Dental amalgam
Reading File
Finding Sources
Searching the Web
dental amalgam composition properties clinical use 2024
Searching PubMed
dental amalgam
Finding Sources
Reading Web Page
dental amalgam composition properties clinical use safety
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information to write a thorough answer. Let me compile everything.
Dental Amalgam
What Is It?
Dental amalgam is one of the oldest and most studied restorative materials in dentistry, having been in use for over 150 years. It is a metallic alloy made by combining liquid (elemental) mercury (Hg⁰) with a powdered alloy of silver, tin, copper, and trace amounts of zinc and other metals. The liquid mercury - which constitutes approximately 50% by weight - gives the freshly mixed amalgam its initial plasticity, allowing it to be condensed and shaped into a prepared cavity before it hardens through an exothermic setting reaction.
The resulting set material is:
- Hard and durable
- Highly radiopaque on dental radiographs
- Silver-grey ("silver filling") in appearance
- Resistant to secondary caries, partly due to antibacterial properties
Composition
| Component | Approximate % |
|---|---|
| Mercury (Hg) | ~50% by weight |
| Silver (Ag) | ~35% |
| Tin (Sn) | ~9% |
| Copper (Cu) | ~6% |
| Zinc, others | trace |
The ANSI/ADA Standard No. 1 (ISO 1559) specifies physical property requirements including:
- Creep: maximum 1.0%
- Dimensional change: -0.15% to +0.20%
- Compressive strength: minimum 80 MPa at 1 hour, minimum 300 MPa at 24 hours
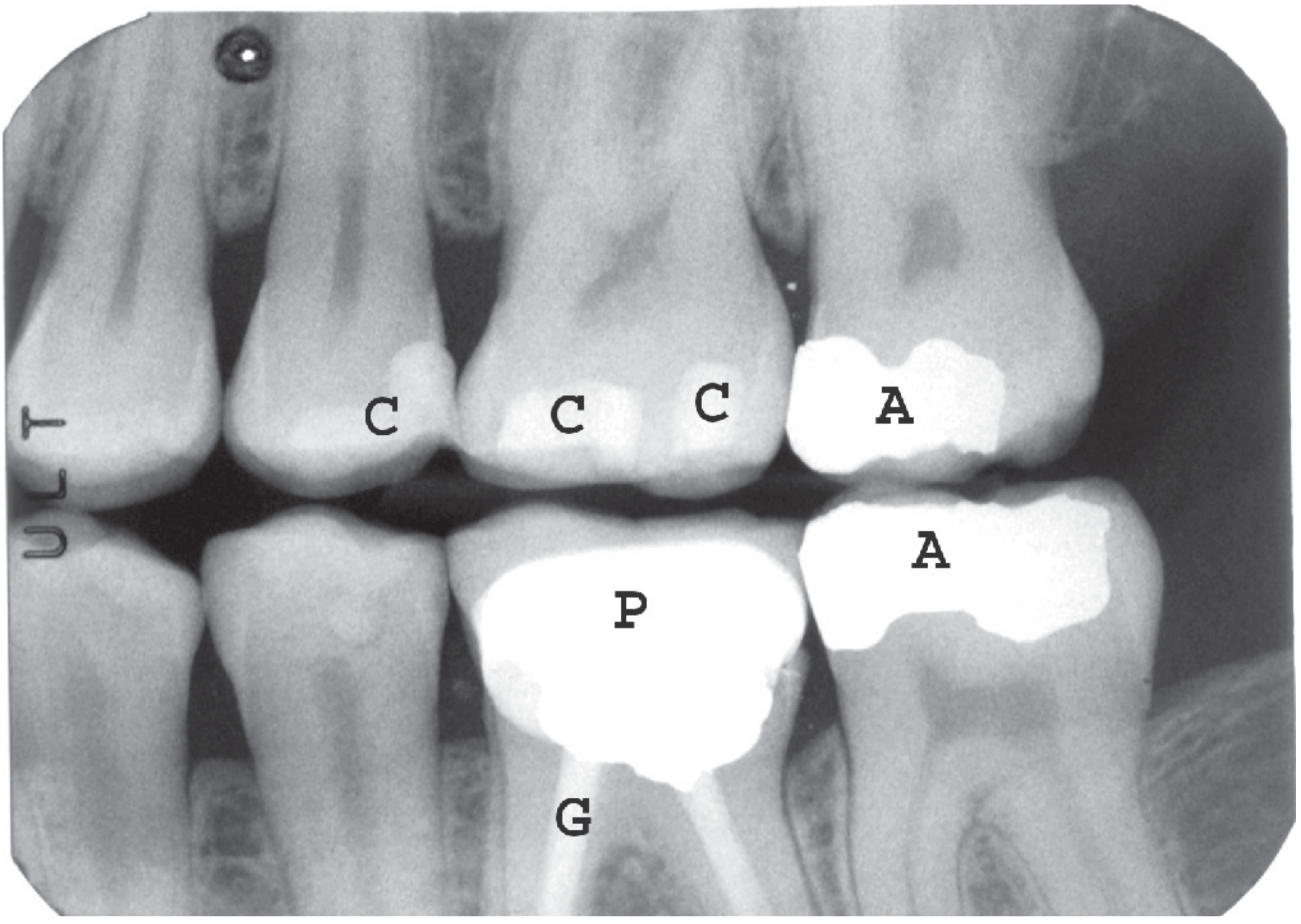
Radiographic Appearance
Amalgam fillings are highly radiopaque on dental X-rays, making them easy to identify. They can replace one or all five surfaces of a posterior tooth. In forensic settings, amalgam restorations are particularly useful for dental identification because their radiographic appearance, size, and shape are highly individualized.
Clinical Properties and Advantages
- Ease and speed of placement - faster to place than composite resin, especially in moisture-prone environments
- Longevity - well-placed amalgam restorations can last 10-15+ years
- Cost - generally less expensive than tooth-colored alternatives
- Antibacterial effect - release of metal ions inhibits biofilm at margins
- Tolerant of moisture - can be placed in difficult-to-isolate areas where composite bonding would fail
- Reparable - defective restorations can often be repaired rather than replaced
Mercury and Safety
Chemistry of Mercury in Amalgam
Three forms of mercury are relevant to human health (Goodman & Gilman):
| Form | Source | Toxicity |
|---|---|---|
| Elemental Hg⁰ | Dental amalgam, vapor inhalation | Moderate (vapor is toxic; ingested Hg⁰ is largely non-toxic) |
| Inorganic Hg²⁺ | Industrial, oxidation of Hg⁰ | Nephrotoxic, immunogenic |
| Methylmercury (CH₃Hg⁺) | Contaminated fish, microbial conversion | Highly neurotoxic, lipophilic |
From set amalgam fillings, a small amount of mercury vapor is continuously released, particularly during chewing, bruxism, or hot food/drink exposure. This vapor is absorbed through the lungs (approximately 70-80% absorption efficiency) and distributed throughout the body.
Mechanisms of Mercury Toxicity
Mercury exerts toxicity through three main mechanisms (Tietz Textbook of Laboratory Medicine):
- Sulfhydryl binding - Hg²⁺ avidly reacts with -SH groups of proteins, altering tertiary structure and abolishing biological activity; the kidney is the primary target organ
- Autoimmune/immunogenic effects - Structural protein changes render them immunogenic, triggering B-lymphocyte proliferation; collagen tissues are particularly sensitive
- Lipophilic neuronal binding - Alkyl mercury species (e.g. methylmercury) bind proteins in lipid-rich tissue; myelin is particularly susceptible
Does Amalgam Cause Harm?
Multiple systematic reviews and regulatory bodies (WHO, EU SCENIHR, FDA, IADR) have concluded that dental amalgam is safe for the general population. Mercury levels from amalgam fillings remain below regulatory concern thresholds in non-vulnerable individuals.
Contraindications / populations requiring extra caution:
- Allergy to amalgam components (mercury, nickel, tin)
- Severe renal disease (impaired mercury excretion)
- Pregnant women and young children (some guidelines recommend avoiding new amalgam placements)
- Patients with neurological conditions where additional mercury exposure may be inadvisable
Oral Mucosal Complications
Amalgam Tattoo
The most common cause of acquired oral pigmentation. Fragments of silver amalgam are traumatically implanted into adjacent oral mucosa - typically the gingiva, alveolar mucosa, or floor of mouth - during dental procedures. It appears as:
- Well-defined, grayish-black macular discoloration
- Asymptomatic, benign
- Highly radiopaque fragments may be visible on X-ray
(Cummings Otolaryngology; Dermatology 2-Volume Set 5e)
Lichenoid Contact Reactions
Amalgam metals - especially mercury, copper, zinc, and tin - can cause lichenoid reactions in the oral mucosa. Lesions are characteristically:
- Topographically related to the amalgam filling (adjacent mucosa)
- Patients may be patch-test positive to mercury or other metals
- Removal of the amalgam resolves the lesions in most cases
(Andrews' Diseases of the Skin)
Regulatory and Environmental Status
- The EU provisionally agreed (February 2024) to prohibit dental amalgam use from January 1, 2025 due to environmental mercury concerns (Minamata Convention on Mercury)
- The US FDA issued rules in 2010 reclassifying amalgam and specifying special controls
- The BDA (British Dental Association, 2024) argues that a complete phase-out without adequate alternatives risks worsening oral health inequalities, as amalgam remains the only feasible option in some clinical scenarios (lack of isolation, disability, dementia)
- Environmental impact relates to amalgam waste in dental wastewater and cremation emissions
Alternatives
| Material | Advantages | Disadvantages vs. Amalgam |
|---|---|---|
| Composite resin | Tooth-colored, bonds to tooth | Moisture-sensitive, shorter lifespan in large cavities, more technique-sensitive |
| Glass ionomer cement (GIC) | Fluoride release, bonds to tooth | Lower strength, wears faster |
| Ceramics/Porcelain | Durable, aesthetic | Requires lab fabrication, higher cost |
| Resin-modified GIC | Combined properties | Intermediate strength |
Recent Evidence (PubMed, 2024-2026)
- Al-Sulimmani et al. (2025) - Systematic review and meta-analysis comparing failure risk of composite resin vs. amalgam restorations [PMID: 40578032]
- Shaw et al. (2026) - Systematic review of health impacts of amalgam vs. alternative restorative materials [PMID: 41643924]
- Hatipoglu et al. (2024) - Meta-analysis on repair vs. replacement of defective direct restorations [PMID: 38796090]
Sources:
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Heavy Metals chapter
- Tietz Textbook of Laboratory Medicine, 7th Ed. - Mercury: Sources, Toxicokinetics
- Brogdon's Forensic Radiology - Dental Restorative Materials
- Andrews' Diseases of the Skin - Lichenoid Reactions
- Cummings Otolaryngology - Amalgam Tattoo
- IADR Safety of Dental Amalgam (2024)
- ADA Amalgam Topic
- BDA Position Paper, February 2024
I am bds student so consider books of it
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
dental amalgam BDS dental materials composition setting reaction manipulation clinical steps
Reading Web Page
dental amalgam composition classification setting reaction manipulation properties BDS
I now have all the BDS-level content needed. Let me write a thorough, exam-oriented answer for a BDS student.
Dental Amalgam - BDS Level Notes
Note: The textbook library does not include BDS-specific dental materials books (Phillips' Science of Dental Materials, Craig's Restorative Dental Materials, etc.), but the content below is compiled from standard BDS dental materials curriculum sources aligned with those texts.
Definition
An amalgam is formed when an alloy of two or more metals is mixed with mercury - this reaction is called amalgamation. Dental amalgam is the product of amalgamation between mercury and an alloy containing silver, tin, copper, and sometimes zinc/other elements.
According to Skinner: "Amalgam is a special type of alloy in which mercury is one of the metals."
History (Key Points)
- 1826 - Auguste Taveau (France) first used silver-mercury paste
- 1833 - Crawcour brothers introduced it in USA ("Royal Mineral Succedaneum")
- 1895 - GV Black standardized cavity preparation and amalgam formula
- 1963 - Innes & Youdelis introduced high-copper admixed alloy
- 1970s - Single-composition high-copper alloys developed
Classification
1. By Copper Content
| Type | Cu % | Key Feature |
|---|---|---|
| Low-copper (conventional) | < 6% | Contains γ2 phase - weak, corrosion-prone |
| High-copper admixed | 13-30% | γ2 nearly eliminated |
| High-copper unicomposition (single-composition) | 13-30% | γ2 completely eliminated |
2. By Particle Shape
- Lathe-cut (irregular) - ground ingot, irregular particles; requires more mercury
- Spherical - atomized particles; needs less mercury, less condensation pressure
- Spheroidal (admixed) - mix of lathe-cut + spherical
3. By Zinc Content
- Zinc-containing (>0.01% Zn) - Zinc acts as scavenger for oxygen during manufacturing; more prone to delayed expansion if contaminated with moisture
- Zinc-free - no delayed expansion risk
4. By Particle Size
- Coarse cut, Fine cut, Microcut (finer particles = faster reaction, faster strength gain)
5. By Generation
1st through 6th generation alloys (each with incremental improvements)
Composition
Alloy Powder Composition (pre-mercury)
| Element | % | Role |
|---|---|---|
| Silver (Ag) | ~65-70% | Strength, hardness, resistance to corrosion; counteracts tin |
| Tin (Sn) | ~25-27% | Enables amalgamation (reacts readily with Hg); reduces hardness/strength |
| Copper (Cu) | ~6% (low-Cu) / 13-30% (high-Cu) | Strength, hardness; eliminates γ2 phase in high-Cu alloys |
| Zinc (Zn) | 0-2% | Scavenger (prevents oxidation during manufacturing) |
| Mercury (Hg) | ~43-55% (by weight of mix) | Liquid metal; provides plasticity and initiates setting reaction |
Phases in Amalgam (VERY IMPORTANT for BDS exams)
Greek Phase Notation
| Phase | Formula | Significance |
|---|---|---|
| γ (Gamma) | Ag₃Sn | Unreacted alloy particles; hardest, strongest phase |
| γ₁ (Gamma-1) | Ag₂Hg₃ | Matrix; 2nd strongest; makes up ~60% of set amalgam |
| γ₂ (Gamma-2) | Sn₇₋₈Hg | WEAKEST phase; most corrosion-prone; responsible for marginal failure ("ditching") |
| ε (Epsilon) | Cu₃Sn | In high-Cu alloys |
| η (Eta) | Cu₆Sn₅ | Forms in high-Cu alloys; eliminates γ2 |
Setting Reaction
Low-Copper (Conventional) Amalgam
γ (Ag₃Sn) + Hg → γ (Ag₃Sn) + γ₁ (Ag₂Hg₃) + γ₂ (Sn₇₋₈Hg)
- Hg dissolves Ag and Sn from the alloy surface
- Intermetallic compounds (γ₁ and γ₂) precipitate out
- γ₂ remains in the set amalgam → weakness and corrosion
High-Copper Amalgam (Admixed)
γ + Cu-Ag eutectic + Hg → γ + γ₁ + γ₂ → γ₁ reacts with γ₂ → η (Cu₆Sn₅) + γ₁
- After initial γ₂ formation, the copper-silver eutectic reacts with γ₂
- Cu preferentially reacts with Sn → forms Cu₆Sn₅ (eta phase)
- γ₂ is consumed/eliminated → superior properties
High-Copper Single Composition (Unicomposition)
γ (Ag₃Sn) + ε (Cu₃Sn) + Hg → γ + γ₁ (Ag₂Hg₃) + η (Cu₆Sn₅)
- No γ₂ formed at all
- Highest strength, lowest creep
Why does eliminating γ₂ matter?
- γ₂ is the weakest and most corrosion-prone phase
- It is responsible for marginal ditching (gap formation at cavity margins over time)
- High-Cu alloys have better creep resistance, strength, and longevity
Properties of Set Amalgam
Mechanical Properties
- Compressive strength - Highest of all properties; ~310-520 MPa (high-Cu > low-Cu)
- Tensile strength - Low (~60 MPa); amalgam is brittle under tension
- Shear/torsion strength - Low; do not carve too aggressively
- Requires bulk of material at margins (never feather edges)
Dimensional Change
- Initially slight contraction (as Hg reacts with alloy surface)
- Then slight expansion (as γ₁ crystals grow)
- Net change should be minimal (-0.15% to +0.20% per ADA standard)
- Excessive contraction → marginal gap → microleakage → secondary caries
- Excessive expansion → post-operative pain, extrusion, tooth fracture
Creep
- Slow plastic deformation under sustained load
- Low-Cu alloys: creep up to 8% → marginal ditching
- High-Cu alloys: creep 0.09-1.8% → far less ditching
- Formula: Higher γ₂ = higher creep
Corrosion / Tarnish
- Tarnish = surface discoloration (sulfide layer)
- Corrosion = electrochemical degradation; most at γ₂ phase
- High-Cu alloys are more corrosion-resistant (no γ₂)
- Corrosion products can expand and seal marginal gaps (self-sealing) - a debated advantage of conventional alloys
Thermal Properties
- Thermal conductivity is high (metal) → needs liner/base under deep cavities
- Coefficient of thermal expansion higher than tooth structure → marginal stresses
Manipulation of Amalgam (Clinical Steps)
1. Proportioning
- Eames Technique (1:1) - Mercury:Alloy ratio of 1:1 by weight (less mercury = better properties)
- Older techniques used higher Hg ratios (8:5)
- Pre-capsulated systems are most common now (correct ratio pre-set)
2. Trituration (Mixing)
- Mechanical mixing in an amalgamator/triturator (capsule spun at high speed)
- Optimal mix: homogeneous, cohesive, slightly warm, not sticky - called "Zipper test" / "snap test"
- Over-trituration → too much heat, rapid set, reduced working time, excess expansion, reduced strength
- Under-trituration → dry, crumbly, granular mix → weaker, more porous, increased corrosion
3. Mulling
- Kneading the amalgam mass in chamois leather or plastic bag after trituration
- Produces smoother, more homogeneous mix
4. Condensation
- Packing amalgam into prepared cavity in small increments
- Use progressively larger condensers
- Pressure drives out excess mercury → lower final Hg:alloy ratio → stronger restoration
- Spherical alloys require less condensation pressure than lathe-cut
- No amalgam should be placed >3 minutes after start of mixing
- Condensing a partly-set amalgam → poor adaptation, weak margins
5. Pre-carve Burnishing
- Using large burnisher for ~15 seconds
- Light force, from center outward to margins
- Reduces surface voids, brings excess Hg to surface for removal during carving
6. Carving
- Within the working time (before set)
- Carve occlusal anatomy, define margins
- Remove excess amalgam
- Do not create thin fins at margins (no feather edges) - they fracture
7. Post-carve Burnishing (Polishing)
- Done 24 hours later (after full set)
- Smooths surface, reduces tarnish and plaque adhesion
- Use slow speed with light, intermittent pressure
- Avoid heat generation (can volatilize mercury)
Indications and Contraindications
Indications
- Class I and II (posterior) restorations that can be well-isolated
- Class VI restorations (cusp tips)
- Large multi-surface restorations (when composite bonding is questionable)
- Patients with high caries risk (moisture control difficult)
- Core build-ups under crowns
- Patients where composite placement technique cannot be adequately performed
Contraindications
- Allergy to mercury, silver, copper, tin, or zinc
- Anterior (visible) areas - aesthetics
- Inability to isolate (relative - amalgam is more forgiving than composite)
- Pregnant women - avoid new placements (precautionary)
- Patients with severe renal disease
- Small Class III/IV restorations (use composite)
- Children < 6 years - FDA advises avoiding in deciduous teeth
Advantages vs. Disadvantages
| Advantages | Disadvantages |
|---|---|
| Durable, long-lasting (10-15+ years) | Unaesthetic (silver-gray color) |
| Easy and fast to place | Contains mercury (health/environmental concerns) |
| Tolerates moisture | Requires retentive cavity preparation (no adhesive bond) |
| Self-sealing corrosion products | Thermal conductivity → sensitivity |
| Inexpensive | Can cause galvanic pain near dissimilar metals |
| Antibacterial (reduces secondary caries) | Marginal ditching with low-Cu alloys |
| Repairable | Environmental disposal issues |
| Works in high-stress posterior areas | Black/gray marginal staining over time |
Cavity Design for Amalgam
Because amalgam has no adhesive bond to tooth structure, cavity preparation must rely on mechanical retention:
- Retention form - parallel or slightly convergent walls (dovetail, undercuts)
- Resistance form - flat pulpal floor perpendicular to occlusal forces
- Minimum depth - 1.5-2.0 mm (minimum bulk for strength)
- Cavosurface angle - 90° butt joint margin (not beveled - thin amalgam at bevel fractures)
- No feather edges
Mercury Safety Precautions (Important for Clinical Practice)
- Use pre-capsulated alloys (avoid open mercury bottles)
- Work in well-ventilated areas
- Wear gloves, mask, eye protection
- Use high-volume evacuation during placement and removal
- Never heat amalgam (increases mercury vapor)
- Store scrap amalgam in sealed containers with water or fixative
- Handle old amalgam removal carefully (rubber dam, water spray, evacuation)
- Amalgam separators required in dental unit wastewater
Bonded Amalgam
- Amalgam can be bonded to tooth using dentin bonding agents
- Benefits: reduced microleakage, reinforces weakened tooth structure, reduces post-op sensitivity
- Not universally adopted but useful in large restorations and cusp replacements
Comparison: Low-Copper vs. High-Copper Amalgam
| Property | Low-Copper | High-Copper |
|---|---|---|
| γ₂ phase | Present | Absent/minimal |
| Compressive strength | Lower | Higher |
| Creep | High (up to 8%) | Low (0.09-1.8%) |
| Marginal ditching | Common | Rare |
| Corrosion | High | Low |
| Early strength | Slow | Fast (full strength in ~1 hr) |
| Clinical longevity | Shorter | Longer |
Exam Memory Tips
- γ₂ = BAD (weak, corrodes, causes ditching) → High-Cu alloys eliminate it
- Gamma phases: γ = alloy particle, γ₁ = matrix (good), γ₂ = weak link (bad)
- Eames technique = 1:1 Hg:Alloy ratio
- Creep = sustained deformation under load → worst in low-Cu
- Zinc in amalgam = scavenger; moisture contamination → delayed expansion (can be >24 hrs later)
- ADA standard: Creep max 1.0%, Dimensional change -0.15 to +0.20%, Compressive strength min 80 MPa (1 hr), 300 MPa (24 hr)
- Never condense amalgam after 3 minutes from start of mix
Primary BDS References for further reading:
- Phillips' Science of Dental Materials (Anusavice, Shen & Rawls) - Chapter on Amalgam
- Craig's Restorative Dental Materials (Sakaguchi & Powers)
- Dental Materials: Properties and Manipulation (Craig & Ward)
- Pocket Dentistry - Dental Amalgam (free online)
This is a shared conversation. Sign in to Orris to start your own chat.