How to arrive to a pathological and suspicious and normal ctg
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
CTG classification normal suspicious pathological FIGO 2015 criteria fetal heart rate
Finding Sources
Reading Web Page
CTG normal suspicious pathological classification criteria table
Finding Sources
Searching Images
CTG cardiotocography classification normal suspicious pathological fetal heart rate
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive guide to CTG (cardiotocography) classification using the FIGO 2015 guidelines — the current international standard that divides tracings into Normal, Suspicious, and Pathological.
CTG Classification: Normal, Suspicious, and Pathological
Step 1 — Evaluate the Four Core CTG Features
Before classifying, assess each of these independently:
| Feature | What to measure |
|---|---|
| Baseline FHR | Mean FHR over a 10-min window (excluding accelerations/decelerations) |
| Variability | Amplitude of beat-to-beat fluctuation around the baseline |
| Accelerations | Transient rises in FHR ≥15 bpm lasting ≥15 sec |
| Decelerations | Transient falls in FHR — classify by timing and shape |
Step 2 — Define Each Feature (Normal Ranges)
Baseline FHR
- Normal: 110–160 bpm
- Tachycardia: >160 bpm
- Bradycardia: <110 bpm (100–110 bpm = intermediate/suspicious zone)
Baseline Variability
- Normal: 5–25 bpm amplitude
- Reduced: <5 bpm
- Increased (saltatory): >25 bpm
- Sinusoidal: smooth, undulating sine-wave pattern ≥30 min — always pathological
Accelerations
- Presence = reassuring (fetus without hypoxia/acidosis)
- Absence during labour is not itself pathological, but is of uncertain significance
Decelerations — Types
| Type | Onset | Cause | Significance |
|---|---|---|---|
| Early | Gradual, mirrors contraction | Head compression | Benign |
| Variable | Abrupt (<30 sec to nadir) | Cord compression | Context-dependent |
| Late | Gradual, begins after contraction peak; nadir >30 sec after onset | Uteroplacental insufficiency → fetal hypoxemia | Most concerning |
| Prolonged | Single deceleration lasting ≥2 min | Various | Duration determines severity |
Step 3 — Classify the Tracing (FIGO 2015)
| Feature | Normal | Suspicious | Pathological |
|---|---|---|---|
| Baseline | 110–160 bpm | Lacks ≥1 normal feature, but no pathological feature | <100 bpm |
| Variability | 5–25 bpm | Reduced <5 bpm for >50 min, or increased >25 bpm for >30 min | Sinusoidal pattern ≥30 min |
| Decelerations | No repetitive decelerations | Repetitive decelerations present (but don't meet pathological criteria) | Repetitive late or prolonged decelerations for >30 min (or >20 min if variability is also reduced), OR a single prolonged deceleration >5 min |
| Clinical meaning | No hypoxia/acidosis | Low probability of hypoxia/acidosis | High probability of hypoxia/acidosis |
"Repetitive" = occurring with ≥50% of contractions over a 20–30 min window.
Step 4 — Management by Category
| Classification | Action |
|---|---|
| Normal | No intervention needed for fetal oxygenation; continue monitoring |
| Suspicious | Correct reversible causes (maternal position, hydration, oxytocin reduction), close monitoring, consider additional fetal assessment (e.g. scalp pH/lactate, fetal pulse oximetry) |
| Pathological | Immediate action: correct reversible causes + additional fetal assessment OR expedite delivery. In acute situations (cord prolapse, uterine rupture, placental abruption) → immediate delivery |
ACOG Three-Tier System (used in the USA)
The USA uses a parallel Category I/II/III system:
| Category | Equivalent | Criteria |
|---|---|---|
| Category I (Normal) | Normal | Baseline 110–160 bpm, moderate variability, ± accelerations, no late/variable decelerations |
| Category II (Indeterminate) | Suspicious | Everything not in I or III — requires continued observation |
| Category III (Abnormal) | Pathological | Absent variability WITH: recurrent late decelerations, recurrent variable decelerations, bradycardia, OR sinusoidal pattern |
(Barash, Clinical Anesthesia 9e)
Visual Examples
Normal vs. Suspicious CTG:
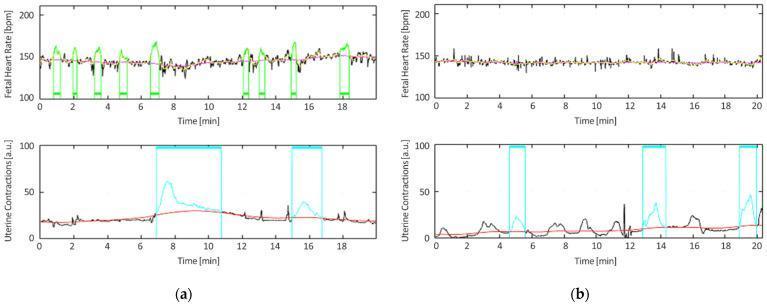
Left (a): Normal — high beat-to-beat variability with multiple accelerations. Right (b): Suspicious — flattened trace with reduced variability.
Pathological vs. Normal comparison:
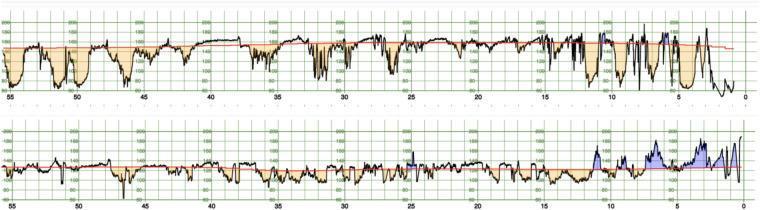
Top: Pathological trace (pH < 7.05) — frequent, deep decelerations, minimal accelerations. Bottom: Normal — reactive pattern with accelerations.
Pathological — deep variable decelerations:
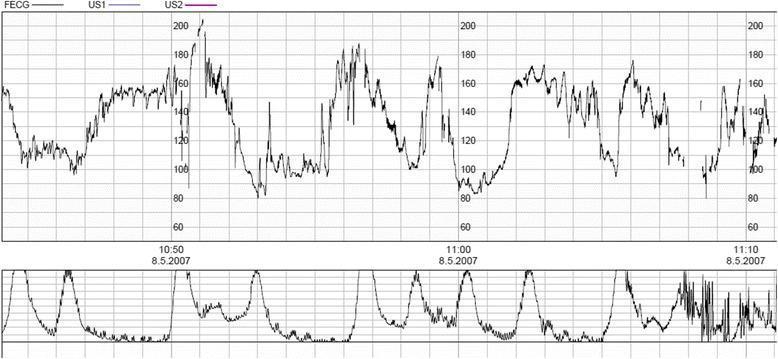
Deep, prolonged variable decelerations (>60 bpm depth, >60 sec duration) with frequent contractions — pathological by FIGO criteria.
Key Pitfalls
- Absent accelerations alone do not make a trace suspicious during labour — this is of uncertain significance
- Reduced variability is only suspicious if present for >50 minutes continuously; short periods may reflect fetal sleep cycle (~20 min)
- A single prolonged deceleration >5 min = pathological regardless of other features
- CTG has significant inter-observer variability — the suspicious/pathological boundary has the lowest agreement among clinicians
- A normal CTG effectively excludes current hypoxia/acidosis; however, suspicious and pathological traces have a high false-positive rate for metabolic acidosis
Sources: FIGO 2015 Consensus Guidelines on Intrapartum Fetal Monitoring; Barash, Cullen & Stoelting's Clinical Anesthesia 9e (Table 41-8); NICE CTG classification framework.
This is a shared conversation. Sign in to Orris to start your own chat.