Change of supine to standing position cause tachycardiya why
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Here is the full explanation:
Why Does Changing from Supine to Standing Cause Tachycardia?
This is a normal cardiovascular reflex involving gravity, venous return, baroreceptors, and the autonomic nervous system. The sequence of events is as follows:
Step 1 - Gravitational Blood Pooling
When you go from lying flat to upright, gravity causes 0.5 to 1 litre of blood to pool in the lower extremities and the splanchnic (gut) venous system.
Step 2 - Reduced Venous Return and Cardiac Output
This pooling reduces the amount of blood returning to the heart (venous return). Less venous return means:
- Reduced right heart filling
- Reduced stroke volume (Frank-Starling mechanism)
- Reduced cardiac output
- A transient fall in arterial blood pressure
Step 3 - Baroreceptor Detection
The arterial baroreceptors (mainly in the carotid sinus and aortic arch) detect the fall in blood pressure as reduced wall stretch. This causes a decrease in afferent baroreceptor firing to the brainstem (nucleus tractus solitarius).
Step 4 - Autonomic Response (the key step)
The brainstem responds to the reduced baroreceptor input by:
- Withdrawing parasympathetic (vagal) tone to the heart
- Increasing sympathetic tone to the heart and blood vessels
The result:
| Effect | Mechanism |
|---|---|
| Tachycardia | Increased sympathetic + reduced vagal tone to SA node |
| Increased contractility | Sympathetic stimulation of myocardium |
| Vasoconstriction | Sympathetic stimulation of arterioles and veins |
Together, these responses restore cardiac output and protect cerebral perfusion.
Summary Diagram
Supine → Standing
↓
Gravity → Blood pools in legs/abdomen (~500–1000 mL)
↓
↓ Venous return → ↓ Stroke volume → ↓ Cardiac output → ↓ BP
↓
↓ Baroreceptor firing (carotid sinus / aortic arch)
↓
↓ Parasympathetic tone + ↑ Sympathetic tone
↓
↑ Heart rate (tachycardia) + ↑ Contractility + Vasoconstriction
↓
BP and cardiac output restored → Cerebral perfusion maintained
Clinical Relevance
- A normal compensatory response: heart rate rises by about 10-20 bpm on standing.
- If this reflex fails or is exaggerated, it produces clinical conditions:
- Orthostatic hypotension: BP drops > 20/10 mmHg without adequate compensation (seen in autonomic neuropathy, hypovolemia, elderly patients).
- POTS (Postural Orthostatic Tachycardia Syndrome): exaggerated reflex where heart rate rises by > 30 bpm on standing without significant BP drop.
- The reflex can be tested clinically by measuring blood pressure and heart rate after lying flat for 10 minutes, then at 1, 3, and 5 minutes of standing.
Source: Braunwald's Heart Disease - A Textbook of Cardiovascular Medicine, "Orthostatic Blood Pressure" section
Peripheral resistence
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Here is a thorough explanation of peripheral resistance from first principles:
Peripheral Resistance (Total Peripheral Resistance / TPR)
Definition
Peripheral resistance (also called Total Peripheral Resistance, TPR, or Systemic Vascular Resistance, SVR) is the resistance offered by the entire systemic circulation to blood flow.
It is not measured directly - it is calculated from pressure and flow:
R = ΔP / F (Pressure difference ÷ Flow)
If the cardiac output is 100 mL/sec and the mean arterial pressure difference (aorta to vena cava) is 100 mm Hg:
TPR = 100 / 100 = 1 PRU (Peripheral Resistance Unit)
- In maximal vasoconstriction: TPR can rise to 4 PRU
- In maximal vasodilation: TPR can fall to 0.2 PRU
The Core Equation: Ohm's Law of Circulation
Just like electrical circuits, blood flow follows:
Blood Pressure (BP) = Cardiac Output (CO) × Total Peripheral Resistance (TPR)
This is the most important equation in cardiovascular physiology. It means:
- BP rises if CO rises or TPR rises
- BP falls if CO falls or TPR falls
Poiseuille's Law - What Determines Resistance?
From the Hagen-Poiseuille equation, resistance in a vessel is:
R = 8ηl / πr⁴
Or equivalently, flow is:
F = ΔP × πr⁴ / 8ηl
| Variable | Symbol | Effect on Resistance |
|---|---|---|
| Vessel radius | r | ↑ radius → resistance falls by 4th power |
| Vessel length | l | ↑ length → ↑ resistance (proportional) |
| Blood viscosity | η | ↑ viscosity → ↑ resistance (proportional) |
The 4th Power Law - Most Important Factor
A 2-fold increase in radius → 16-fold increase in flow (2⁴ = 16)
A 4-fold increase in radius → 256-fold increase in flow (4⁴ = 256)
This is why small changes in arteriole diameter have enormous effects on blood flow and resistance.
Where Does Peripheral Resistance Come From?
The arterioles are the main site of resistance - they contribute ~2/3 of total systemic resistance. Their inner diameters range from 4 to 25 micrometres, and their muscular walls can change their diameter up to 4-fold, creating huge swings in resistance.
| Vessel Type | Contribution to Resistance |
|---|---|
| Arterioles | ~65-70% (main resistance vessels) |
| Capillaries | ~25% |
| Veins/venules | ~5% |
Factors That Increase Peripheral Resistance
| Factor | Mechanism |
|---|---|
| Vasoconstriction (arterioles) | Smooth muscle contraction → ↓ radius → ↑ resistance |
| Sympathetic stimulation | Noradrenaline on α₁ receptors → vasoconstriction |
| Angiotensin II | Potent vasoconstrictor |
| Endothelin | Vasoconstrictor from endothelium |
| Increased blood viscosity | e.g., polycythaemia, dehydration |
| Increased vessel length | e.g., obesity (more tissue = more vessels to perfuse) |
Factors That Decrease Peripheral Resistance
| Factor | Mechanism |
|---|---|
| Vasodilation | Smooth muscle relaxation → ↑ radius → ↓ resistance |
| Nitric oxide (NO) | Produced by endothelium, causes vasodilation |
| Prostacyclin | Vasodilator |
| Local metabolites (CO₂, lactic acid, adenosine) | Vasodilation during exercise |
| Calcium channel blockers | Relax vascular smooth muscle |
| ACE inhibitors / ARBs | Block angiotensin II |
| Anaemia | ↓ viscosity → ↓ resistance |
Series vs. Parallel Arrangement
Series (arteries → arterioles → capillaries → venules → veins):
R_total = R1 + R2 + R3 + ... Each segment adds to total resistance.
Parallel (organs in parallel - brain, kidney, muscle, gut, skin):
1/R_total = 1/R1 + 1/R2 + 1/R3 + ... Adding more parallel pathways REDUCES total resistance. This is why removing a kidney or amputating a limb increases TPR - one parallel pathway is lost.
Clinical Significance
| Condition | Change in TPR | Effect |
|---|---|---|
| Hypertension | ↑ TPR | BP rises |
| Septic shock | ↓↓ TPR (massive vasodilation) | BP falls |
| Exercise | ↓ TPR in muscles (vasodilation) | local flow ↑ |
| Standing up | ↑ TPR (reflex vasoconstriction) | protects BP |
| Polycythaemia | ↑ TPR (↑ viscosity) | ↑ BP, ↑ clot risk |
| Heart failure (compensated) | ↑ TPR (compensatory) | maintains BP |
Summary Diagram
BP = CO × TPR
↑
|
[Arterioles] ← main site
|
Radius (most powerful - 4th power)
Viscosity (hematocrit, proteins)
Length (vessel anatomy)
Sources: Guyton and Hall Textbook of Medical Physiology; Medical Physiology (Boron & Boulpaep)
How does peripheral resistance change during exercise vs. at rest?
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Excellent sources retrieved. Here is the complete answer:
Peripheral Resistance: Exercise vs. Rest
The Short Answer
During exercise, Total Peripheral Resistance (TPR) falls markedly (↓↓), even though the sympathetic nervous system is highly activated. This seems paradoxical but makes perfect sense once you understand the two competing mechanisms at work.
The Two Competing Mechanisms
Exercise triggers two simultaneous processes that pull TPR in opposite directions:
| Mechanism | Effect on TPR | Where it acts |
|---|---|---|
| Central command (sympathetic) | ↑ Vasoconstriction | Skin, gut (splanchnic), kidneys, inactive muscles |
| Local metabolites (active hyperemia) | ↓↓ Vasodilation | Exercising skeletal muscle, coronary, cerebral |
The local vasodilation in skeletal muscle wins overall - it is so massive that it overwhelms the sympathetic vasoconstriction in other beds, and TPR falls as a net result.
Mechanism 1: Central Command (Sympathetic Activation)
When exercise begins (or is even just anticipated), the cerebral motor cortex issues a "central command" that:
- ↑ Sympathetic outflow to heart and vessels
- ↓ Parasympathetic outflow to the heart
This causes vasoconstriction via α₁ receptors in:
- Splanchnic (gut) circulation
- Renal circulation
- Skin (initially)
- Inactive skeletal muscles
This vasoconstriction redirects blood away from non-essential organs and toward the working muscles. On its own, this would raise TPR. But mechanism 2 overrides it.
Mechanism 2: Local Metabolic Vasodilation (Active Hyperemia)
As skeletal muscle contracts and its metabolic rate rises, it releases vasodilatory metabolites locally:
- Lactate (↓ local pH)
- K⁺ (potassium ions)
- Adenosine
- CO₂
- Nitric oxide (NO)
These act directly on arterioles within the exercising muscle to cause massive local vasodilation. This is called active hyperemia - blood flow follows metabolic demand.
This vasodilation in exercising muscle overrides any sympathetic vasoconstriction there, so muscle arterioles dilate even in the face of a highly activated sympathetic system.
Net Result: Why TPR Falls
Because skeletal muscle makes up ~40% of body mass, massive vasodilation across all active muscle beds causes such a large drop in resistance that the TPR falls overall, even though other vascular beds are constricted.
Full Summary Table (Costanzo Physiology)
| Parameter | At Rest | During Exercise |
|---|---|---|
| Heart rate | Normal | ↑↑ |
| Stroke volume | Normal | ↑ |
| Cardiac output | ~5 L/min | ↑↑ (up to 20-25 L/min) |
| Venous return | Normal | ↑ |
| Total Peripheral Resistance | Normal (~1 PRU) | ↓↓ |
| Mean arterial pressure | ~93 mmHg | ↑ (slight) |
| Systolic BP | ~120 mmHg | ↑ (increased stroke volume) |
| Diastolic BP | ~80 mmHg | Same or ↓ (due to ↓ TPR) |
| A-V O₂ difference | Normal | ↑↑ |
Why Does Blood Pressure Still Rise Then?
Using: BP = CO × TPR
- CO increases massively (up to 5x at maximal exercise)
- TPR falls (but not 5x)
- Net effect: BP rises slightly - mainly systolic BP rises (due to larger stroke volume), while diastolic may stay the same or even fall (due to low TPR)
Cardiovascular Flow Chart During Exercise
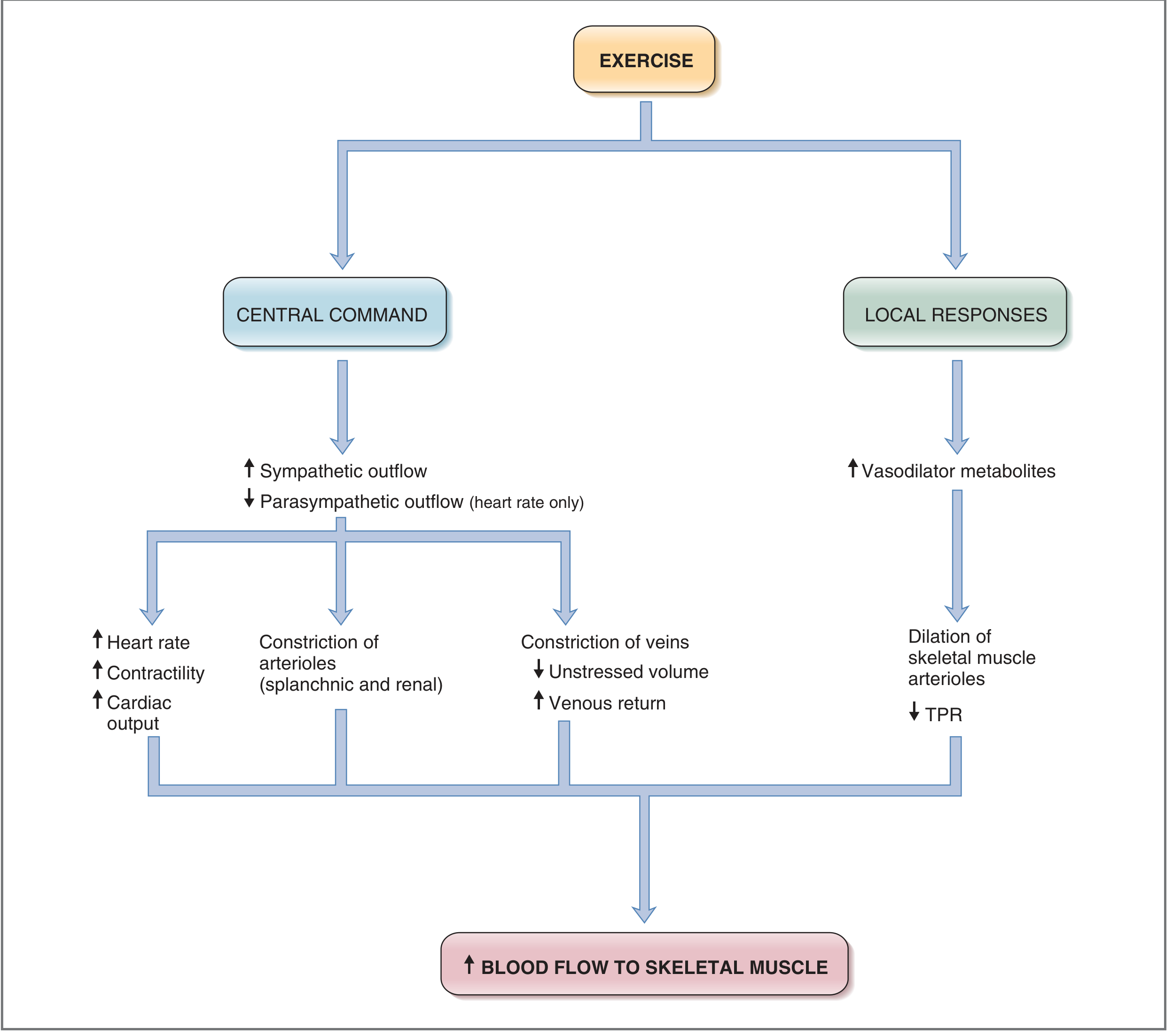
Fig. 4.35 - Cardiovascular responses to exercise. (Costanzo Physiology, 7th Edition)
Blood Flow Redistribution at Rest vs. Exercise
| Organ/Region | At Rest | Strenuous Exercise |
|---|---|---|
| Skeletal muscle | ~20% | ~80-85% |
| Coronary | ~5% | ↑↑ (stays protected) |
| Brain | ~15% | Maintained |
| Gut/Splanchnic | ~25% | ↓↓ (vasoconstricted) |
| Kidneys | ~20% | ↓↓ (vasoconstricted) |
| Skin | ~10% | ↓ initially, then ↑ (heat dissipation) |
Key Points to Remember
- TPR falls during exercise - driven by massive vasodilation in working muscles (active hyperemia)
- Sympathetic activity rises, causing vasoconstriction in gut/kidney/inactive muscle - but this is overridden locally in exercising muscle
- BP rises slightly because the large increase in CO outweighs the fall in TPR
- Skeletal muscle arterioles dilate due to local metabolites (lactate, K⁺, adenosine) regardless of sympathetic tone
- Diastolic BP may actually fall or stay unchanged - a useful clinical point
Sources: Costanzo Physiology 7th Edition; Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.