear production and drainage)
- Optic nerve anatomy
- Visual pathway (from eye to brain - very NEET PG important)
🔵 PHASE 2 — Optics and Refraction
- Basic optics: lenses, prisms, mirrors
- Emmetropia (normal eye), Myopia (short-sightedness), Hypermetropia (long-sightedness), Astigmatism (blurred at all distances)
- Presbyopia (age-related reading difficulty)
- Accommodation (how the eye adjusts focus for near/far)
- Refractive surgery - LASIK, PRK
- Contact lenses
- Instruments: Retinoscope, Keratometer, Autorefractometer
- Optical coherence: important formulas (Snellen chart, Jaeger chart)
- IOL (Intraocular Lens) power calculation
🔵 PHASE 3 — Eyelids, Orbit & Lacrimal System
- Eyelid anatomy and diseases:
- Chalazion (a painless, firm lump in the eyelid due to blocked gland)
- Hordeolum/Stye (painful infection of eyelid gland)
- Blepharitis (inflammation/infection of eyelid margins)
- Ptosis (drooping of upper eyelid)
- Entropion (eyelid turning inward)
- Ectropion (eyelid turning outward)
- Trichiasis (eyelashes growing inward and scratching the eye)
- Orbital diseases:
- Proptosis (bulging of eyeball out of the socket)
- Thyroid Eye Disease (Graves' ophthalmopathy)
- Orbital cellulitis (infection of the tissue around the eye)
- Blow-out fracture of orbit
- Lacrimal system diseases:
- Dacryocystitis (infection of the tear sac)
- Dry eye syndrome
🔵 PHASE 4 — Conjunctiva & Sclera
- Anatomy of conjunctiva
- Conjunctivitis (redness/infection of the white part of the eye):
- Bacterial, Viral (Adenoviral - epidemic), Chlamydial (Trachoma)
- Allergic conjunctivitis
- Neonatal conjunctivitis (Ophthalmia neonatorum)
- Pterygium (a wing-shaped growth of tissue on the white part of the eye)
- Pinguecula (a small yellowish deposit on the conjunctiva)
- Subconjunctival hemorrhage (bleeding under the clear surface)
- Sclera diseases:
- Episcleritis (mild inflammation of outer layer of white part)
- Scleritis (deeper, more painful inflammation)
🔵 PHASE 5 — Cornea
- Corneal anatomy (5 layers - must memorize)
- Corneal ulcers:
- Bacterial (most common: Pseudomonas, Pneumococcus)
- Fungal (after vegetative trauma - e.g., twig injury)
- Herpetic/Viral (Herpes simplex - dendritic ulcer)
- Acanthamoeba (in contact lens wearers)
- Keratoconus (cone-shaped cornea causing blurring)
- Corneal dystrophies
- Keratoplasty (corneal transplant - PK/DALK/DSAEK)
- Mooren's ulcer (peripheral corneal ulcer with no known cause)
- Band-shaped keratopathy (calcium deposits on cornea)
- Arcus senilis (white ring around cornea in elderly - harmless)
🔵 PHASE 6 — Glaucoma
- Intraocular Pressure (IOP) - what is normal, what is high
- Open angle vs Closed angle glaucoma (the two main types)
- Primary Open Angle Glaucoma (POAG) - the most common type, painless
- Acute Angle Closure Glaucoma (AACG) - emergency, very painful red eye
- Secondary glaucomas - steroid-induced, traumatic, neovascular
- Congenital glaucoma (Buphthalmos - enlarged eye in baby)
- Visual field defects in glaucoma (what parts of vision are lost first)
- Optic disc changes in glaucoma (cup-disc ratio)
- Investigations: Tonometry, Gonioscopy, Perimetry
- All medical treatments (eye drops)
- Surgical treatments: Trabeculectomy, Laser procedures
🔵 PHASE 7 — Lens & Cataract
- Lens anatomy and metabolism
- Cataract (clouding of the lens):
- Age-related (senile) cataract - most common
- Congenital cataract (present from birth)
- Traumatic cataract
- Secondary/Complicated cataract
- Metabolic cataracts (diabetic, galactosemic)
- Types of age-related cataract: Nuclear, Cortical, Posterior Subcapsular
- Cataract surgery:
- ECCE (Extracapsular Cataract Extraction)
- ICCE (Intracapsular)
- Phacoemulsification (modern method using ultrasound)
- IOL (Intraocular Lens) implantation
- Complications of cataract surgery
- Subluxation/dislocation of lens (Marfan syndrome, Homocystinuria)
- Aphakia (eye without lens) vs Pseudophakia (eye with artificial lens)
🔵 PHASE 8 — Uvea & Uveitis
- Uveal tract anatomy (Iris + Ciliary body + Choroid)
- Uveitis (inflammation of uvea):
- Anterior uveitis/Iritis (front part)
- Intermediate uveitis
- Posterior uveitis/Choroiditis
- Panuveitis (all parts together)
- Systemic associations (HLA-B27 diseases, TB, Sarcoidosis, Behcet's disease, Toxoplasma, etc.)
- Complications: Hypopyon (pus in the front chamber of the eye), Posterior Synechiae (iris sticks to lens), Complicated Cataract, Secondary Glaucoma
- Sympathetic Ophthalmia (a special rare condition where injury to one eye causes inflammation in the other eye)
- Treatment principles
🔵 PHASE 9 — Retina
- Retinal anatomy and the 10 layers
- Diabetic Retinopathy (retinal damage due to diabetes)
- Non-proliferative vs Proliferative stages
- Hypertensive Retinopathy (retinal changes due to high blood pressure)
- Retinal Detachment (retina peels away from back wall):
- Rhegmatogenous (hole-related)
- Tractional
- Exudative
- CRAO (Central Retinal Artery Occlusion - sudden painless vision loss, cherry red spot)
- CRVO (Central Retinal Vein Occlusion - "blood and thunder" fundus)
- Age-related Macular Degeneration (AMD) - dry and wet types
- Retinitis Pigmentosa (hereditary disease, night blindness first)
- Retinoblastoma (malignant eye tumor in children - "white pupil"/leukocoria)
- Fundus examination findings - must recognize images
🔵 PHASE 10 — Neuro-Ophthalmology
- Visual pathway in detail - where each lesion causes what field defect
- Visual field defects (Hemianopia, Quadrantanopia, Scotoma, etc.)
- Pupil anatomy and reflexes
- RAPD (Relative Afferent Pupillary Defect - a clinical test where one eye has reduced response to light)
- Argyll Robertson Pupil (pupil of syphilis - "prostitute's pupil" - accommodates but does not react to light)
- Horner's Syndrome (droopy lid + small pupil + sunken eye)
- Holmes-Adie Pupil (sluggish pupil reaction)
- Optic neuritis (inflammation of the optic nerve, associated with Multiple Sclerosis)
- Papilloedema (swelling of optic disc due to raised brain pressure)
- Optic atrophy (degeneration/death of optic nerve fibers)
- Cranial nerve palsies (3rd, 4th, 6th nerve)
- Nystagmus (involuntary rhythmic eye movements)
🔵 PHASE 11 — Squint & Amblyopia
- Squint/Strabismus (misalignment of eyes - one eye turns in, out, up, or down)
- Concomitant vs Incomitant squint
- Esotropia (eye turns inward), Exotropia (eye turns outward)
- Cover test, Hirschberg test, Prism bar cover test
- Amblyopia (lazy eye - reduced vision in one eye without structural cause)
- Treatment: Patching, Surgery, Glasses
- Diplopia (double vision)
- Paralytic squint (due to nerve palsy)
🔵 PHASE 12 — Ocular Trauma
- Chemical injuries (acid vs alkali - alkali is worse)
- Mechanical injuries:
- Blunt trauma
- Penetrating/Perforating injuries
- IOFB (Intraocular Foreign Body)
- Hyphema (bleeding into the front chamber of the eye after trauma)
- Blow-out fracture of orbit
- Sympathetic Ophthalmia (post-traumatic, bilateral inflammation)
- Radiation injuries
🔵 PHASE 13 — Ophthalmic Instruments & Investigations
- Slit lamp (the main examination instrument of the eye)
- Direct and Indirect Ophthalmoscope
- Tonometer (measures eye pressure):
- Goldman Applanation Tonometer (gold standard)
- Schiotz Tonometer
- Non-contact/Air puff tonometer
- Gonioscope (to see the drainage angle of the eye)
- Perimeter (to test visual fields)
- Keratometer / Autorefractometer
- OCT (Optical Coherence Tomography - like a CT scan for retina)
- Retinoscope
- Synoptophore (to test eye muscle balance)
- Fundus Fluorescein Angiography (FFA) - retinal blood vessel imaging
🔵 PHASE 14 — Ocular Manifestations of Systemic Diseases
- Diabetes - retinopathy, cataract, cranial nerve palsies, rubeosis iridis (new blood vessel growth on iris)
- Hypertension - hypertensive retinopathy (Keith-Wagener classification)
- Thyroid disease - Graves' ophthalmopathy (proptosis, lid retraction)
- Tuberculosis - uveitis, choroiditis, optic neuritis
- Sarcoidosis - uveitis, lacrimal gland swelling
- Syphilis - Argyll Robertson pupil, interstitial keratitis
- Multiple Sclerosis - optic neuritis, INO (Internuclear Ophthalmoplegia)
- Rheumatoid Arthritis - scleritis, dry eye
- HIV/AIDS - CMV retinitis (pizza pie appearance on fundus)
- Hypertension in Pregnancy - ocular changes
🔵 PHASE 15 — High-Yield One-Liners, PYQs & Rapid Revision
- All "first choice" drugs for each eye disease
- All eponyms in ophthalmology (Fleischer ring, Kayser-Fleischer ring, etc.)
- All classic associations (e.g., asteroid hyalosis, etc.)
- Previous year NEET PG question analysis
- Image-based question practice (fundus photos, slit-lamp images, instruments)
- Important one-liners and must-remember facts
- Short-cut mnemonics for visual field defects, drug mechanisms, etc.
📊 PHASE-WISE NEET PG IMPORTANCE TABLE
| Phase | Topic | NEET PG Importance |
|---|---|---|
| 1 | Anatomy & Physiology | ⭐⭐⭐⭐ High |
| 2 | Optics & Refraction | ⭐⭐⭐⭐ High |
| 3 | Eyelids, Orbit, Lacrimal | ⭐⭐⭐ Moderate-High |
| 4 | Conjunctiva & Sclera | ⭐⭐⭐ Moderate-High |
| 5 | Cornea | ⭐⭐⭐⭐ High |
| 6 | Glaucoma | ⭐⭐⭐⭐⭐ Very High |
| 7 | Lens & Cataract | ⭐⭐⭐⭐⭐ Very High |
| 8 | Uvea & Uveitis | ⭐⭐⭐⭐ High |
| 9 | Retina | ⭐⭐⭐⭐⭐ Very High |
| 10 | Neuro-Ophthalmology | ⭐⭐⭐⭐ High |
| 11 | Squint & Amblyopia | ⭐⭐⭐ Moderate-High |
| 12 | Ocular Trauma | ⭐⭐⭐⭐ High |
| 13 | Instruments | ⭐⭐⭐⭐⭐ Very High |
| 14 | Systemic Associations | ⭐⭐⭐⭐ High |
| 15 | PYQs & Rapid Revision | ⭐⭐⭐⭐⭐ Very High |
📅 SUGGESTED STUDY SEQUENCE
Week 1-2 → Phase 1 (Anatomy) + Phase 2 (Optics)
Week 3 → Phase 3 (Lids/Orbit) + Phase 4 (Conjunctiva)
Week 4 → Phase 5 (Cornea) + Phase 8 (Uvea)
Week 5 → Phase 6 (Glaucoma) — spend extra time here
Week 6 → Phase 7 (Cataract/Lens) — spend extra time here
Week 7 → Phase 9 (Retina) — spend extra time here
Week 8 → Phase 10 (Neuro-Ophthalmology) + Phase 11 (Squint)
Week 9 → Phase 12 (Trauma) + Phase 13 (Instruments) + Phase 14 (Systemic)
Week 10+ → Phase 15 (PYQs + Revision) — repeat weak areas
✅ HOW TO USE THIS ROADMAP
- Say "Phase 1" and I will write a complete, detailed lesson on Anatomy - with simple language, bracket explanations for every term, doctor-style prescriptions for any diseases mentioned, and NEET PG high-yield points highlighted.
- We go phase by phase - one at a time - so your concepts build logically on each other.
- Each phase will include:
- 📖 Simple concept explanations
- 🔬 Important facts in easy language
- 💊 Doctor-style prescription notes for all diseases
- ⭐ NEET PG high-yield boxes
- 🧠 Memory tricks and mnemonics
Phase 1
🔵 PHASE 1 — Foundation: Anatomy & Physiology of the Eye
Complete Detailed Lesson | Concept + NEET PG
🌟 START HERE: Think of the Eye Like a Camera
Your eye = A digital camera
- The cornea + lens = The camera lens (focuses light)
- The pupil = The aperture/hole (controls how much light enters)
- The retina = The camera sensor/film (captures the image)
- The optic nerve = The data cable (sends image to the brain)
- The brain (visual cortex) = The computer screen (shows the final picture)
📐 PART 1: The Eyeball — Shape, Size & Position
- Roughly spherical (round like a ball)
- About 24 mm in diameter (size of a large marble)
- Sits inside a bony cavity called the Orbit (the protective bone socket in your skull)
- Protected by bony walls made of 7 bones: frontal, zygomatic, maxilla, sphenoid, palatine, lacrimal, and ethmoid
🏗️ PART 2: The Three Coats (Layers) of the Eyeball
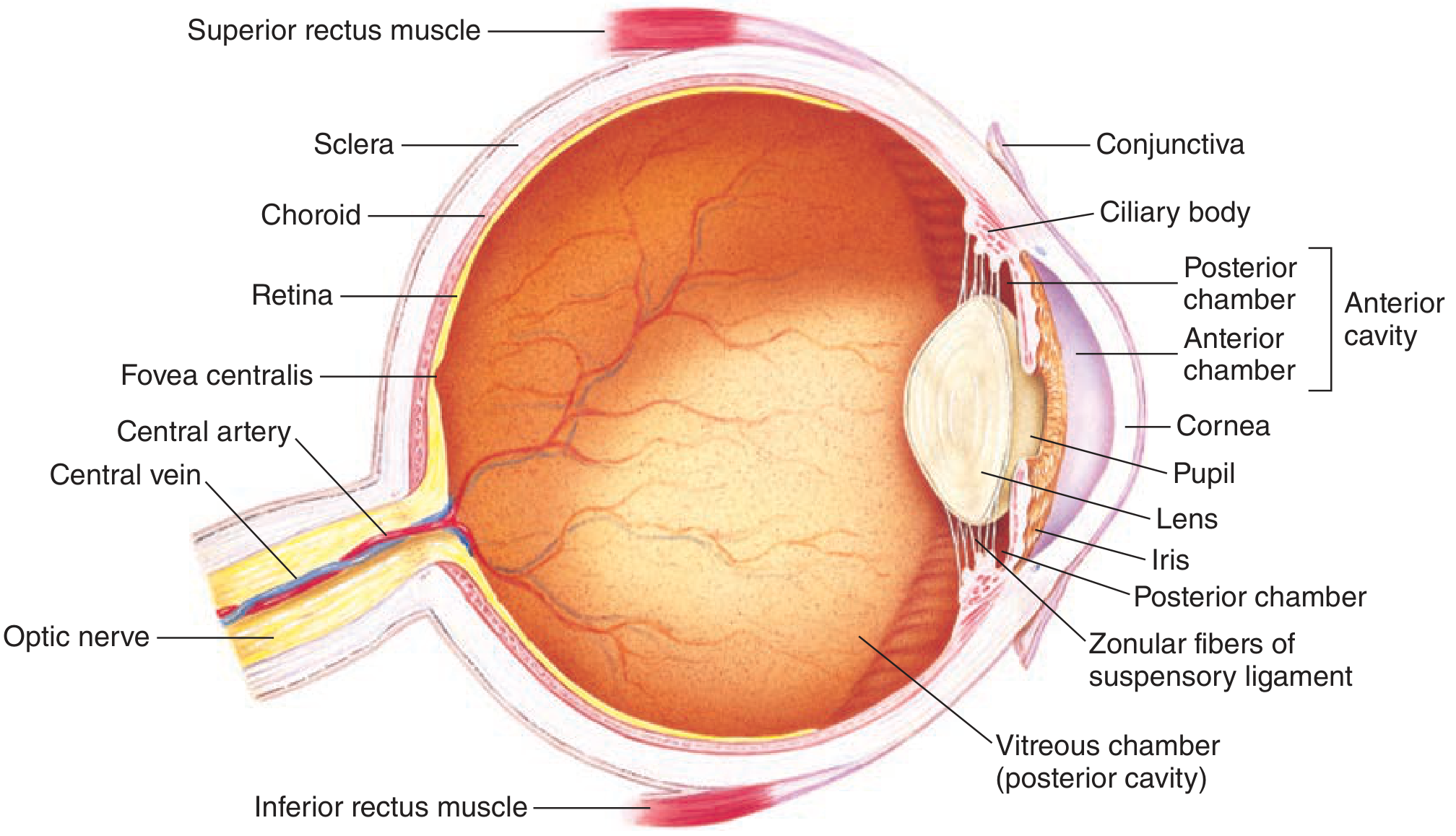
🔴 COAT 1 — Fibrous Coat (Outermost Layer)
A) SCLERA (The White of the Eye)
- Makes up the posterior 5/6th (back 5/6th) of the eyeball
- White, tough, opaque (no light passes through it)
- Made of collagen fibers
- Protects all the inner delicate structures
- Think of it as the white shell of an egg
B) CORNEA (Transparent Front Window)
- Makes up the anterior 1/6th (front 1/6th) of the eyeball
- Completely transparent (clear - allows light to enter)
- Avascular (no blood vessels - gets nutrition from aqueous humor and tear film)
- Highly sensitive - has the richest nerve supply of any tissue in the body (that's why a speck of dust in your eye hurts so much!)
- The first and most powerful refracting (light-bending) surface of the eye
- Power of cornea = +43 Diopters (most of the focusing power)
| Layer (front to back) | Memory Trick |
|---|---|
| 1. Epithelium (outer skin layer) | E |
| 2. Bowman's membrane (tough layer below epithelium) | B |
| 3. Stroma (thickest middle layer - 90% of cornea) | S |
| 4. Descemet's membrane (thin strong membrane) | D |
| 5. Endothelium (single inner cell layer - pumps water out) | E |
Important: The Endothelium is critical - it pumps fluid OUT of the cornea to keep it transparent. If endothelial cells die (they cannot regenerate!), cornea becomes cloudy (edematous). This is why corneal transplant is needed in advanced corneal disease.
🔵 COAT 2 — Uveal Coat (Middle Layer)
A) IRIS (The Colored Part of the Eye)
- The colored ring you see (brown, blue, green, etc.) is the iris
- Has a central hole = the Pupil (the black circle you see in the middle)
- Contains two muscles that control pupil size:
| Muscle | Action | Nerve Supply |
|---|---|---|
| Sphincter pupillae (ring-shaped muscle) | Makes pupil SMALLER (Miosis = constriction) | Parasympathetic (CN III) |
| Dilator pupillae (radial/spoke-like muscle) | Makes pupil BIGGER (Mydriasis = dilation) | Sympathetic nerve |
- Light (bright day) → Pupil constricts (shrinks) → Parasympathetic
- Dark (night/fear) → Pupil dilates (enlarges) → Sympathetic
B) CILIARY BODY (The Middle Part of Uvea)
- Located just behind the iris
- Has two very important functions:
- Produces Aqueous Humor (the clear fluid that fills the front part of the eye - like water filling a tank)
- Controls Lens Shape via the Ciliary Muscle (for near/far focusing)
- Fine fibers that connect the ciliary body to the lens
- When ciliary muscle contracts → zonules relax → lens becomes thicker → eye focuses NEAR
- When ciliary muscle relaxes → zonules tighten → lens becomes thinner → eye focuses FAR
C) CHOROID (The Back Part of Uvea)
- A dark-brown, highly vascular layer
- Lines the posterior 2/3rds of the eyeball (behind the ciliary body)
- Main function: Nourishes the outer layers of the retina (like a rich blood supply carpet)
- Rich in melanin pigment (dark color) - acts like a dark room to prevent internal light scatter
- Contains the Choriocapillaris (a very fine network of capillaries just inside the choroid that supplies the outer retina)
🟢 COAT 3 — Nervous Coat (Innermost Layer)
THE RETINA (The Camera Film)
- The innermost layer, lining the back 2/3rds of the eyeball
- Contains the photoreceptors (light-sensing cells) - the actual "camera sensor"
- Is a neurosensory membrane - converts light energy into nerve signals
- Only about 0.5 mm thick but incredibly complex
| # | Layer | Simple Meaning |
|---|---|---|
| 1 | Retinal Pigment Epithelium (RPE) | Outer dark pigment layer |
| 2 | Photoreceptor layer (rods & cones) | The actual light sensors |
| 3 | External Limiting Membrane | Thin boundary layer |
| 4 | Outer Nuclear Layer | Nuclei (cell bodies) of photoreceptors |
| 5 | Outer Plexiform Layer | Connections between photoreceptors and next cells |
| 6 | Inner Nuclear Layer | Nuclei of bipolar cells, horizontal cells, amacrine cells |
| 7 | Inner Plexiform Layer | Connections between bipolar and ganglion cells |
| 8 | Ganglion Cell Layer | The ganglion cell bodies |
| 9 | Nerve Fiber Layer | Axons of ganglion cells heading to optic nerve |
| 10 | Internal Limiting Membrane | Innermost boundary |
- The retina is attached to the underlying RPE only at 2 points: the optic disc and the ora serrata (the front edge of the retina)
- The rest is only loosely attached → this is why retinal detachment happens (retina peels away)
SPECIAL AREAS OF THE RETINA (Very Important!)
- Where all the nerve fibers collect and leave the eye as the optic nerve
- Located slightly to the nasal side (toward the nose)
- Has NO photoreceptors → this creates the Blind Spot (a small area where you cannot see anything)
- Appears as a pale pinkish-white disc on fundus examination
- The central depression in the optic disc is called the Cup (physiological cup)
- Cup-to-Disc ratio (CDR): Normally < 0.5. If > 0.5, it may indicate Glaucoma (increased eye pressure causing damage)
- Located slightly temporal (toward the ear) to the optic disc
- The area of highest visual acuity (sharpest, most detailed vision)
- Rich in cones (color vision cells)
- Yellow due to xanthophyll pigment
- Appears darker than surrounding retina
- The absolute center of the macula
- Contains only cones (absolutely NO rods here)
- Site of the sharpest vision in the entire eye
- When you look directly at something, the image falls on the fovea
- The front border/edge of the retina, where it ends
- Here the retina merges with the ciliary body
PHOTORECEPTORS: RODS vs CONES
| Feature | RODS | CONES |
|---|---|---|
| Number | ~120 million | ~6-7 million |
| Location | Peripheral retina (sides) | Macula/Fovea (center) |
| Function | Night vision / dim light | Day vision / color vision |
| Speed | Slow | Fast |
| Colors detected | No (black & white only) | Yes (Red, Green, Blue) |
| Pigment | Rhodopsin (Visual Purple) | Photopsin (Iodopsin) |
- Rods = Radar in the dark (peripheral night vision)
- Cones = Color (bright day, color, detail)
💧 PART 3: The Chambers of the Eye & Aqueous Humor
Anterior Chamber
- Space between the Cornea (front) and the Iris + Lens (back)
- Filled with Aqueous Humor (clear, watery fluid)
- At the angle between cornea and iris is the Trabecular Meshwork and Canal of Schlemm (where aqueous drains out)
Posterior Chamber
- Narrow space between the Iris (front) and the Lens + Zonules (back)
- Also filled with Aqueous Humor
- Aqueous is produced here (by ciliary body processes) and flows FORWARD through the pupil into the anterior chamber
Vitreous Chamber (Posterior Cavity)
- Large space behind the lens, filling the entire back of the eye
- Filled with Vitreous Humor (a thick, gel-like, jelly substance)
- Vitreous is 99% water but has a gel consistency due to hyaluronic acid and collagen
- It gives the eyeball its round shape and supports the retina
- Unlike aqueous humor, vitreous does NOT circulate - it stays in place
- Age-related changes cause Vitreous Syneresis (liquefaction of vitreous gel) → leads to Floaters (tiny specks/cobwebs seen in vision)
Aqueous Humor — How It Is Made and Drained
- Made by the Ciliary Body (ciliary processes) in the posterior chamber
- Rate of production = 2 microliters/minute
- Process involves carbonic anhydrase enzyme (key for drug action)
- Composition: clear, protein-free, similar to blood plasma
Ciliary Body → Posterior Chamber → Through Pupil → Anterior Chamber → Trabecular Meshwork → Canal of Schlemm → Episcleral Veins → Blood
- If drainage is blocked → Aqueous builds up → Pressure inside eye (IOP) rises → GLAUCOMA
- Normal IOP = 10-21 mmHg (average ~15 mmHg)
- Drugs for glaucoma work by either reducing production (e.g., Timolol - beta blocker, Dorzolamide - carbonic anhydrase inhibitor) or increasing drainage (e.g., Pilocarpine, Latanoprost)
🔭 PART 4: The Lens
- Transparent, biconvex (curved on both sides) crystalline structure
- Located behind the iris, in front of the vitreous
- Held in place by the Zonules (Suspensory Ligament) which connect it to the ciliary body
- Has NO blood vessels, NO nerves - gets nutrition from aqueous humor
- Power of lens = +16 to +22 Diopters (can change with accommodation)
- Capsule: Outermost clear envelope
- Epithelium: Single layer just inside the anterior capsule - the only metabolically active cells
- Cortex: Outer softer part of the lens
- Nucleus: Hard central core
- Made of Alpha, Beta, and Gamma Crystallins (special proteins)
- Any damage to these proteins (UV light, diabetes, injury, age) causes them to become opaque = CATARACT (clouding of the lens)
👁️ PART 5: Extraocular Muscles (The 6 Muscles That Move the Eye)
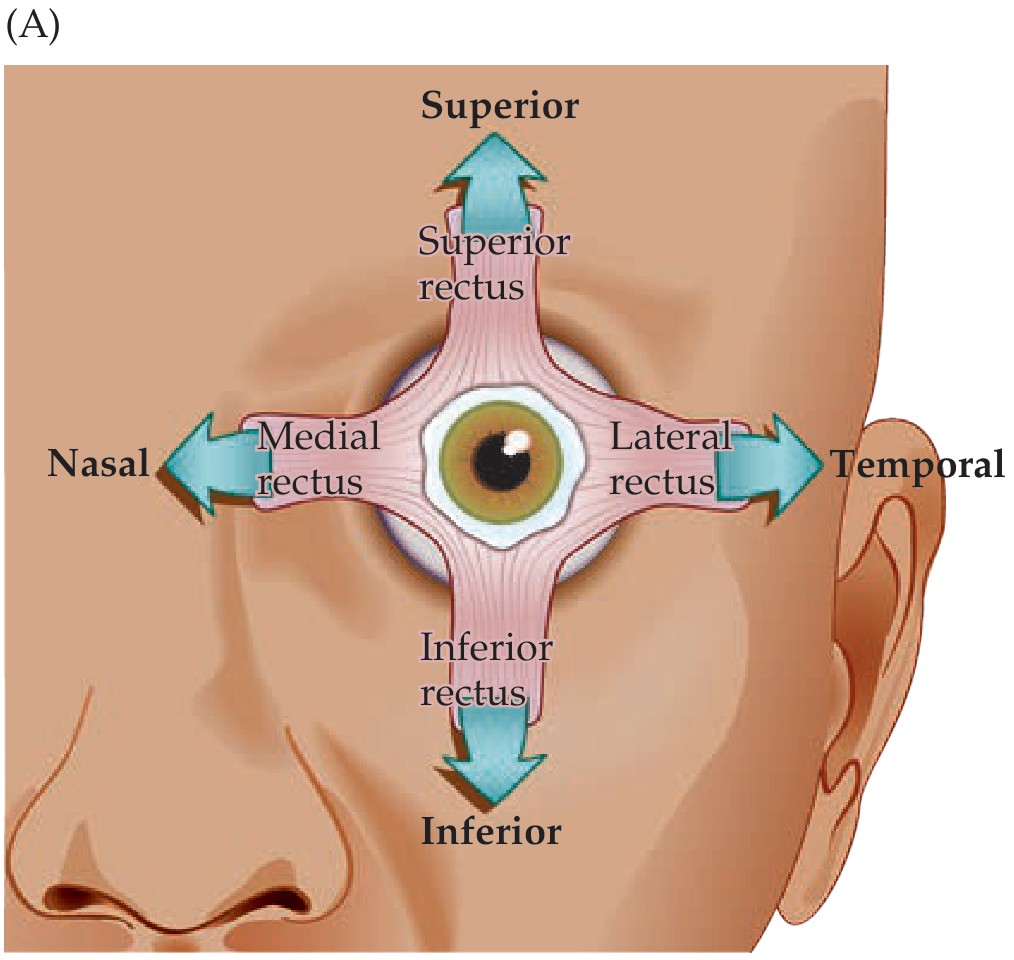
The 6 Muscles - Actions & Nerve Supply
| Muscle | Primary Action | Nerve Supply |
|---|---|---|
| Medial Rectus (MR) | Adduction (eye turns inward/toward nose) | CN III (Oculomotor) |
| Lateral Rectus (LR) | Abduction (eye turns outward/toward ear) | CN VI (Abducens) |
| Superior Rectus (SR) | Elevation (eye looks up) + Intorsion | CN III (Oculomotor) |
| Inferior Rectus (IR) | Depression (eye looks down) + Extorsion | CN III (Oculomotor) |
| Superior Oblique (SO) | Intorsion + Depression (when eye is adducted) | CN IV (Trochlear) |
| Inferior Oblique (IO) | Extorsion + Elevation (when eye is adducted) | CN III (Oculomotor) |
- Lateral Rectus = CN 6
- Superior Oblique = CN 4
- All the rest = CN 3 (Oculomotor)
- Intorsion = Top of the eye rotates toward the nose (inward tilt)
- Extorsion = Top of the eye rotates away from nose (outward tilt)
- To test Superior Rectus: Ask patient to look Up and Out
- To test Inferior Rectus: Ask patient to look Down and Out
- To test Superior Oblique: Ask patient to look Down and In (inward then down)
- To test Inferior Oblique: Ask patient to look Up and In
🩸 PART 6: Blood Supply of the Eye
| Branch | What It Supplies |
|---|---|
| Central Retinal Artery (CRA) | Enters the optic nerve → supplies inner 2/3 layers of retina |
| Short Posterior Ciliary Arteries | Supplies choroid and outer 1/3 of retina (via choriocapillaris) |
| Long Posterior Ciliary Arteries (2) | Supply the anterior uvea (iris and ciliary body) |
| Anterior Ciliary Arteries | Also supply the anterior uvea |
| Lacrimal Artery | Lacrimal gland and upper eyelid |
| Supraorbital Artery | Forehead and scalp |
- The Central Retinal Artery is an end artery (no collateral connections) - so if it blocks → sudden, complete, painless loss of vision (CRAO - Central Retinal Artery Occlusion)
- The inner retina gets blood from CRA; the outer retina gets nutrition from the choroid (via diffusion)
- Venous drainage: Central Retinal Vein → Ophthalmic Vein → Cavernous Sinus
😢 PART 7: Lacrimal System (Tear System)
- Main lacrimal gland: sits in the upper-outer part of the orbit (above and lateral to the eye)
- Also accessory lacrimal glands: Glands of Krause and Wolfring (in the eyelid)
- Normal tear production: 1-2 microliters/minute
- Schirmer's test: Measures tear production (normal ≥ 10 mm wetting in 5 minutes)
| Layer | Produced By | Function |
|---|---|---|
| Outer Lipid layer | Meibomian glands (in eyelids) | Prevents evaporation |
| Middle Aqueous layer | Lacrimal gland | Washes, nourishes, antibacterial |
| Inner Mucin layer | Goblet cells of conjunctiva | Helps tears stick to cornea |
- Presents as: painful swelling at the inner corner of the eye, discharge
- Common organisms: Staphylococcus, Streptococcus
🧠 PART 8: The Visual Pathway
The Journey of Light → Vision
Light enters eye
↓
Cornea (bends light - most of focusing)
↓
Pupil (controls amount of light)
↓
Lens (fine-tunes focusing)
↓
Retina (converts light to nerve signals)
↓
Optic Nerve (carries signals from one eye)
↓
Optic Chiasm (crossing point - very important!)
↓
Optic Tract (carries signals from both eyes)
↓
Lateral Geniculate Nucleus/LGN (relay station in thalamus)
↓
Optic Radiation (nerve fibers fan out in brain)
↓
Primary Visual Cortex (Occipital lobe - Area 17)
↓
VISION IS PERCEIVED!
The Optic Chiasm - Key Concept (⭐⭐⭐ Very NEET PG Important)
- Nasal (inner) fibers from each eye CROSS to the opposite side
- Temporal (outer) fibers from each eye DO NOT CROSS (stay on the same side)
- The Left Optic Tract carries visual information from the right side of your visual field (from both eyes)
- The Right Optic Tract carries visual information from the left side of your visual field (from both eyes)
Why does this matter for NEET PG?
| Location of Damage | Visual Field Loss |
|---|---|
| One optic nerve (before chiasm) | Blindness in that ONE eye only |
| Optic Chiasm (center) | Bitemporal Hemianopia (loss of both side/peripheral fields - "tunnel vision") - classic sign of pituitary tumor pressing on chiasm |
| Optic Tract (after chiasm) | Homonymous Hemianopia (loss of same half in BOTH eyes) |
| Temporal lobe (optic radiation) | Upper quadrantanopia (loss of upper quarter of vision in both eyes) - "Pie in the sky" |
| Parietal lobe (optic radiation) | Lower quadrantanopia (loss of lower quarter of vision) |
| Occipital cortex | Homonymous hemianopia with MACULAR SPARING (center of vision preserved) |
🧬 PART 9: Autonomic Innervation of the Eye
SYMPATHETIC SUPPLY (Fight or Flight)
Hypothalamus → Descends through brainstem and spinal cord → Exits at T1 → Cervical Sympathetic Chain → Superior Cervical Ganglion → Follows Internal Carotid Artery → Into the orbit
- Dilates the pupil (Mydriasis via dilator pupillae)
- Raises the upper eyelid (via Muller's muscle - partial eyelid elevator)
- Retracts the lower eyelid slightly
- Ptosis (drooping eyelid - due to Muller's muscle paralysis)
- Miosis (small pupil - dilator doesn't work)
- Anhidrosis (no sweating on the same side of face)
- Enophthalmos (slight sinking of the eyeball back into socket)
- Can be caused by: Pancoast tumor (lung cancer at apex), carotid artery dissection, neck tumors
PARASYMPATHETIC SUPPLY (Rest and Digest)
Edinger-Westphal nucleus (in CN III origin) → CN III (Oculomotor nerve) → Ciliary Ganglion (in orbit) → Short Ciliary Nerves → Eye
- Constricts the pupil (Miosis via sphincter pupillae)
- Controls accommodation (ciliary muscle contraction for near vision)
- Fixed dilated pupil (mydriasis - sphincter paralyzed)
- Ptosis (most of upper lid elevation is CN III)
- Eye turns DOWN and OUT (other muscles are also CN III)
🧪 PART 10: The Conjunctiva
- Covers the white of the eye (bulbar conjunctiva - over sclera)
- Lines the inside of the eyelids (palpebral conjunctiva - inside lid surface)
- The fold where they meet is called the Fornix (like a pocket)
- Protects the eye surface
- Contains goblet cells → secretes mucin (inner layer of tear film)
- Acts as a pocket/pouch - you can put eye drops here (lower fornix)
💊 PART 11: DISEASE-BASED PRESCRIPTION NOTES
🩺 Rx 1 — Dry Eye Syndrome
Patient Name: ___________
Date: ___________
Diagnosis: Dry Eye Syndrome (Keratoconjunctivitis Sicca)
Rx:
1. Carboxymethylcellulose (CMC) 0.5% Eye Drops
(Artificial tears / lubricating drops)
- Instill 1 drop in each eye, 4-6 times a day
- Use as needed for dryness/irritation
2. Sodium Hyaluronate 0.1% Eye Drops
(Lubricating gel-type drops - longer lasting)
- Instill 1 drop in each eye, 3-4 times a day
3. Carbomer Gel (Lacrigel/Viscotears)
- Apply small amount in lower fornix at bedtime
(Thicker lubricant for overnight use)
4. Omega-3 Fatty Acids 1000mg capsule
- Take 1 capsule twice daily with food
(Improves the lipid layer of tear film)
Advice:
- Avoid air-conditioned environments / screen time without blinking
- Use humidifier in room if dry climate
- Follow-up in 4 weeks with Schirmer's test
🩺 Rx 2 — Dacryocystitis (Acute)
Patient Name: ___________
Date: ___________
Diagnosis: Acute Dacryocystitis (Right/Left eye)
Rx:
1. Moxifloxacin 0.5% Eye Drops
- Instill 1 drop in affected eye every 6 hours
2. Tab. Amoxicillin + Clavulanic Acid 625mg
- Take 1 tablet orally, twice daily for 7 days
(Antibiotic - for systemic treatment of infection)
OR
Cefalexin 500mg - 1 tab orally four times daily x 7 days
3. Tab. Ibuprofen 400mg (Anti-inflammatory)
- Take 1 tablet orally three times daily with food (for pain and swelling)
4. Hot Fomentation (applying warm cloth over the area)
- Apply 3-4 times daily for 10-15 minutes
Advice:
- Warm compress to soften the blocked duct
- Do NOT squeeze the swelling
- If abscess forms: incision and drainage needed
- Definitive surgical treatment: DCR (Dacryocystorhinostomy - making a new drainage passage)
- Follow up in 1 week
⭐ PHASE 1 — NEET PG HIGH-YIELD SUMMARY BOX
| Topic | High-Yield Fact |
|---|---|
| Corneal layers | 5 layers: E-B-S-D-E (Every Body Should Drink Enough) |
| Lens power | Cornea = +43D; Lens = +16-22D; Total = ~+60D |
| Aqueous drainage | Canal of Schlemm via trabecular meshwork |
| Normal IOP | 10-21 mmHg |
| Extraocular muscles | LR6, SO4, rest 3 (CN VI, IV, III) |
| Optic chiasm lesion | Bitemporal Hemianopia = Pituitary tumor |
| Fovea has | ONLY cones (no rods) - site of best vision |
| Rods use | Rhodopsin (needs Vitamin A) |
| Horner's Syndrome | Ptosis + Miosis + Anhidrosis = Sympathetic damage |
| Aqueous humor | Made by ciliary body; drained via Schlemm's canal |
| End artery in eye | Central Retinal Artery (blocks = CRAO) |
| Weakest point of sclera | Lamina Cribrosa |
| Schirmer's test | Normal ≥ 10 mm in 5 min (dry eye if less) |
| Vitamin A deficiency | Night blindness (rhodopsin cannot be made) |
🧠 MNEMONICS SUMMARY FOR PHASE 1
| Mnemonic | What it helps remember |
|---|---|
| "Every Body Should Drink Enough" | 5 layers of cornea (Epithelium-Bowman's-Stroma-Descemet's-Endothelium) |
| "LR6 SO4 Rest 3" | Nerve supply of extraocular muscles |
| "SIN - Super Is Nasal" | Superior oblique = Intorsion (top goes Nasal) |
| "Bitemporal = B = pituBary" | Bitemporal hemianopia = pituitary tumor at chiasm |
| Dark = Dilate = Sympathetic | Sympathetic → dilates pupil |
| Light = constrict = paraSymP | Parasympathetic → constricts pupil |
✅ END OF PHASE 1
- The 3 coats of the eye (Fibrous, Uveal, Nervous)
- Cornea, Sclera, Iris, Ciliary Body, Choroid, Retina in detail
- Aqueous humor production and drainage
- 6 extraocular muscles with nerve supply
- Blood supply of the eye
- Lacrimal system
- Visual pathway from eye to brain
- Autonomic control of the pupil
Phase 2
🔵 PHASE 2 — Optics and Refraction
Complete Detailed Lesson | Concept + NEET PG
🌟 START HERE: Think of the Eye Like a Camera Zoom Lens
The science of how light bends through lenses and focuses on the retina = OPTICS The error when focus does not land exactly on the retina = REFRACTIVE ERROR
📐 PART 1: Basic Optics — Understanding Light and Lenses
What is Refraction?
What is a Diopter (D)?
- Positive (+) Diopter = Converging lens (brings light rays together = convex lens)
- Negative (-) Diopter = Diverging lens (spreads light rays apart = concave lens)
Power (in Diopters) = 1 / Focal length (in meters)
The Refracting Power of the Eye
| Structure | Power | Type of Lens |
|---|---|---|
| Cornea | +43 Diopters (fixed, cannot change) | Convex |
| Lens | +16 to +26 Diopters (variable, changes with accommodation) | Convex (biconvex) |
| Total eye (at rest) | ~+60 Diopters | - |
What is the "Far Point" and "Near Point"?
- Far Point = The farthest distance at which an eye can see clearly WITHOUT using any accommodation (lens relaxed). In a normal eye = Infinity.
- Near Point = The closest distance at which an eye can see clearly WITH maximum accommodation. In a young adult = ~10 cm.
🔭 PART 2: Accommodation — How the Eye Adjusts Focus
How does it work?
- The ciliary muscle CONTRACTS (tightens like a ring getting smaller)
- This RELAXES the tension on the zonular fibers (the lens's "support wires")
- The lens becomes thicker and more curved (like a bulging ball)
- Lens power increases → more bending → near object comes into focus
- Ciliary muscle RELAXES
- Zonular fibers become TAUT (tight)
- Lens becomes flatter and thinner
- Lens power decreases → just the right bending for distant objects
Near = Ciliary contracts, zonule relaxes, lens bulges (gets fat) Far = Ciliary relaxes, zonule tightens, lens flattens (gets thin)
Amplitude of Accommodation
- = Maximum power the eye can add through accommodation
- Young child: ~14 Diopters
- Young adult (20 years): ~10 Diopters
- Age 40: ~5 Diopters
- Age 60+: ~1 Diopter or ZERO → This is why old people need reading glasses!
👁️ PART 3: Emmetropia — The Normal Eye
- When the eye is at REST (no accommodation), parallel rays of light from infinity focus exactly ON the retina
- Far point = Infinity
- Such a person can see far clearly without glasses
- Can see near by using accommodation
Think of it as: "The camera is perfectly set up — everything in focus when relaxed"
🔴 PART 4: Myopia (Short-sightedness / Nearsightedness)
What is Myopia?
Why does Myopia happen?
- Axial Myopia (most common) - The eyeball is too long (too much axial length). Light focuses before retina.
- Refractive Myopia - The cornea or lens is too curved (too powerful), so it bends light too much.
Symptoms of Myopia
- Cannot see distant objects clearly (blackboard, TV, faces)
- Can see near objects (phone, books) perfectly
- Often squints eyes to try to see better
- Headaches
How is Myopia measured?
- Mild myopia: -0.5 D to -3 D
- Moderate myopia: -3 D to -6 D
- High myopia: > -6 D
Far Point in Myopia
- Example: -2 D myopia → Far point = 50 cm in front of eye
How to Correct Myopia?
🔵 PART 5: Hypermetropia (Hyperopia / Long-sightedness / Farsightedness)
What is Hypermetropia?
Why does it happen?
- Axial Hypermetropia (most common) - The eyeball is too short (too small axial length)
- Refractive Hypermetropia - The cornea or lens is too flat (too weak)
Symptoms of Hypermetropia
- Young person with mild hypermetropia: sees FINE (accommodation compensates)
- Young person with high hypermetropia: has difficulty with near tasks, headaches, eye strain
- Older person with any hypermetropia: vision blurs especially at near (as accommodation power decreases with age)
- Convergent squint (eyes cross inward) in children with hypermetropia — because the extra accommodation needed for focus also causes the eyes to converge (turn in) → This is called Accommodative Esotropia (eye turns inward due to hypermetropia)
Types of Hypermetropia
| Type | Meaning |
|---|---|
| Latent Hypermetropia | Hidden - fully compensated by accommodation (not detected without cycloplegic refraction) |
| Manifest Hypermetropia | Part not compensated by accommodation |
| Facultative | Can be compensated by accommodation but with effort |
| Absolute | Cannot be compensated even with max accommodation |
| Total Hypermetropia | = Latent + Manifest (only measured after cycloplegia - paralysis of accommodation) |
How to Correct Hypermetropia?
🟡 PART 6: Astigmatism — "Two Focuses"
What is Astigmatism?
Imagine: A normal cornea is like a basketball (same curve all around). An astigmatic cornea is like a rugby ball (different curves in different directions).
Types of Astigmatism
- Regular Astigmatism - The two principal meridians are perpendicular (at 90° to each other). Correctable with cylindrical lenses.
- Irregular Astigmatism - Meridians are NOT perpendicular. Common in keratoconus (cone-shaped cornea). NOT correctable with glasses alone - needs contact lenses or surgery.
- Simple Myopic Astigmatism - One focus on retina, other in front
- Simple Hypermetropic Astigmatism - One focus on retina, other behind
- Compound Myopic Astigmatism - Both foci in front of retina
- Compound Hypermetropic Astigmatism - Both foci behind retina
- Mixed Astigmatism - One in front, one behind (most blurry!)
- With-the-Rule (WTR) - Vertical meridian is steeper. Common in young people. Corrected with plus cylinder at 90°.
- Against-the-Rule (ATR) - Horizontal meridian is steeper. Common in elderly.
- Oblique Astigmatism - Steepest meridian is between 30°-60° or 120°-150°.
How to Correct Astigmatism?
- A sphero-cylindrical lens (sphere + cylinder combined) corrects most astigmatism
🟠 PART 7: Presbyopia — "Old Eyes"
What is Presbyopia?
When does it start?
- Usually noticed around age 40-45 years
- Person holds reading material farther and farther away ("arm's length reading")
- Difficulty reading fine print, threading needles, near work
What happens?
- Lens proteins change → Lens nucleus hardens → Nuclear Sclerosis
- The lens cannot bulge/change shape even when ciliary muscle contracts
- Therefore near objects cannot be brought into focus
Important Difference:
| Condition | Problem | Age |
|---|---|---|
| Hypermetropia | Eyeball too short / cornea too flat (structural) | Any age |
| Presbyopia | Lens too hard to accommodate (functional aging) | 40+ years |
How to Correct Presbyopia?
- LASIK monovision (one eye corrected for near, other for far)
- Conductive Keratoplasty (CK) - mild radiofrequency burns to steepen cornea
- Presbyopia-correcting IOL (multifocal lens implant)
📊 PART 8: Summary Table — All Refractive Errors at a Glance
| Feature | Myopia | Hypermetropia | Astigmatism | Presbyopia |
|---|---|---|---|---|
| Common name | Short-sighted | Long-sighted | "Rugby ball eye" | Old-age reading difficulty |
| Problem | Eye too long OR cornea too curved | Eye too short OR cornea too flat | Unequal corneal curves | Lens too hard (aging) |
| Focus point | IN FRONT of retina | BEHIND retina | Two focal points | Cannot accommodate |
| Blurred vision | FAR (distance) | NEAR (especially with age) | ALL distances | NEAR only |
| Correction lens | Concave (-ve, diverging) | Convex (+ve, converging) | Cylindrical | Convex (+) for reading |
| NEET PG number | -ve Diopters | +ve Diopters | Cylinder axis given | +1 to +3 D for reading |
🔬 PART 9: Important Optics Instruments (High-Yield NEET PG!)
1. Snellen's Chart (Visual Acuity Test)
- The standard chart with rows of letters of decreasing size
- Patient reads from 6 meters distance (or 20 feet)
- Recorded as a fraction: 6/6 (normal) or 6/60 etc.
- Numerator = distance patient is standing (6 meters)
- Denominator = distance at which a normal eye should read that line
- 6/6 = Normal vision (can read at 6 m what should be read at 6 m)
- 6/60 = Very poor vision (can only read at 6 m what a normal eye reads at 60 m)
- CF (Counting Fingers) - Can count fingers held up close
- HM (Hand Movements) - Can only see hand waving
- PR (Perception of Light) - Can only tell if light is on/off
- NPL (No Perception of Light) - Completely blind
2. Retinoscope
- An instrument used to find the actual refractive error of the eye
- The doctor shines a light into the patient's eye and observes the reflection (reflex)
- Used for objective refraction (no response needed from the patient — great for children and infants!)
- The "with" movement of the reflex = Hypermetropia
- The "against" movement of the reflex = Myopia
- Neutralization = When the reflex no longer moves → that's the correct lens power
3. Autorefractometer / Keratometer
- Autorefractometer = A computerized machine that automatically measures refractive error
- Keratometer (Ophthalmometer) = Measures the curvature of the cornea (detects astigmatism, used before contact lens fitting and LASIK surgery)
- Keratometer measures corneal power in diopters
4. Slit Lamp
- The main eye examination microscope
- Used for detailed examination of all anterior segment structures
5. Lensometer (Focimeter / Vertometer)
- Used to measure the power of a lens already present in glasses
- Determines the exact correction in a patient's existing spectacles
🔭 PART 10: Refractive Surgery — LASIK and Others
What is Refractive Surgery?
LASIK (Laser-Assisted In Situ Keratomileusis)
- A thin flap of corneal tissue is created (with a microkeratome blade OR femtosecond laser)
- Flap is lifted up
- Excimer laser (ultraviolet laser) removes a precise amount of corneal tissue from underneath
- Flap is placed back → heals without stitches
- Myopia: up to -10 to -12 D (depending on corneal thickness)
- Hypermetropia: up to +4 D
- Astigmatism: up to +/-5 D
- Age ≥ 18 years (stable prescription)
- Stable refraction for at least 1 year (no significant change)
- Adequate corneal thickness (minimum ~500 microns)
- No keratoconus (cone-shaped cornea - absolute contraindication)
- Keratoconus
- Dry eye (gets worse after LASIK)
- Thin cornea
- Unstable/progressing myopia
- Pregnancy
- Autoimmune diseases (SLE, RA)
- Active corneal disease
PRK (Photorefractive Keratectomy)
- Older surface ablation technique
- No flap is made — epithelium is removed and laser applied directly to surface
- Slower recovery, more pain than LASIK
- Suitable when cornea is too thin for LASIK
LASEK (Laser Epithelial Keratomileusis)
- A modification of PRK — epithelial sheet is moved aside (not cut off)
- Intermediate between PRK and LASIK
SMILE (Small Incision Lenticule Extraction)
- Newest laser technique
- No flap created — a small lenticule (disc of corneal tissue) is cut inside the cornea and removed through a tiny incision
- Advantages: No flap complications, less dry eye, quicker
- Used for myopia and myopic astigmatism
Phakic IOL (Implantable Collamer Lens / ICL)
- A lens is implanted inside the eye (between iris and natural lens) without removing the natural lens
- Used for very high myopia (too high for LASIK or cornea too thin)
- Types: Iris-clip lens (anterior chamber), ICL/Visian ICL (posterior chamber)
🔋 PART 11: Contact Lenses
- Soft contact lenses - Most popular, comfortable, daily/monthly wear
- Rigid Gas Permeable (RGP) lenses - Better optics, lasts longer, best for irregular astigmatism
- Orthokeratology - Special lenses worn at night to temporarily reshape cornea
- Correction of myopia, hypermetropia, astigmatism
- Cosmetic use (colored lenses)
- RGP lenses are the best correction for Keratoconus (irregular astigmatism)
- Bandage contact lenses - placed on cornea after surgery to protect it while healing
- Corneal ulcers (especially Pseudomonas, Acanthamoeba)
- Giant Papillary Conjunctivitis (GPC - bumps inside upper eyelid from allergic reaction to lens protein deposits)
- Dry eye
- Corneal hypoxia (oxygen deprivation) from overwearing
⭐ PART 12: NEET PG High-Yield One-Liners — Optics
| Fact | Answer |
|---|---|
| Correction for myopia | Concave lens (-D) |
| Correction for hypermetropia | Convex lens (+D) |
| Correction for astigmatism | Cylindrical lens |
| Correction for presbyopia | Convex (+) reading lens |
| Normal visual acuity | 6/6 |
| Normal near vision Snellen equivalent | N6 / Jaeger 1 |
| Legal blindness (India) | < 6/60 in better eye |
| Absolute blindness | < 3/60 (profound blindness) |
| Instrument to measure corneal curvature | Keratometer |
| Instrument to measure glasses power | Lensometer / Focimeter |
| Objective refraction in children | Retinoscopy under cycloplegia |
| Best correction for keratoconus | RGP contact lenses |
| Absolute contraindication for LASIK | Keratoconus |
| Myopia is corrected by | Making cornea flatter (ablate center) |
| Hypermetropia is corrected by | Making cornea steeper (ablate periphery) |
| Presbyopia begins at | ~40-45 years |
| Cycloplegic used in children | Atropine 1% |
| Cycloplegic quick acting (adults) | Tropicamide 1% |
| Refractive index of cornea | ~1.376 |
| Refractive index of aqueous | ~1.336 |
| Diameter of cornea (horizontal) | ~12 mm |
| Cornea provides how much power | +43 Diopters |
💊 PART 13: DISEASE-BASED PRESCRIPTION NOTES
🩺 Rx 1 — Myopia (Simple, Mild-Moderate)
Patient Name: ___________ Age: 18 yrs
Date: ___________
Diagnosis: Simple Myopia (Right eye: -3.0 D Sph, Left eye: -2.75 D Sph)
Rx (Spectacle Prescription):
Right Eye: Sph -3.00 D Cyl: Nil Axis: -
Left Eye: Sph -2.75 D Cyl: Nil Axis: -
Advice:
- Wear glasses for distance vision at all times
- Good lighting while reading; avoid reading in lying position
- Regular annual eye checkup (for progression)
- Reduce prolonged near work / screen time
- Annual dilated fundus exam (for high myopia - check retina)
If surgery planned (age ≥ 18 with stable Rx for 1 year):
- Counseling for LASIK / ICL depending on corneal thickness
- Pachymetry (corneal thickness test) before surgery
🩺 Rx 2 — Hypermetropia with Accommodative Esotropia (Child)
Patient Name: ___________ Age: 5 yrs
Date: ___________
Diagnosis: Hypermetropia with Accommodative Esotropia (eye crossing inward)
Cycloplegic Refraction: Right Eye +4.0 D, Left Eye +3.5 D
Step 1: CYCLOPLEGIC DROPS for refraction
Atropine 1% Eye Ointment
- Apply in both eyes, twice daily for 3 days before refraction appointment
Rx (Spectacle Prescription - full cycloplegic correction):
Right Eye: +4.00 D Left Eye: +3.50 D
(Glasses must be worn FULL TIME to reduce the eye crossing)
Advice:
- Full-time glasses wear is mandatory
- The squint may correct completely once glasses are worn consistently
- Follow up every 3-6 months
- Amblyopia (lazy eye) treatment: if one eye is weaker, patching of the stronger eye will be advised
- Surgery may be needed if squint does not fully correct with glasses
🩺 Rx 3 — Presbyopia (Age 45+, Previous Emmetrope / No Glasses Before)
Patient Name: ___________ Age: 45 yrs
Date: ___________
Diagnosis: Presbyopia (Difficulty reading fine print, holding books at arm's length)
Distance Vision: Normal (6/6 both eyes, no correction needed for distance)
Reading Glasses Prescription:
Right Eye: +1.50 D Sph Left Eye: +1.50 D Sph
(Reading addition of +1.50 D)
Advice:
- Wear these glasses ONLY for near tasks (reading, phone, needlework)
- Adequate lighting while reading
- Prescription will need to be increased every 2-3 years as condition progresses
- By age 60, may need +2.5 to +3.0 D
Note to patient: This is a normal aging process. Everyone develops presbyopia.
Follow-up: Annual check
🩺 Rx 4 — Presbyopia in a Myope (Most Common Type in Clinical Practice)
Patient Name: ___________ Age: 48 yrs
Date: ___________
Diagnosis: Myopia + Presbyopia (Distance blur + new reading difficulty)
Spectacle Prescription (BIFOCAL or Progressive):
Distance vision:
Right Eye: -3.00 D Sph Left Eye: -2.75 D Sph
Near addition (for reading):
Add: +2.00 D both eyes
Therefore:
Right Eye Near: -3.00 + 2.00 = -1.00 D Sph
Left Eye Near: -2.75 + 2.00 = -0.75 D Sph
Options:
1. Bifocal glasses (distance top, reading bottom - visible line)
2. Progressive/Varifocal glasses (gradual change, no line - cosmetically preferred)
Advice:
- Give time to adjust to progressive lenses (1-2 weeks)
- Do not look through bottom of lens when walking down stairs
🧠 MNEMONICS SUMMARY FOR PHASE 2
| Mnemonic | What It Helps Remember |
|---|---|
| "Myopia = Minus, Near OK" | Myopia corrected with Minus/Concave lens; Near vision fine |
| "Hypermetropia = Help with Plus" | Hypermetropia corrected with Plus/Convex lens |
| "Cylinders for Astigmatism" | Astigmatism → Cylindrical lens |
| "Presbyopia = Presbyter = Old Priest = +1.5 reading glasses" | Age 40+ → +reading glasses |
| "Near = ciliary Narrows (contracts)" | Near vision = ciliary muscle contracts |
| "LASIK flap, PRK scrape" | LASIK makes a flap; PRK scrapes surface epithelium |
| "Keratoconus = Kill LASIK" | Keratoconus is absolute contraindication for LASIK |
| "6/6 = Snellen Normal" | Normal Snellen visual acuity |
⭐ PHASE 2 — NEET PG HIGH-YIELD SUMMARY BOX
| Topic | High-Yield Fact |
|---|---|
| Type of lens for myopia | Concave (-) |
| Type of lens for hypermetropia | Convex (+) |
| Type of lens for astigmatism | Cylindrical |
| Presbyopia starts at | 40-45 years |
| Accommodative esotropia cause | Hypermetropia |
| Cycloplegic for children | Atropine 1% (gold standard) |
| Legal blindness India | < 6/60 |
| Absolute contraindication LASIK | Keratoconus |
| Best correction for keratoconus | RGP contact lenses |
| Retinoscopy "with" reflex | Hypermetropia |
| Retinoscopy "against" reflex | Myopia |
| Instrument for corneal curvature | Keratometer |
| Instrument for glasses power | Lensometer / Focimeter |
| Snellen test distance | 6 meters |
| Far point of emmetrope | Infinity |
| Presbyopia correction | + convex reading glasses |
| Near point of emmetrope (20 yr) | ~10 cm |
| ICL / Phakic IOL used for | Very high myopia (cornea too thin for LASIK) |
✅ END OF PHASE 2
- What refraction is and how the eye focuses light
- Diopters and lens types (concave vs convex)
- All 4 refractive errors: Myopia, Hypermetropia, Astigmatism, Presbyopia
- Accommodation - how the lens changes shape
- How to read and write a basic spectacle prescription
- LASIK, PRK, SMILE, ICL - what each is for
- Contact lenses and their complications
- Snellen chart, Retinoscope, Keratometer