Ectopic heartbeats
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ectopic beats" OR "premature contractions"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
I now have all the material needed for a thorough, image-rich answer.
Ectopic Heartbeats
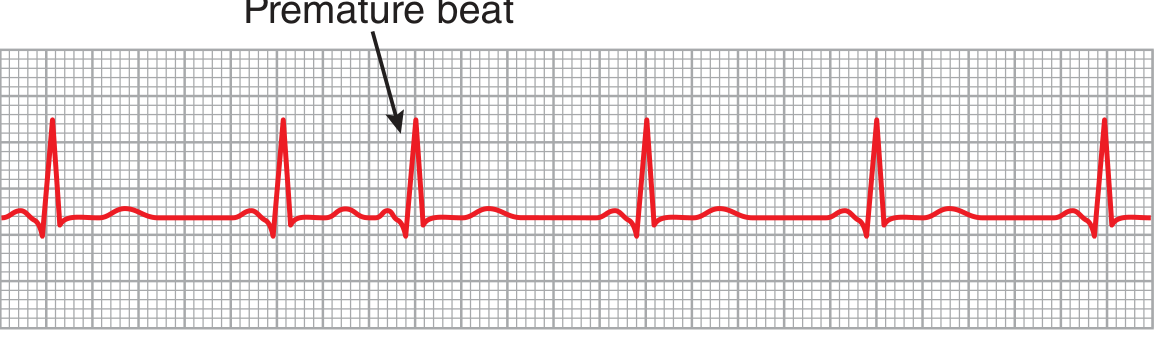
An ectopic beat (also called an extrasystole, premature beat, or premature contraction) is a cardiac impulse that originates from any site in the heart other than the sinoatrial (SA) node. It fires before the next expected normal beat and transiently interrupts the cardiac rhythm.
Mechanisms of Ectopic Beat Formation
There are two main electrophysiological mechanisms:
1. Abnormal Automaticity (Enhanced Ectopic Focus)
Normally, myocardial cells outside the SA node do not discharge spontaneously - the SA node suppresses them by firing faster (a concept called overdrive suppression). When the SA node slows or an ectopic site becomes abnormally irritable (increased automaticity), that focus can fire and produce a premature beat. If the ectopic focus discharges once, the result is a single premature beat. If it discharges repetitively at a rate faster than the SA node, it produces a sustained tachyarrhythmia (atrial tachycardia, junctional tachycardia, or ventricular tachycardia). - Ganong's Review of Medical Physiology, p. 530
2. Reentry
A more common cause of repetitive ectopic firing. A transient conduction block in one limb of a circuit allows an impulse to travel down the unblocked path, then circle back through the previously blocked path (when it recovers), establishing a continuous circus movement. - Ganong's Review of Medical Physiology, p. 530
Causes of Ectopic Foci
-
Local areas of myocardial ischemia
-
Small calcified plaques pressing on adjacent cardiac muscle
-
Toxic irritation of the AV node, Purkinje system, or myocardium: infection, drugs, nicotine, caffeine, digitalis toxicity
-
Mechanical irritation (e.g., catheter tip touching the endocardium during cardiac catheterization)
-
Electrolyte imbalances (hypokalemia, hypomagnesemia)
-
Hypoxia, sympathetic excess, thyrotoxicosis
-
Guyton & Hall Textbook of Medical Physiology, p. 168
Classification by Site of Origin
| Type | Origin | Also Called |
|---|---|---|
| Atrial | Atrial muscle (outside SA node) | PAC, APC (atrial premature complex) |
| Junctional | AV node / AV bundle (His bundle) | AV nodal premature contraction |
| Ventricular | Ventricular myocardium / Purkinje system | PVC (premature ventricular contraction) |
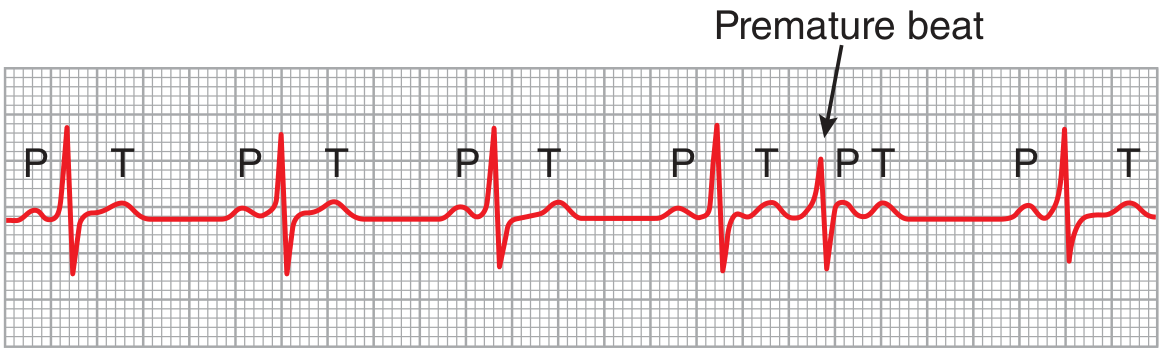
1. Atrial Premature Contractions (PACs)
ECG features:
- Early P wave with an abnormal morphology (different from the sinus P wave)
- P wave is frequently inscribed within the preceding T wave, making morphology unclear
- PR interval may be shortened (if ectopic focus is near the AV node) or prolonged
- QRS is usually narrow (normal) - conducted normally through the bundle of His and ventricles
- Compensatory pause follows - the premature impulse discharged the sinus node early, resetting its timing
A nonconducted (blocked) PAC - where the ectopic atrial impulse arrives when the AV node is still refractory - is one of the most common causes of an unexpected pause on an ECG and can mimic sinus bradycardia, especially in bigeminy.
Clinical significance of PACs:
- In the vast majority, PACs are benign and require only reassurance
- However, Haïssaguerre et al.'s landmark work showed PACs from pulmonary vein sleeves can trigger atrial fibrillation (AF)
- Excess PACs (>30/hour or runs >20 beats) are associated with incident AF, stroke, and death
- Patients with excess PACs and CHADS-VASc ≥ 2 have an annual stroke risk comparable to patients with known AF
- Very frequent PACs (20-40% daily burden) may cause reversible cardiomyopathy
Braunwald's Heart Disease, p. 491
2. Junctional (AV Nodal) Premature Contractions
ECG features:
- P wave is absent or hidden - the impulse travels retrogradely into the atria and forward into the ventricles simultaneously, superimposing the P wave onto the QRS-T complex
- The QRS complex is usually narrow (normal configuration)
- The P wave, if visible, appears just before or just after the QRS and is typically inverted in inferior leads
General significance and causes are similar to PACs.
3. Premature Ventricular Contractions (PVCs)
PVCs are the most clinically significant type of ectopic beat.
ECG features:
- Wide, bizarre QRS complex (usually >120 ms) - the impulse travels through the ventricular myocardium rather than the fast-conducting Purkinje system
- High voltage - in a normal beat, both ventricles depolarize nearly simultaneously so the vectors partially cancel out. In a PVC, one ventricle depolarizes ahead of the other, generating large electrical potentials
- T wave polarity opposite to the QRS - because slow muscle conduction means the first areas to depolarize are also the first to repolarize, creating discordance
- Full compensatory pause - the SA node timing is usually undisturbed; the post-PVC pause brings the next sinus beat back on schedule
Patterns of PVCs:
| Pattern | Definition |
|---|---|
| Bigeminy | Every other beat is a PVC |
| Trigeminy | Every third beat is a PVC |
| Couplet | Two PVCs in a row |
| Triplet | Three PVCs in a row (= non-sustained VT) |
| R-on-T | PVC falls on T wave of preceding beat (dangerous) |
Pulse deficit: Because the ventricle contracts prematurely before adequate filling, stroke volume is reduced or absent. The peripheral pulse may not be felt even though the heart contracted, creating a discrepancy between apical rate and radial pulse rate.
Clinical significance of PVCs:
- Isolated, infrequent PVCs in an otherwise healthy heart are usually benign (nicotine, caffeine, fatigue, emotion)
- PVC burden >20% of beats is associated with cardiac dilation and cardiomyopathy - often reversible with treatment
- PVCs occurring in the vulnerable period (on the T wave, "R-on-T phenomenon") risk triggering ventricular fibrillation
- PVCs in the setting of ischemia, structural heart disease, or after MI carry significantly higher risk
Guyton & Hall, p. 169-170
Symptoms
Most ectopic beats are asymptomatic. When symptoms occur, patients may describe:
- A sense that the heart gave an "extra beat" or "missed a beat"
- Palpitations or fluttering in the chest or throat
- A thudding or pounding sensation (the forceful beat after the pause)
- Occasional brief dizziness or faintness
Braunwald's Heart Disease, p. 491
Diagnosis
- 12-lead ECG - detects ectopic beats occurring at the time of recording
- Ambulatory Holter monitoring (24-48 hours) - quantifies ectopic burden; essential for assessing frequency and patterns
- Event recorder / loop recorder - for infrequent symptoms; allows patient-triggered recording
- Echocardiogram - to assess for underlying structural heart disease and cardiomyopathy (especially if PVC burden is high)
Treatment
PACs: No treatment needed in most cases. If symptomatic:
- Eliminate triggers (caffeine, alcohol, sleep deprivation, stimulants)
- Beta-blocker or non-dihydropyridine calcium channel blocker (verapamil, diltiazem)
- Antiarrhythmic drugs (e.g., flecainide) in refractory cases
- Catheter ablation for high-burden, unifocal, drug-refractory symptomatic PACs
PVCs:
- Address reversible causes (ischemia, electrolyte abnormalities, thyrotoxicosis)
- Beta-blockers - first-line for symptomatic PVCs
- Antiarrhythmics (flecainide, propafenone for structurally normal heart; amiodarone, mexiletine if structural disease)
- Catheter ablation - highly effective, especially for unifocal PVCs; indicated for symptomatic or high-burden PVCs causing cardiomyopathy
Braunwald's Heart Disease, p. 491
Summary Table
| Feature | PAC | AV Junctional | PVC |
|---|---|---|---|
| P wave | Early, abnormal morphology | Hidden in QRS | Absent |
| QRS width | Narrow | Narrow | Wide (>120 ms) |
| Compensatory pause | Incomplete (usually) | Variable | Full (usually) |
| T wave | Normal | Normal | Discordant (opposite QRS) |
| Risk | AF trigger if frequent | Generally benign | VF risk if R-on-T; cardiomyopathy if >20% |
Proximal femur nailing
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive data from Rockwood & Green and Miller's Review. Let me compile the full answer:
Proximal Femur Nailing (Cephalomedullary Nailing)
Proximal femur nailing - also called cephalomedullary (CM) nailing - is the fixation of proximal femoral fractures using an intramedullary nail inserted via the greater trochanter, with a cephalocervical lag screw locking into the femoral head/neck. It combines the mechanical advantage of intramedullary load sharing with rotational control of the head-neck fragment.
Indications
CM nailing is the implant of choice for:
| Fracture Type | Notes |
|---|---|
| Unstable intertrochanteric fractures | Reverse oblique, comminuted, absent lateral wall (<20.5 mm) |
| All intertrochanteric fractures | Valid option; mandatory for unstable patterns |
| Subtrochanteric fractures | Long nail preferred; extends to distal interlocking |
| Basicervical femoral neck fractures | Cephalomedullary construct controls rotation |
| Pathological fractures of proximal femur | |
| Ipsilateral femoral neck + shaft fractures | Reconstruction nail |
For stable intertrochanteric fractures (intact lateral wall >20.5 mm), a Sliding Hip Screw (SHS/DHS) is also acceptable and cheaper - but a CM nail is still a valid choice for all patterns.
- Miller's Review of Orthopaedics 9th Ed, p. 918
- Rockwood and Green's Fractures in Adults 10th Ed
Implant Principles
The CM nail acts as an intramedullary buttress - it resists femoral medialization and provides less fracture collapse than extramedullary devices (SHS). The nail body sits in the medullary canal, and the lag screw slides within the nail barrel, allowing controlled fracture impaction while preventing medialization.
Key design features:
- Proximal entry angle: typically 4-6° valgus (trochanteric entry)
- Anterior bow: nail bow must match the anterior bow of the femur to avoid anterior cortex perforation distally
- Lag screw: single-screw design (e.g., PFNA, Gamma nail, TFN) or dual-screw design (e.g., InterTAN)
- Blade vs. screw: Cephalad blade has more medial migration risk than a cephalad screw
Surgical Setup and Positioning
Table: Fracture table is essential - closed reduction without it is not recommended.
Position: Supine. The injured leg is placed in traction in a traction boot. The uninjured leg is either:
- Flexed and abducted in a lithotomy stirrup (C-arm goes between legs)
- Extended in the "scissor" position (C-arm from opposite side) - preferred when contralateral hip motion is limited
A transparent plastic isolation drape suspended from a rail above the patient is preferred to separate the sterile field from the image intensifier.

Fracture Reduction - The Most Critical Step
The two most important intraoperative steps are: (1) fracture reduction and (2) guidewire placement in the femoral head.
AP view:
- Reduce to anatomical or slight valgus - valgus is associated with the lowest risk of implant cut-out and less limb shortening
- A slight medial cortex gap in valgus is acceptable - it closes rapidly with fracture collapse
- Varus must never be accepted - mechanically unstable, leads to progressive varus collapse and cut-out
Lateral view:
- Femoral head, neck, and trochanteric region must align in a straight line
- Sagittal sag is more common in bariatric patients, high-energy injuries, and comminuted fractures
Reduction aids when closed reduction fails:
- Posterior reduction aid (attached to fracture table - provides upward pressure)
- Vertical crutch/support under the fracture site
- Bone lever or clamp placed percutaneously
- Formal open reduction (rare - mainly for A3/reverse oblique/subtrochanteric)
- Cerclage wires after open reduction in selected cases
Rotation control: Patella should face the ceiling throughout.
Surgical Technique - Step by Step
| Step | Detail |
|---|---|
| 1. Incision | 3-cm incision ~5 cm proximal to the tip of greater trochanter; incise fascia lata; split muscle to the trochanter |
| 2. Entry point guidewire | Insert at tip of greater trochanter - just lateral to medial aspect on AP view; centered or slightly posterior on lateral view |
| 3. Open proximal canal | Core/ream proximal 5 cm with solid channel reamer to size |
| 4. Ream medullary canal | Ream to accommodate nail diameter (if required by nail design) |
| 5. Insert nail | Advance nail under fluoroscopic guidance - confirm alignment AP and lateral |
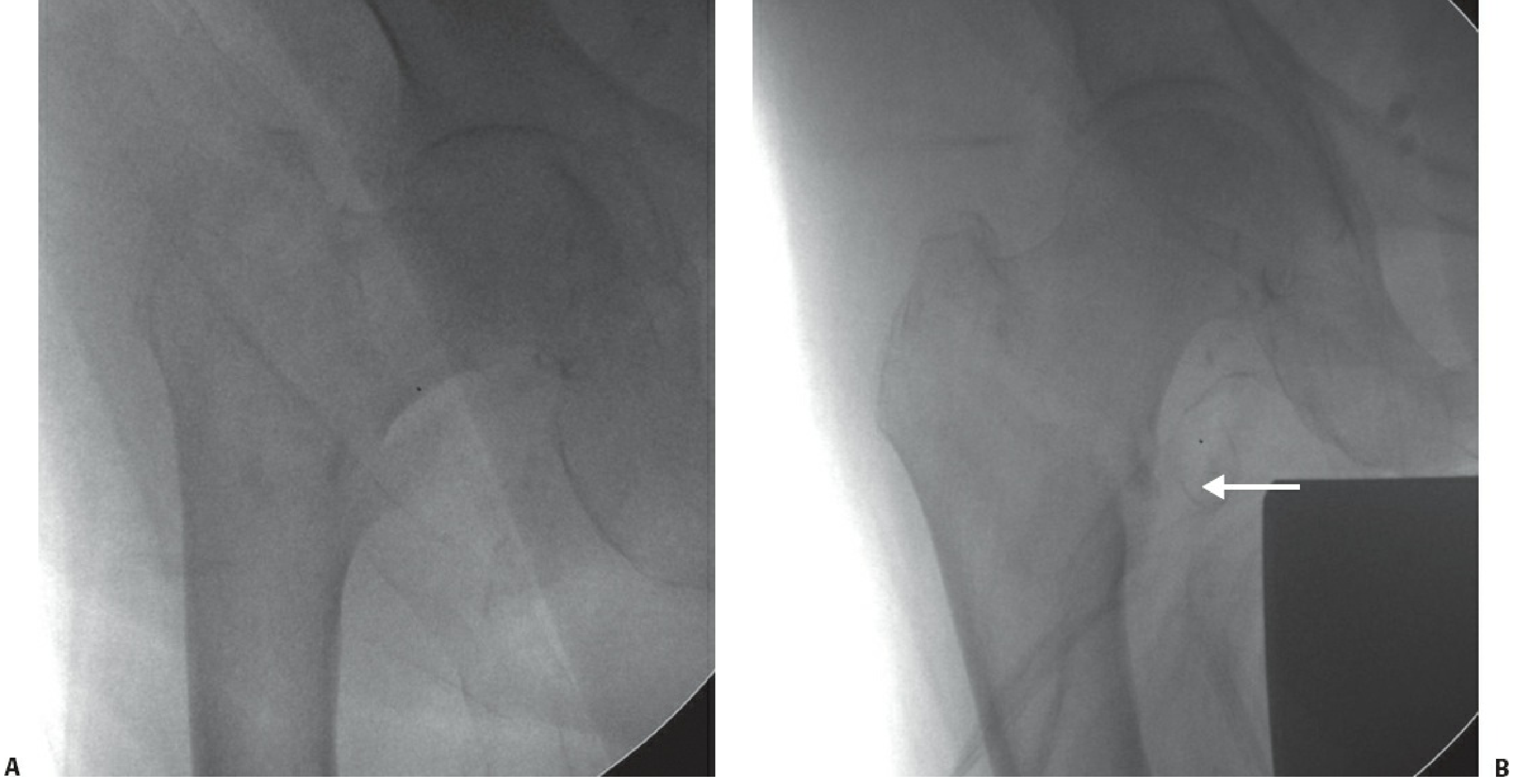
| 6. Lag screw guidewire | Target center-center on AP (inferior half acceptable), center on lateral - to achieve TAD <25 mm |
| 7. Measure lag screw length | From guidewire measurement; advance to 5-7 mm from the joint line |
| 8. Ream femoral neck | Over the guidewire to the appropriate lag screw diameter |
| 9. Insert lag screw | Anti-rotation: place a finger on the femoral neck anteriorly to resist head rotation; use anti-rotation pin/screw |
| 10. Distal interlocking | Static lock for unstable/subtrochanteric fractures; optional for stable intertrochanteric fractures |
| 11. Closure | Fascia lata closed; absorbable subcuticular skin sutures; pressure dressing |
- Rockwood and Green's Fractures in Adults 10th Ed, p. 2726-2727
The Tip-Apex Distance (TAD)
The TAD is the single most important predictor of lag screw cut-out.
TAD = distance from screw tip to femoral head apex on AP + distance on lateral view (corrected for magnification)
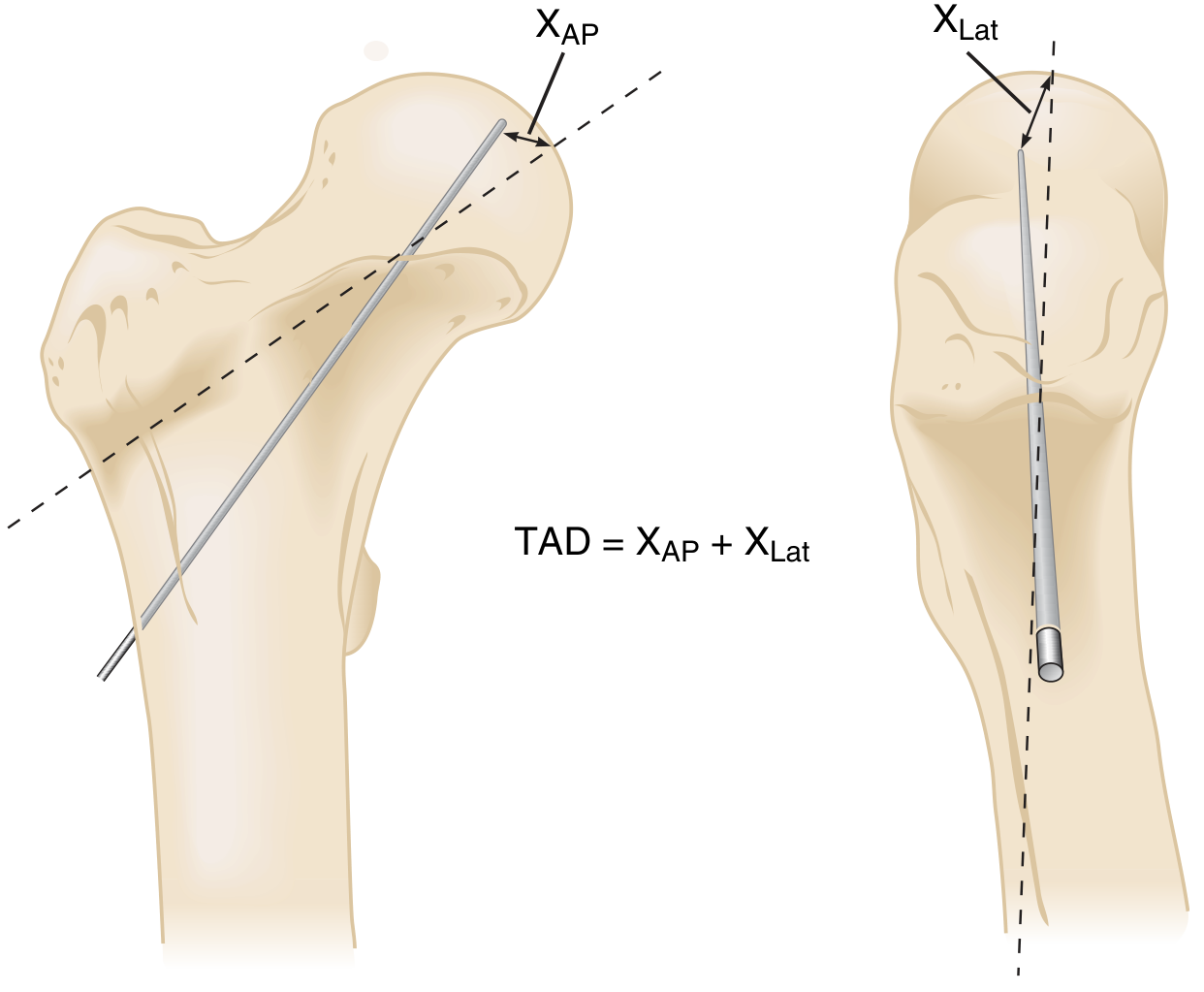
- TAD <25 mm - strongly associated with lowest cut-out rate
- TAD >25 mm - significantly higher risk of screw cut-out
- The ideal lag screw position is center-center on AP, center on lateral
Nail Length - Short vs. Long
| Short Nail | Long Nail |
|---|---|
| Standard oblique (AO 31-A1, A2) stable fractures | Reverse oblique (A3), subtrochanteric, fractures extending distally |
| Distal interlocking optional | Distal interlocking required |
| Cheaper | Reduces risk of stress fracture at nail tip |
A literature review of 1,276 patients found no statistically significant difference in periprosthetic fracture rate between short and long nails for standard intertrochanteric fractures, but long nails are preferred when the fracture pattern extends or to protect the entire femur.
Postoperative Care and Weight Bearing
- Immediate or early full weight bearing is the goal in elderly patients
- Physiotherapy and mobilization start on day 1 post-op
- Prophylactic anticoagulation for VTE prevention
- Transfer to a pressure-relieving mattress as soon as possible
Complications and Their Prevention
| Complication | Incidence | Prevention |
|---|---|---|
| Lag screw cut-out (varus collapse) | 1-5% | Valgus reduction + TAD <25 mm |
| Cut-in (craniomedial migration) | ~2% | Avoid jamming; correct positioning |
| Malunion (varus) | 5-10% | Correct reduction before fixation |
| Nonunion | 1-3% | Reduction + correct implant positioning |
| Implant breakage | 1-2% | Treat nonunion early |
| Avascular necrosis | ~1% | Avoid rotating femoral head at surgery |
| Anterior perforation distally | Rare | Match nail bow to femoral bow; avoid posterior entry |
| Superficial wound infection | 1-5% | Minimize exposure; prophylactic antibiotics |
| Deep wound infection | <1% | Strict aseptic technique |
| Peri-implant fracture at nail tip | Low | Long nail to bypass stress riser if fracture near tip |
- Rockwood and Green's Fractures in Adults 10th Ed, p. 2730
Cut-out is the most common mechanical failure. The lag screw fails to slide as the fracture collapses (jamming), acts as a fixed implant, and eventually breaches the femoral head.

CM Nail vs. Sliding Hip Screw (SHS) - Decision Guide
| Feature | SHS (DHS) | Cephalomedullary Nail |
|---|---|---|
| Cost | Lower | Higher (long nail costliest) |
| Stable intertrochanteric (A1, A2 with lateral wall >20.5 mm) | First choice | Also valid |
| Unstable intertrochanteric (reverse oblique, lateral wall <20.5 mm) | Higher failure rate | Preferred |
| Subtrochanteric extension | Contraindicated | Required |
| Collapse/medialization | More collapse | Less collapse (IM buttress) |
| Blood loss / operative time | Similar | Similar |
| Risk of iatrogenic lateral wall fracture | Yes (if wall thin) | Lower |
- Miller's Review of Orthopaedics 9th Ed, p. 918
This is a shared conversation. Sign in to Orris to start your own chat.