Alopecia types and patterns
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, well-sourced information to compile a thorough answer. Here is the full response:
Alopecia: Types and Patterns
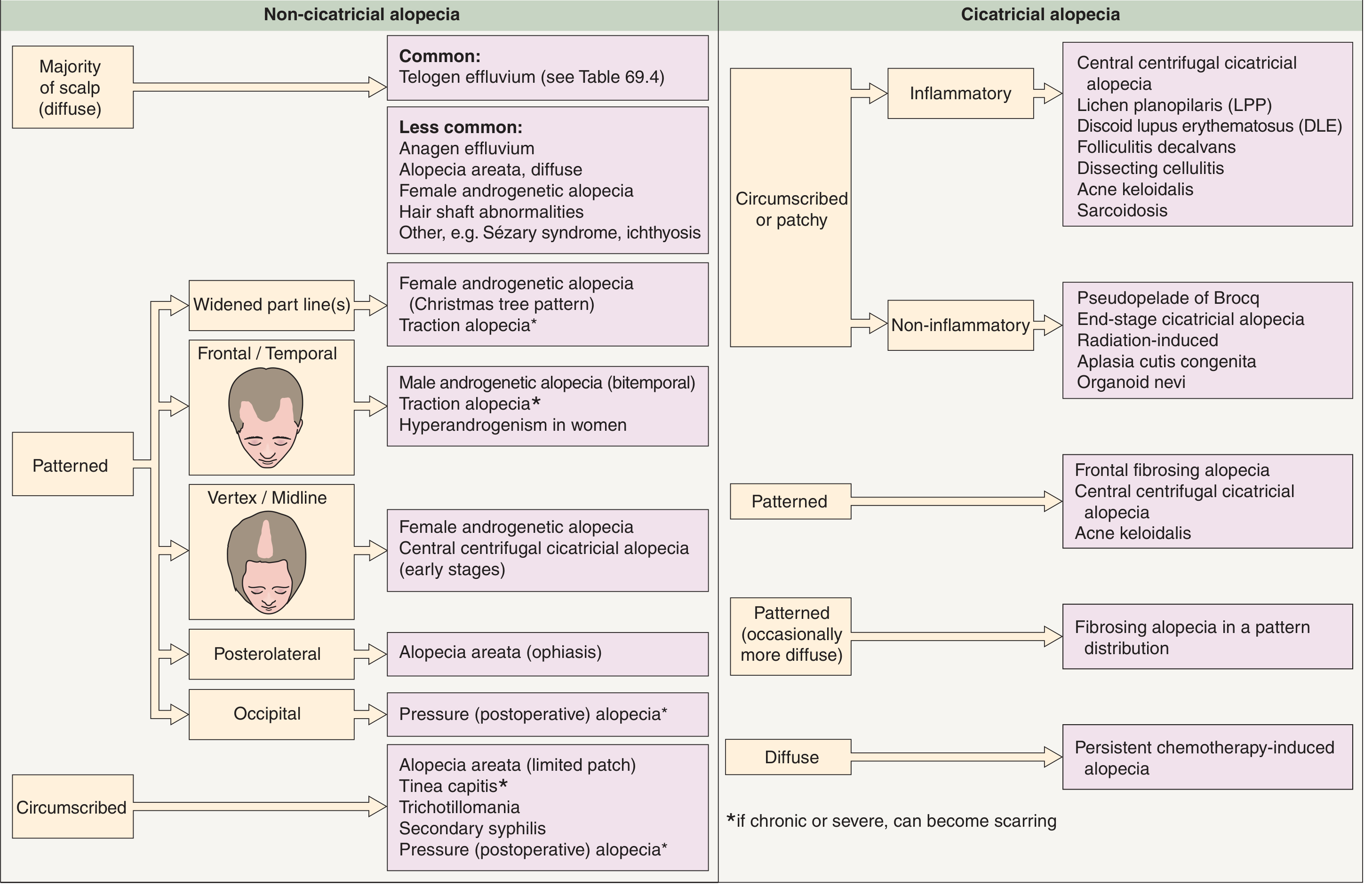
Alopecia (hair loss) is classified along two major axes: scarring (cicatricial) vs. non-scarring (non-cicatricial), and diffuse vs. patterned vs. circumscribed. This framework drives clinical approach and diagnosis.
Clinical Classification Framework
I. NON-SCARRING (NON-CICATRICIAL) ALOPECIA
Hair follicles are preserved; hair shafts are absent or miniaturized. This explains the reversible nature of most non-scarring alopecias. A smooth scalp with maintained follicular openings is the hallmark.
1. Androgenetic Alopecia (Pattern Alopecia)
The most common form of hair loss, affecting up to 80% of men and 50% of women during their lifetime.
Pathogenesis: Progressive follicular miniaturization driven by DHT (dihydrotestosterone), the product of testosterone reduced by 5α-reductase. DHT binds androgen receptors in susceptible follicles, leading to shortening of the anagen (growth) phase, progressive reduction in hair shaft diameter and pigmentation, and eventual conversion of terminal hairs to vellus hairs. Androgen-inducible TGF-β1 from dermal papilla cells mediates growth suppression. Eunuchs castrated before puberty do not develop pattern alopecia, confirming androgen dependence.
Male pattern (Hamilton-Norwood scale):
- Begins in teens, twenties, or early thirties
- Bi-parietal recession ("Geheimratswinkeln" / professor angles) with vertex loss
- Progressive until entire vertex/frontotemporal scalp is devoid of terminal hair
- Parietal and occipital areas are permanently spared
Female pattern (Ludwig scale):
- Diffuse thinning of the crown with preservation of the frontal hairline ("Christmas tree pattern" on part-line widening)
- Compare hair density at vertex vs. occiput
- In premenopausal women, may signal hyperandrogenism (consider DHEA-S, free testosterone)
Histology: Decrease in anagen/telogen ratio, follicular miniaturization, variability in shaft diameter, fibromucinous fibrous tract remnants below miniaturized follicles, sebaceous gland enlargement. Inflammatory cells absent (unlike cicatricial alopecias).
Trichoscopy: >20% variability in hair diameter is a key diagnostic sign.
- Andrews' Diseases of the Skin, p. 870; Goldman-Cecil Medicine, p. 4330; Dermatology 2-Volume Set 5e, p. 1391
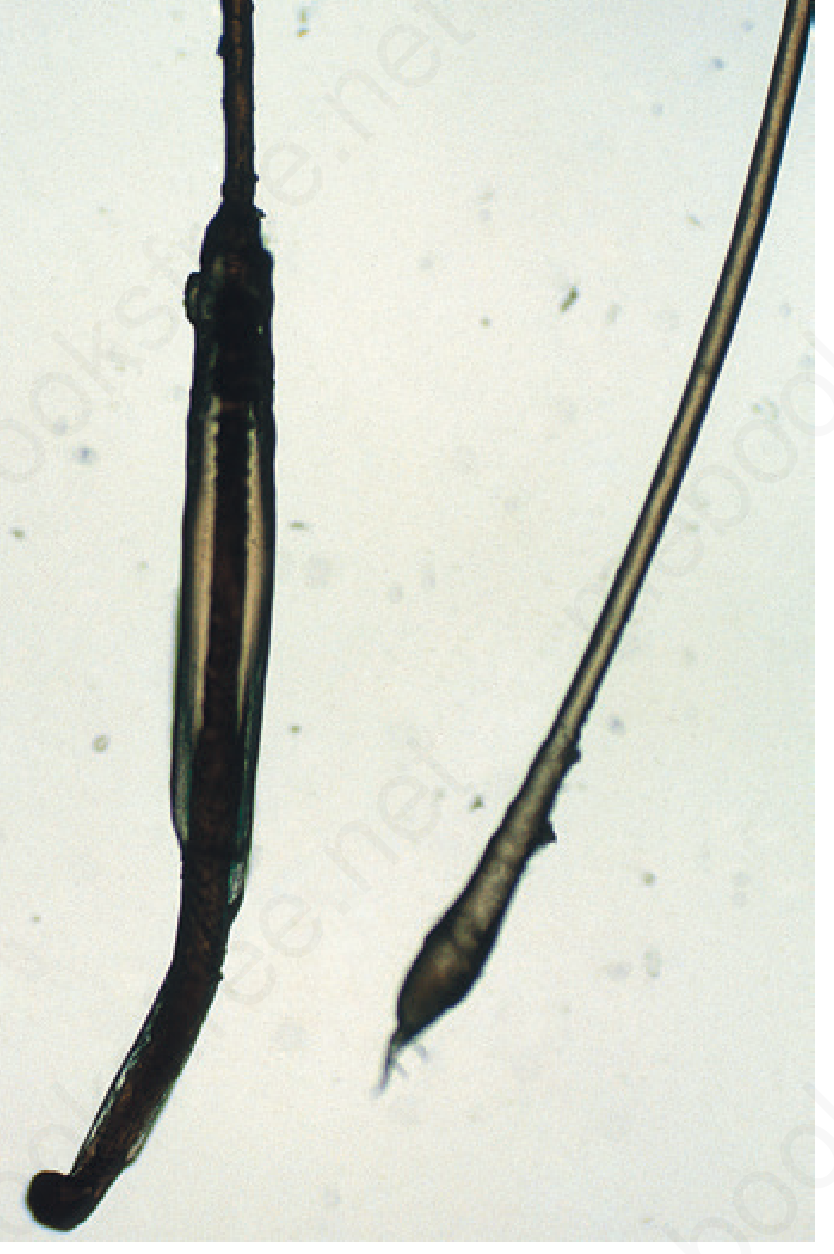
2. Telogen Effluvium
Mechanism: Premature conversion of anagen hairs to telogen, followed by synchronous shedding 3-5 months later. Triggers include surgery, parturition, fever, severe illness, crash dieting, medications, and stress. Hair is lost "at the root" with a visible depigmented club bulb and no root sheath.
Clinical features:
- Diffuse scalp shedding (150-400+ hairs/day vs. normal 100-150)
- Pull test: >4-6 club hairs abnormal (adjust for recent shampooing)
- Usually reversible once trigger is removed
Causes:
- Post-partum (common; follicles held in prolonged anagen during pregnancy, then synchronously released)
- Febrile illness, surgery, crash dieting
- Drugs (see drug-induced section below)
- Hypothyroidism/hyperthyroidism
- Chronic telogen effluvium (idiopathic, >6 months, mainly women)
- Andrews' Diseases of the Skin, p. 870
3. Anagen Effluvium
Mechanism: Abrupt inhibition of mitotic activity in follicular matrix cells during the growth (anagen) phase. Anagen follicles with highest mitotic activity are most affected.
Key causes:
- Chemotherapy (anthracyclines, alkylating agents, topoisomerase inhibitors cause near-total alopecia)
- Radiation therapy
- Hair shedding starts 4-6 weeks after drug exposure, up to 1000 hairs/day
- Regrowth usually follows discontinuation; permanent loss may occur with high-dose radiation, busulfan, or docetaxel regimens
Clinical note: Scalp hypothermia (chemo caps) can reduce or prevent alopecia but is controversial in curative-intent hematologic malignancies (richly vascularized scalp may harbor micrometastases).
- Harrison's Principles of Internal Medicine 22E, p. 2109; Goldman-Cecil Medicine, p. 4329
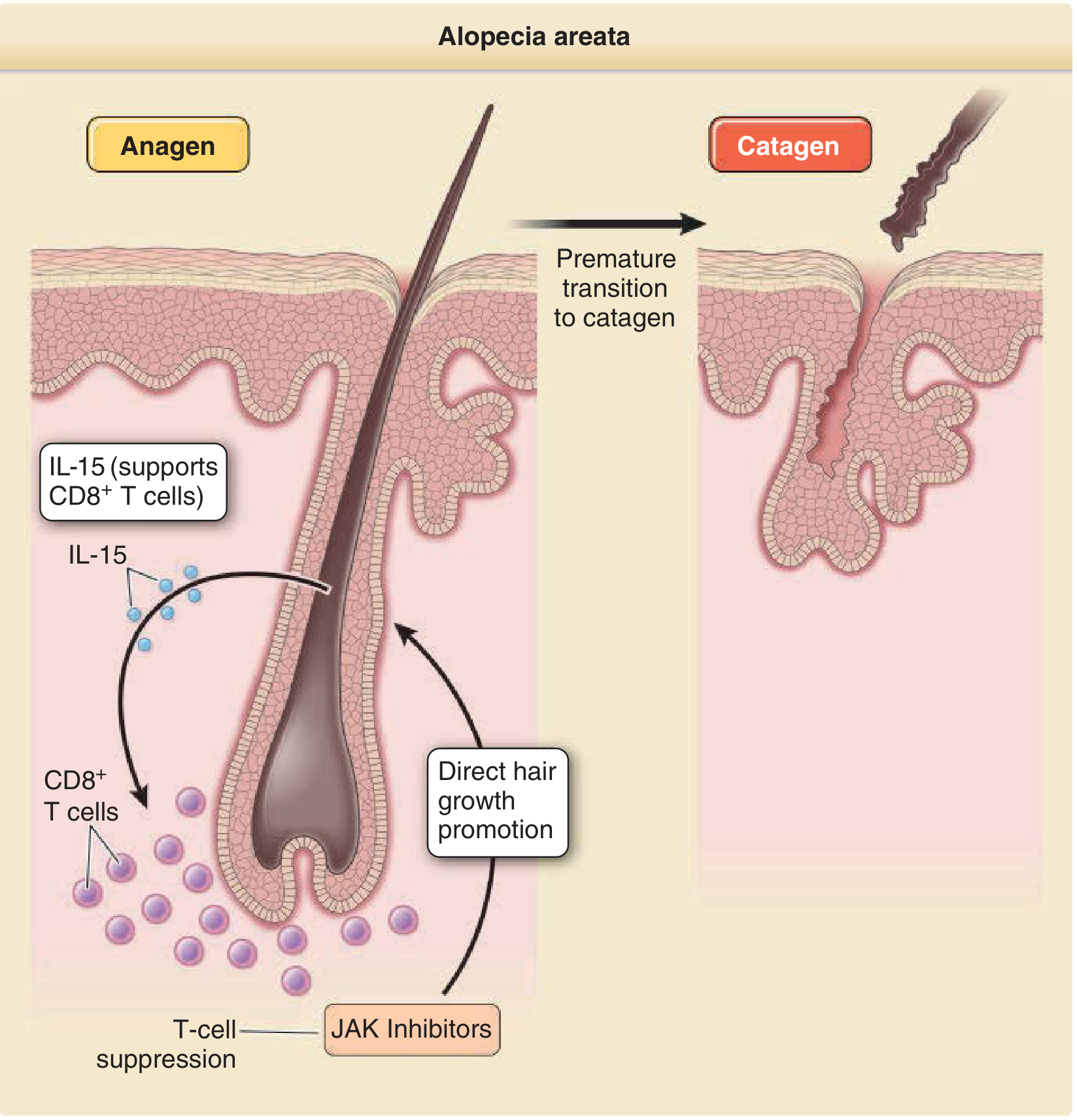
4. Alopecia Areata (AA)
Mechanism: Autoimmune, T-cell mediated (predominantly CD8+ cytotoxic T cells, IL-15, IFN-γ) attack on anagen hair bulbs. Loss of "immune privilege" of the hair follicle allows lymphocytic infiltration. The bulge (stem cell region) is spared, explaining reversibility.
Three major phenotypic variants:
| Variant | Description |
|---|---|
| Patchy AA | Circumscribed coin-shaped bald patches on scalp |
| Alopecia totalis | Complete loss of scalp hair |
| Alopecia universalis | Complete loss of all body hair (scalp + integument) |
| Ophiasis | Band-like loss along posterolateral scalp margin |
Trichoscopy: Yellow dots, exclamation mark hairs, broken hairs.
Associations: Thyroiditis and other autoimmune diseases.
- Fitzpatrick's Dermatology, p. 229; Goldman-Cecil Medicine
5. Traction Alopecia
Hair loss from mechanical stress - excessive hair straightening, braiding, tight ponytails, or extensions. Typically affects the frontal/temporal hairline. If chronic or severe, can progress to permanent scarring (cicatricial conversion).
6. Trichotillomania
Compulsive hair pulling producing irregular patchy loss with hairs broken at different lengths. Trichoscopy shows broken hairs and question mark hairs (distinctive from AA's exclamation mark hairs).
7. Tinea Capitis
Dermatophyte scalp infection producing circumscribed patches with scaling, broken "comma" or corkscrew hairs on trichoscopy. Predominantly in children.
8. Drug-Induced Alopecia
Drugs can cause either telogen effluvium (most) or anagen effluvium (chemotherapy). Key culprits include:
| Category | Examples |
|---|---|
| Anticoagulants | Warfarin, heparin, apixaban, dabigatran |
| Antithyroid | Carbimazole, propylthiouracil |
| Antiepileptics | Valproic acid, carbamazepine |
| Retinoids | Isotretinoin, acitretin |
| Beta-blockers | Propranolol, metoprolol |
| Cardiac | Amiodarone |
| Chemotherapy | Anthracyclines, alkylating agents, taxanes |
| Other | Lithium, interferons, colchicine, amphetamines |
Spontaneous regrowth usually follows discontinuation.
9. Systemic Causes (Diffuse Non-Scarring)
- Lupus erythematosus: Two forms - (1) non-scarring coinciding with disease flares ("lupus hairs," short regrowth hairs at frontal scalp); (2) scarring from discoid lesions
- Secondary syphilis: "Moth-eaten" patchy alopecia
- Hypothyroidism/hyperthyroidism: Diffuse thinning
- Nutritional deficiencies: Iron, zinc, protein
II. SCARRING (CICATRICIAL) ALOPECIA
The hallmark is loss of follicular ostia (follicular openings). Fibrosis replaces follicles, and hair loss is permanent. Treatment can halt progression but not restore lost hair. Biopsy should be taken from areas of active inflammation (periphery of patches, not the atrophic center).
Primary Cicatricial Alopecias
Classified by predominant inflammatory cell on histopathology:
Lymphocytic
| Condition | Key Features |
|---|---|
| Lichen planopilaris (LPP) | Most common cicatricial alopecia; perifollicular erythema/scaling; severe pruritus; peripilar casts on trichoscopy; violaceous perifollicular macules at periphery |
| Frontal fibrosing alopecia (FFA) | Variant of LPP; postmenopausal women most affected; recession of fronto-temporal hairline with associated eyebrow and eyelash/body hair loss; shows no photoaging in the alopecic band |
| Discoid lupus erythematosus (DLE) | Erythematous scaly active lesions at periphery; central hypopigmentation with rim of hyperpigmentation; red dots and follicular plugs on trichoscopy; direct immunofluorescence helpful |
| Central centrifugal cicatricial alopecia (CCCA) | Centrifugal spread from crown vertex outward; predominantly African American women |
Neutrophilic
| Condition | Key Features |
|---|---|
| Folliculitis decalvans | Follicular pustules at periphery of patches; hair tufts on trichoscopy; may cause reactive arthritis |
| Dissecting cellulitis | Fluctuant nodules and sinuses on vertex/occiput |
Other Primary
- Acne keloidalis nuchae: Follicular pustules at occiput/nape, keloid-like scarring
- Sarcoidosis: Plaques on scalp with dermal granulomas on biopsy; virtually always in African/African American women
Secondary Cicatricial Alopecias
Result from disorders scarring the dermis secondarily:
- Burns, radiation (high-dose)
- Severe skin infections
- Localized scleroderma (morphea)
- Scalp tumors / cutaneous metastases
- Pseudopelade of Brocq (end-stage, non-inflammatory)
III. PATTERN SUMMARY TABLE
| Distribution | Non-Cicatricial Cause | Cicatricial Cause |
|---|---|---|
| Diffuse | Telogen effluvium (most common), anagen effluvium, diffuse AA, FAGA, hypothyroidism | Persistent chemo-induced alopecia |
| Widened part line | FAGA (Christmas tree pattern), traction | - |
| Frontal/temporal | Male AGA (bitemporal), traction, hyperandrogenism in women | Frontal fibrosing alopecia |
| Vertex/midline | FAGA, early CCCA | CCCA, patterned fibrosing alopecia |
| Posterolateral | Alopecia areata (ophiasis pattern) | - |
| Occipital | Pressure alopecia | Acne keloidalis |
| Circumscribed/patchy | AA (limited patch), tinea capitis, trichotillomania, secondary syphilis | LPP, DLE, folliculitis decalvans, dissecting cellulitis, sarcoidosis |
IV. TRICHOSCOPY (DERMATOSCOPY) QUICK REFERENCE
| Condition | Trichoscopic Findings |
|---|---|
| Alopecia areata | Yellow dots, exclamation mark hairs, broken hairs |
| Androgenetic alopecia | >20% variability in hair diameter |
| Lichen planopilaris / FFA | Peripilar casts; loss of follicular openings |
| Trichotillomania | Broken hairs, question mark hairs |
| Tinea capitis | Comma hairs, corkscrew hairs |
| Discoid lupus | Red dots, follicular plugs |
| Folliculitis decalvans | Hair tufts |
| Scalp psoriasis | Coiled capillaries |
| Seborrheic dermatitis | Arborizing vessels |
Goldman-Cecil Medicine International Edition, p. 4329
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Andrews' Diseases of the Skin | Goldman-Cecil Medicine | Dermatology 2-Volume Set 5e (Dermatology Bologniaet al.) | Fitzpatrick's Dermatology
This is a shared conversation. Sign in to Orris to start your own chat.