A patient with known case ,of seizures has fever with guiddines, she has severe anemia a nd also tell about, MCV and mch and mchc and menterz in simple , how to approach her
Patient with Seizures + Fever + Severe Anemia - Clinical Approach
1. Red Cell Indices - Explained Simply
| Index | What it measures | Normal range | Simple meaning |
|---|---|---|---|
| MCV (Mean Corpuscular Volume) | Average SIZE of one RBC | 80-96 fL | Is the cell big, small, or normal? |
| MCH (Mean Corpuscular Hemoglobin) | Average AMOUNT of Hb per cell | 27-33 pg | How much Hb is packed in one cell? |
| MCHC (Mean Corpuscular Hb Concentration) | Average CONCENTRATION of Hb per volume of packed cells | 33-36 g/dL | How concentrated is the Hb in the cell? |
- MCH = Hb ÷ RBC count
- MCHC = (Hb ÷ Hct) × 100
- MCV × RBC = Hct
- MCV = cell size (think: Volume = size)
- MCH = total Hb per cell (like total paint in a bucket)
- MCHC = how densely filled the cell is (like paint concentration)
- MCHC only goes HIGH in spherocytosis (rarely >38 g/dL). In most anemias, it is normal or low.
2. The Mentzer Index
| Result | Interpretation |
|---|---|
| >13 | Suggests Iron Deficiency Anemia |
| <13 | Suggests Thalassemia trait |
- (Source: Harriet Lane Handbook, 23rd ed.)
3. Using MCV to Classify the Anemia - Step 1
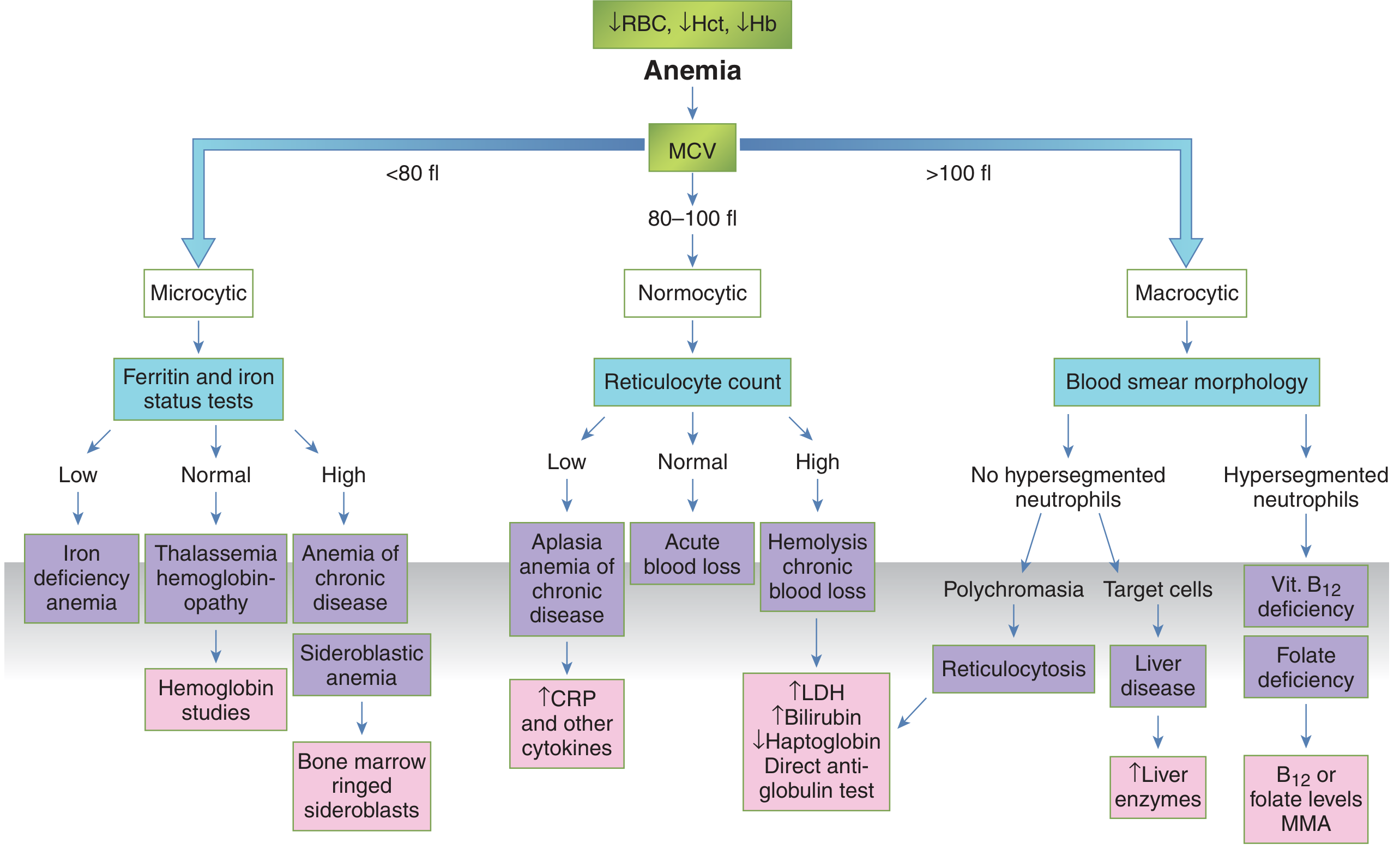
| MCV | Type | Common causes |
|---|---|---|
| <80 fL | Microcytic | Iron deficiency, thalassemia, anemia of chronic disease, lead poisoning, sideroblastic |
| 80-100 fL | Normocytic | Acute blood loss, aplastic anemia, hemolysis, CKD, anemia of chronic disease |
| >100 fL | Macrocytic | B12 deficiency, folate deficiency, liver disease, hypothyroidism |
4. Special Consideration: This Patient is on Anti-Epileptic Drugs (AEDs)
| AED | Mechanism | Type of anemia |
|---|---|---|
| Phenytoin, Phenobarbital, Carbamazepine | Interfere with folate absorption/metabolism | Macrocytic (megaloblastic) anemia |
| Valproic acid | Bone marrow suppression | Normocytic or thrombocytopenia |
| Levetiracetam | Less commonly causes anemia |
5. Fever in This Patient - What to Think About
- Fever can be a sign of hemolytic crisis (malaria, G6PD deficiency, autoimmune hemolytic anemia, sickle cell crisis)
- Check: LDH (high), bilirubin (indirect high), haptoglobin (low), reticulocyte count (high), peripheral smear, direct antiglobulin test (DAT/Coombs)
- Malaria causes severe anemia + fever - check thick/thin smear, RDT
- Sepsis causes normocytic anemia (anemia of inflammation) + suppressed erythropoiesis
- Typhoid, TB, endocarditis all cause anemia
- Drug-induced fever (especially carbamazepine, phenytoin, lamotrigine) - can cause aplastic anemia or agranulocytosis simultaneously
6. Complete Clinical Approach - Step by Step
History
- Duration and type of seizures, which AED she is on and for how long
- Dietary history (vegetarian? alcohol? malnutrition?)
- Blood loss history (menorrhagia, GI symptoms)
- Symptoms of hemolysis (dark urine, jaundice)
- Family history (thalassemia, G6PD)
- Travel history (malaria-endemic area?)
- Source of fever - UTI, pneumonia, any localizing symptoms
Examination
- Pallor (conjunctival, palmar)
- Jaundice (suggests hemolysis)
- Splenomegaly (hemolysis, malaria, thalassemia)
- Signs of heart failure from severe anemia (tachycardia, raised JVP, gallop)
- Signs of B12 deficiency (tongue changes, neuropathy - peripheral or subacute combined degeneration of spinal cord)
- Lymphadenopathy, petechiae (bone marrow failure)
Immediate Investigations (Tier 1)
- CBC with differential - Hb, MCV, MCH, MCHC, RDW, WBC, platelets
- Peripheral blood smear - morphology is gold (target cells, sickle cells, schistocytes, hypersegmented neutrophils, ring forms in malaria)
- Reticulocyte count - high = production is trying (hemolysis/blood loss); low = bone marrow problem
- LFTs, LDH, indirect bilirubin, haptoglobin - hemolysis screen
- Blood culture + malaria smear - source of fever
- Serum ferritin + serum iron + TIBC
- Serum B12 + RBC folate - especially given AED use
- Direct Antiglobulin Test (DAT/Coombs) - autoimmune hemolytic anemia
- Renal function, urine routine - CKD as cause of normocytic anemia
- CRP/ESR - inflammation
If Microcytic (MCV <80)
- Iron studies + Mentzer index
- If Mentzer <13 and normal iron: do Hb electrophoresis (thalassemia)
- If low ferritin: iron deficiency - find the source of loss
If Macrocytic (MCV >100)
- B12 and folate levels
- Check for hypersegmented neutrophils on smear
- Stop or supplement for the offending AED
Severity Assessment for Transfusion
- Hb <7 g/dL (or <8 g/dL with cardiac symptoms): transfuse packed RBCs
- In severe malaria with Hb <4 g/dL: urgent transfusion regardless
- Always stabilize first - oxygen, IV access, cardiac monitoring
Summary Flowchart Logic
Anemia confirmed (low Hb)
↓
Look at MCV
- <80 (Microcytic) → Iron studies → Mentzer index → Hb electrophoresis if needed
- 80-100 (Normocytic) → Reticulocyte count → hemolysis screen / BM workup
- >100 (Macrocytic) → B12 / folate levels → smear for hypersegmented neutrophils
↓
Add fever workup: malaria smear, blood culture, CBC for pancytopenia (aplastic from AED?)
↓
AED review: phenytoin/carbamazepine/phenobarbital → check folate; valproate → check BM suppression
↓
Stabilize: transfuse if Hb <7, treat infection, supplement deficiency
Find recent guidelines on AED-induced hematologic complications
antiepileptic drugs hematologic complications
antiseizure medication anemia blood dyscrasia monitoring
PMID: 34382515
valproate carbamazepine phenytoin thrombocytopenia aplastic anemia folate
antiepileptic drugs folate deficiency macrocytic anemia monitoring
valproic acid thrombocytopenia mechanism management
antiepileptic drugs CBC monitoring blood count recommendations
antiepileptic drugs adverse hematological effects review
AED antiepileptic drug hematologic complications guidelines monitoring 2023 2024 2025
epilepsy treatment hematotoxicity leukopenia neutropenia review
valproate carbamazepine phenytoin blood dyscrasias hematologic monitoring clinical guidelines 2024
https://www.epilepsy.va.gov/EPILEPSY/Library/PDFs/ECoE_Antis…
levetiracetam lamotrigine oxcarbazepine hematologic side effects blood count
Recent Guidelines on AED-Induced Hematologic Complications
- VA ECoE Antiseizure Medication Desk Guide, July 2025 - full guide PDF
- American Epilepsy Society (AES) Summary of ASMs, 4th edition, April 2024 - AES PDF
- PubMed Systematic Review (PMID: 34382515) - valproate hematotoxicity in children
Drug-by-Drug Hematologic Profile
1. Carbamazepine (CBZ / Tegretol)
| Effect | Frequency | Notes |
|---|---|---|
| Transient leukopenia | ~10% of patients | Usually first 4 months; resolves spontaneously |
| Persistent leukopenia | ~2% | Requires drug withdrawal |
| Aplastic anemia | ~1 in 200,000 | Rare but life-threatening; FDA black box warning |
| Agranulocytosis | ~1 in 125,000 | No clear correlation with the benign transient leukopenia |
| Thrombocytopenia | Rare | Drug-dependent autoantibodies + direct marrow toxicity |
| Eosinophilia/leukocytosis | Rare | Hypersensitivity-mediated |
2. Valproic Acid / Sodium Valproate (VPA)
| Effect | Notes |
|---|---|
| Thrombocytopenia | Most common; dose-dependent; autoantibodies + direct marrow suppression |
| Decreased platelet aggregation | Affects coagulation even with normal platelet count |
| Neutropenia | Documented especially in children |
| Bone marrow depression | Reversible in most cases within 2 weeks of dose reduction or switch |
| Hemorrhage | Secondary to above |
3. Phenytoin (PHT)
| Effect | Notes |
|---|---|
| Megaloblastic / macrocytic anemia | Via folate depletion (inhibits intestinal absorption + alters folate metabolism) |
| Leukopenia, agranulocytosis | Rare |
| Drug-induced hypersensitivity syndrome | Can include eosinophilia + lymphadenopathy (see case review PMID: 39331866) |
| Aplastic anemia | Very rare |
4. Phenobarbital / Primidone
| Effect | Notes |
|---|---|
| Megaloblastic anemia | Same mechanism as phenytoin - folate depletion |
| Rare aplasia | Case reports only |
5. Lamotrigine (LTG)
| Effect | Notes |
|---|---|
| Blood dyscrasias (neutropenia, thrombocytopenia, pancytopenia) | Uncommon; higher risk in combination with VPA |
| Hemophagocytic lymphohistiocytosis (HLH) | Rare but life-threatening; presents with fever + cytopenias |
6. Oxcarbazepine / Eslicarbazepine (OXC / ESL)
| Effect | Notes |
|---|---|
| Bone marrow suppression (aplastic anemia, leukopenia, neutropenia, thrombocytopenia) | Less common than carbamazepine |
| Cross-sensitivity to carbamazepine | Important - if patient had hematologic reaction to CBZ, do not use OXC/ESL |
7. Felbamate (FBM)
| Effect | Notes |
|---|---|
| Aplastic anemia | High risk - estimated 1 in 3,000-5,000 (much higher than CBZ) |
| Hepatic failure | Also high risk |
8. Ethosuximide (ESM)
| Effect | Notes |
|---|---|
| Leukopenia, agranulocytosis, pancytopenia, aplastic anemia | Rare |
| Eosinophilia | Hypersensitivity |
| SLE-like syndrome | With cytopenias |
9. Levetiracetam (LEV)
Consolidated Monitoring Protocol (Current Guidelines Summary)
| Drug | Baseline CBC | Periodic CBC | Folate/B12 | Notes |
|---|---|---|---|---|
| Carbamazepine | Yes | Yes | No | Stop if severe progressive leukopenia or fever with sore throat |
| Valproate | Yes | Yes (+ INR, PTT) | No | Also check ammonia; thrombocytopenia is dose-dependent |
| Phenytoin | Periodically | Periodically | Yes | Supplement folate; monitor B12 |
| Phenobarbital | Periodically | Periodically | Yes | Same as phenytoin |
| Lamotrigine | Periodic | Periodic | Caution | Weak DHFR inhibitor |
| Felbamate | Mandatory | Frequently | No | High aplasia risk; contraindicated with hx of dyscrasia |
| Oxcarbazepine | Yes | Yes | No | Cross-sensitive with CBZ |
| Ethosuximide | Periodic | Periodic | No | Especially if signs of infection |
When to Stop the Drug - Red Flags
- Severe, progressive, or symptomatic leukopenia (especially if WBC <3,000 or neutrophils <1,500 with fever/sore throat) - stop drug
- Thrombocytopenia with bleeding - reduce dose or stop (especially valproate)
- Aplastic anemia / agranulocytosis confirmed - permanently stop the offending AED; do NOT rechallenge
- DRESS syndrome (fever + eosinophilia + organ involvement) - stop immediately, treat with steroids
Special Points for Your Patient
- Identify the exact AED she is on - the type of anemia will differ dramatically
- If on phenytoin or phenobarbital - check folate and B12 immediately; supplement folic acid 1-5 mg/day
- If on valproate - check platelet count + coagulation (PTT/INR) urgently; thrombocytopenia may explain bleeding tendency alongside fever
- If on carbamazepine - fever + leukopenia raises concern for agranulocytosis; urgent CBC and differential; consider stopping if WBC is critically low
- Rule out drug-induced fever (DRESS, hypersensitivity syndrome) from carbamazepine, phenytoin, or lamotrigine - these present with fever + eosinophilia + cytopenias together
Tell me approach to acute febrile illness u der evaly,how to approach im simple
Approach to Acute Febrile Illness - Simple & Clear
STEP 1 - Define the Fever First
- Temperature varies throughout the day - lowest in early morning, highest at 4-6 PM
- Always confirm with a proper thermometer (oral, rectal, or tympanic)
- Rectal is most accurate, oral is standard
STEP 2 - Ask Yourself "Is This an Emergency?"
| Red Flag Sign | Think of... | Action |
|---|---|---|
| Fever + non-blanching petechial/purpuric rash | Meningococcemia | Emergency - IV antibiotics NOW |
| Fever + neck stiffness + headache | Meningitis | LP urgently, start antibiotics |
| Fever + altered consciousness | Encephalitis, sepsis, cerebral malaria | Urgent |
| Fever + hypotension/shock | Septic shock | IV fluids + antibiotics immediately |
| Fever + severe thrombocytopenia + bleeding | Dengue hemorrhagic fever, DIC | Urgent |
| Fever + very high HR + rigors | Bacteremia, malaria | Blood cultures, malaria smear |
Rule: If any red flag is present - stabilize first, investigate second.
STEP 3 - Take a Focused History (MNEMONIC: "POET AVID")
P - Pattern of fever
- Continuous (stays high, doesn't come down) - Typhoid, pneumonia
- Remittent (goes up and down but never to normal) - Most bacterial infections
- Intermittent (returns to normal between spikes) - Malaria, abscess, TB
- Relapsing (fever-free days between episodes) - Malaria (tertian/quartan), Brucella, Borrelia
O - Onset & Duration
- Sudden onset with rigors → Malaria, bacteremia, pyelonephritis
- Gradual onset, 1st week building up → Typhoid, TB
- Duration <7 days = acute febrile illness; >3 weeks = fever of unknown origin (FUO)
E - Exposure & Epidemiology
- Travel history - where? malaria zone? dengue area? Middle East (MERS)?
- Animal contact - cattle (Brucella), rats (Leptospira, rat-bite fever), birds (Psittacosis)
- Water/food - untreated water (typhoid, leptospira), raw meat
- Insects - mosquitoes (malaria, dengue, chikungunya), ticks (Rickettsia, Lyme), sandfly (Leishmaniasis)
- Sexual history - HIV, gonorrhea
- Injection drug use - endocarditis, HIV, hepatitis
T - Tender areas / Localizing symptoms
- Headache → meningitis, malaria, typhoid, dengue
- Sore throat → pharyngitis, EBV (mono), diphtheria
- Cough → pneumonia, TB, influenza
- Diarrhea → enteric infections (Salmonella, Shigella, Campylobacter)
- Dysuria → UTI/pyelonephritis
- Abdominal pain → hepatitis, typhoid, amoebic abscess
- Joint pain → Dengue ("breakbone fever"), chikungunya, rheumatic fever
A - Allergies & past history
- Known illnesses: diabetes, HIV, immunosuppression → atypical organisms more likely
- Past similar episodes → malaria, Brucella
V - Vaccinations
- Not vaccinated? → consider typhoid, hepatitis A, meningitis
I - Immunization & drug history
- On steroids or immunosuppressants? - fungal, opportunistic infections
- On AEDs? → drug fever possible (especially carbamazepine, phenytoin, lamotrigine)
D - Drug fever / non-infectious causes
- Remember: fever can be non-infectious - malignancy, autoimmune (SLE, Still's disease), DVT, drug reaction, thyroid storm
STEP 4 - Examination - Head to Toe
| System | What to look for | Suggests |
|---|---|---|
| General | Toxic vs non-toxic appearance | Severity |
| Vitals | Pulse-temp dissociation | Typhoid, dengue, legionella |
| Skin | Rash type and distribution | Many (see below) |
| Eyes | Jaundice, conjunctival pallor, suffusion (red eyes) | Leptospira, malaria, hepatitis |
| Mouth | Pharyngitis, oral ulcers, strawberry tongue | Strep, EBV, Kawasaki |
| Lymph nodes | Generalized vs regional adenopathy | EBV, HIV, TB, lymphoma |
| Chest | Crepitations, bronchial breathing | Pneumonia |
| Abdomen | Hepatomegaly, splenomegaly, tenderness | Malaria, typhoid, EBV, TB, dengue |
| Neuro | Meningismus, altered GCS, focal deficits | Meningitis, encephalitis, cerebral malaria |
| Joints | Swelling, warmth | Septic arthritis, rheumatic fever, dengue |
Rash Guide (very useful at the bedside):
| Rash type | Think of... |
|---|---|
| Maculopapular | Dengue, viral exanthem, drug reaction, EBV, HIV seroconversion |
| Petechiae / purpura (non-blanching) | Meningococcemia (emergency!), DIC, dengue |
| Rose spots on abdomen | Typhoid |
| Eschar (black scab) | Scrub typhus (Rickettsia) |
| Vesicular | Chickenpox, herpes zoster, herpes simplex |
| Target lesion | Lyme disease (erythema migrans) |
| Diffuse erythema + peeling | Toxic shock syndrome, scarlet fever |
STEP 5 - Investigations - Tiered Approach
Tier 1 - Do in ALL fever patients (the "baseline fever workup"):
- CBC with differential - leukocytosis (bacterial), leukopenia (typhoid, dengue, viral), atypical lymphocytes (EBV), thrombocytopenia (dengue, malaria)
- Peripheral blood smear - malaria parasites, morphology
- ESR / CRP - confirms inflammation; elevated in bacterial > viral
- Blood cultures x 2 - before starting antibiotics
- Urine routine and culture - always (UTI is common and easy to miss)
- Malaria rapid test (RDT) + thick/thin smear - in any febrile patient in endemic area or with travel history
- LFTs - hepatitis, typhoid, dengue
- Renal function - leptospira, severe malaria, sepsis
Tier 2 - Add based on clinical clues:
| Suspicion | Test |
|---|---|
| Dengue | NS1 antigen (day 1-5), IgM/IgG serology |
| Typhoid | Widal test (low specificity), blood culture (gold standard), Typhidot |
| TB | CXR, Mantoux, sputum AFB, GeneXpert |
| Malaria | Thick smear + RDT (repeat if negative and high suspicion) |
| Leptospirosis | IgM ELISA (after day 7), PCR early |
| Scrub typhus | Weil-Felix test, IgM serology |
| Meningitis | LP - CSF analysis urgently |
| Endocarditis | Serial blood cultures, ECHO |
| EBV/CMV | Monospot, IgM serology |
| HIV seroconversion | HIV Ag/Ab combo |
| Drug fever | Clinical diagnosis - stop suspected drug, see if fever resolves in 48-72h |
Tier 3 - Severe/Persistent cases:
- CT chest/abdomen - occult abscess, lymphoma
- Bone marrow biopsy - pancytopenia, suspected leishmania or TB
- Procalcitonin - distinguishes bacterial vs viral (high in bacterial sepsis)
- ANA, complement, ANCA - autoimmune causes
STEP 6 - Management Framework
FEBRILE PATIENT
↓
Is patient STABLE? → No → Resuscitate (ABC, IV access, fluids, O2)
↓ Yes
Identify FOCUS → Treat specifically
↓
No focus found?
↓
Empirical treatment based on:
- Severity (mild = oral; severe = IV)
- Likely organism (community vs hospital vs travel)
- Local antimicrobial sensitivity patterns
↓
ALWAYS: Blood cultures BEFORE first antibiotic dose
ALWAYS: Antipyretics (paracetamol 500mg-1g) for comfort
ALWAYS: Adequate hydration (oral or IV)
ALWAYS: Monitor vitals every 4-6 hours
When to admit vs send home:
| Admit | Can manage outpatient |
|---|---|
| Hb <7 or severe anemia | Mild self-limited viral fever |
| Thrombocytopenia <50,000 | Low-grade fever, no red flags |
| Altered sensorium | Tolerating oral fluids |
| Hypotension/shock | No serious underlying disease |
| Unable to take oral meds | Reliable follow-up possible |
| Suspected meningitis/sepsis | Good home environment |
| Immunocompromised | — |
Quick Memory Aid - "FEVER" Mnemonic
| Letter | Meaning |
|---|---|
| F | Find the focus (history + exam) |
| E | Emergency signs? - treat first if yes |
| V | Vitals - pulse, BP, RR, SpO2, temperature |
| E | Essential tests - CBC, smear, cultures, CRP |
| R | Review travel, exposures, drugs, vaccinations |