Investigation finding in mi
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive data from multiple authoritative textbooks to compose a detailed answer. Let me compile everything.
Investigation Findings in Myocardial Infarction (MI)
Investigations in MI are grouped into ECG, cardiac biomarkers, imaging, and general labs. Both STEMI and NSTEMI are covered below.
1. Electrocardiogram (ECG)
The ECG is the cornerstone of immediate MI diagnosis. Three membrane-potential changes in infarcted cells cause ECG changes (Ganong's Review of Medical Physiology):
| Defect in Infarcted Cells | Current Flow | ECG Change in Leads over Infarct |
|---|---|---|
| Rapid repolarization | Out of infarct | ST segment elevation |
| Decreased resting membrane potential | Into infarct | TQ segment depression (manifested as ST elevation) |
| Delayed depolarization | Out of infarct | ST segment elevation |
ECG Changes by Phase
Hyperacute / Early (minutes to hours):
- Tall, peaked (hyperacute) T waves - earliest change
- ST segment elevation (hallmark of STEMI) - >1 mm in 2 or more contiguous limb leads, or >2 mm in 2 or more contiguous precordial leads
- ST elevation represents current of injury
Evolving (hours to days):
- ST elevation becomes more pronounced
- T wave inversion develops
- Q waves begin to appear (pathological Q width >40 ms, depth >25% of the R wave)
Established / Chronic (days to weeks):
- ST segments return toward baseline
- Deep T wave inversions
- Persistent pathological Q waves (permanent marker of necrosis)
- "Failure of R wave progression" in anterior MI
NSTEMI / Unstable Angina ECG
- No ST elevation
- New ST segment depression (occurs in ~1/3 of NSTEMI patients)
- T wave changes are common but less specific; new deep T wave inversions (≥0.3 mV) are more significant
- Wellens syndrome: deep, symmetric T wave inversions in V2-V3 = critical LAD stenosis
ECG Localisation of Infarct
| Leads with Changes | Territory | Artery |
|---|---|---|
| V1-V4 | Anterior | LAD |
| V1-V2 | Septal | LAD (septal branch) |
| V5-V6, I, aVL | Lateral | LCx |
| II, III, aVF | Inferior | RCA (or LCx) |
| V7-V9 (reciprocal V1-V3 depression) | Posterior | RCA / LCx |
| V1, V4R | Right ventricle | RCA |
2. Cardiac Biomarkers
The most important investigations - biomarkers are proteins that leak from necrotic myocardial cells through damaged membranes.
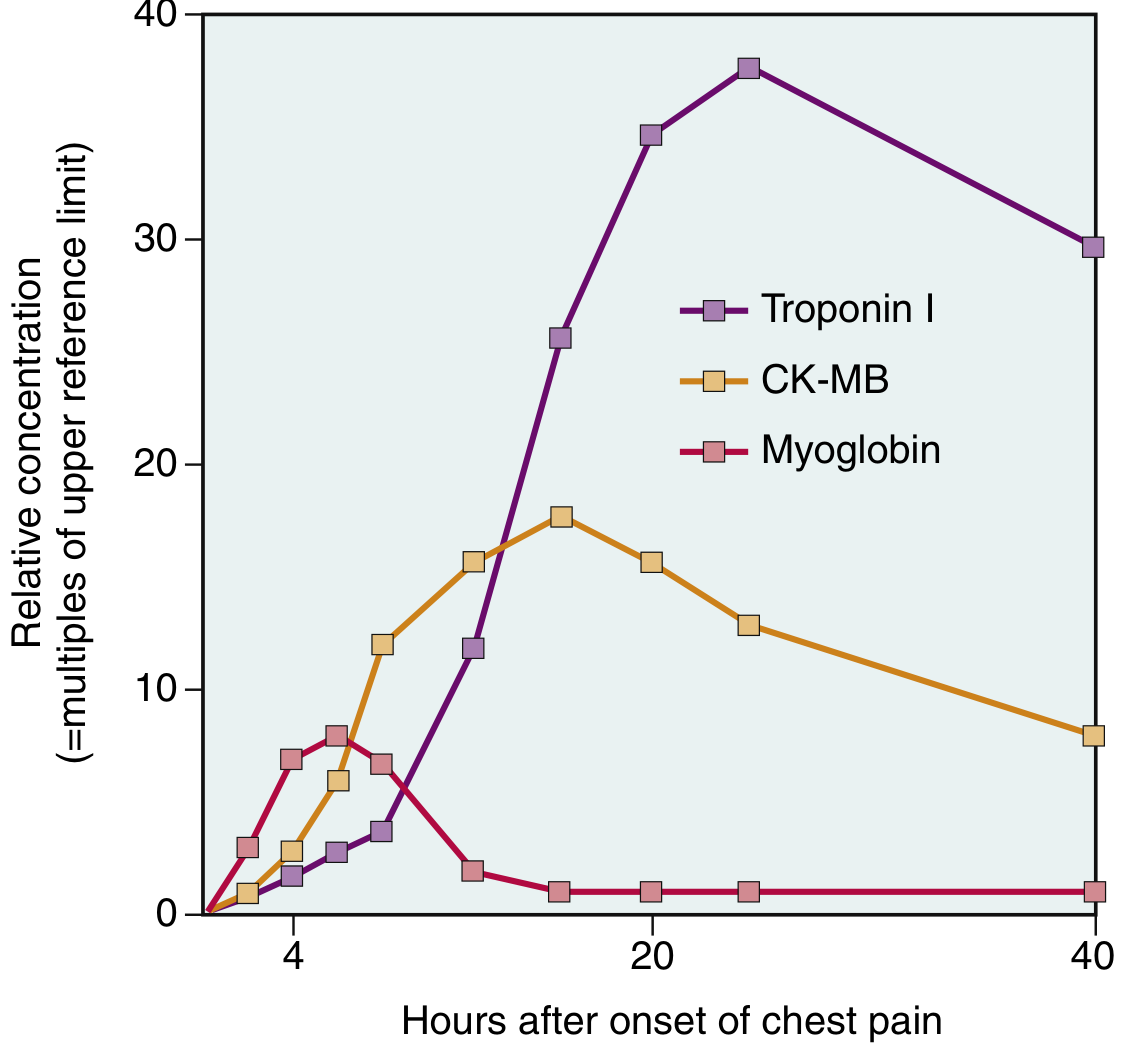
Figure: Acute increases in myocardium-derived Troponin I, CK-MB, and Myoglobin following MI. Note the persistence of Troponin I for up to 7-10 days. (Robbins & Kumar Basic Pathology)
Troponin I and Troponin T (cTnI, cTnT) - Gold Standard
- Cardiac-specific regulatory proteins not normally found in the circulation
- Rise: 2-4 hours after infarct onset
- Peak: ~48 hours
- Return to normal: 7-10 days (cTnI), up to 14 days (cTnT)
- Diagnosis: elevation >99th percentile of the upper reference limit
- High-sensitivity troponin (hs-cTn): An undetectable level at presentation reduces the probability of acute MI to <1%; a 0-2 hour repeat protocol is as effective as longer observation
- Elevated troponin persists long after CK-MB returns to normal, enabling late diagnosis
- With reperfusion, levels peak earlier (washout effect)
CK-MB (Creatine Kinase - MB fraction)
- Rise: 2-4 hours
- Peak: 24-48 hours
- Return to normal: ~72 hours (3 days)
- No longer recommended as the primary marker for initial NSTEMI diagnosis (Washington Manual) - lacks specificity since it is present in both skeletal and cardiac muscle
- Still useful for detecting reinfarction (second rise after normalisation) since troponin remains elevated
Myoglobin
- Earliest rise: within 1-2 hours (first marker to rise)
- Peak: ~6-8 hours
- Return to normal: ~24 hours
- High sensitivity, very low specificity (present in skeletal muscle too) - used as an early rule-out only
Summary Table of Biomarker Kinetics
| Marker | Rises | Peaks | Returns to Normal | Specificity |
|---|---|---|---|---|
| Myoglobin | 1-2 h | 6-8 h | ~24 h | Low |
| CK-MB | 2-4 h | 24-48 h | 72 h (~3 days) | Moderate |
| Troponin I/T | 2-4 h | 48 h | 7-10 days | High (gold standard) |
Other Biomarkers
- BNP / NT-proBNP: Elevated with myocardial stress; associated with worse outcomes in ACS; severe elevation should raise concern for large infarction
- LDH (Lactate dehydrogenase): Historically used; rises late (24-48 h), peaks at 3-6 days, returns to normal over 8-14 days; less specific
- CBC: May show leukocytosis (neutrophilia) due to inflammatory response within 12-24 h; normalises over days
- ESR / CRP: Elevated as acute phase reactants; CRP begins rising within hours of necrosis
3. General Laboratory Investigations
| Investigation | Finding / Purpose |
|---|---|
| CBC | Leukocytosis (neutrophilia); detect anaemia (worsens ischemia) |
| BMP / Electrolytes | Hypokalemia/hypomagnesemia (arrhythmia risk); hyperkalemia (ECG changes) |
| Fasting glucose & HbA1c | DM is a major risk factor; hyperglycaemia worsens outcome |
| Lipid profile | Dyslipidaemia risk stratification |
| Renal function (Cr, eGFR) | Baseline before contrast use; CKD worsens prognosis |
| Coagulation (PT, aPTT) | Before thrombolytics/anticoagulants |
| Thyroid function | Hyperthyroidism can precipitate demand ischemia |
4. Imaging Investigations
Chest X-Ray
- May show cardiomegaly, pulmonary oedema/congestion (Kerley B lines, bat-wing opacity) in heart failure complicating MI
- Useful to exclude aortic dissection, pneumothorax as differential diagnoses
Echocardiography (Echo)
- Detects regional wall motion abnormalities (RWMA) - the earliest functional sign of ischemia (before biomarkers rise)
- Assesses LV ejection fraction (LVEF) - essential for prognosis and treatment planning
- Identifies mechanical complications: free wall rupture, VSD, papillary muscle rupture with mitral regurgitation, pericardial effusion
- Bedside echo is particularly useful when ECG is equivocal
CT Coronary Angiography (CTCA)
- Useful in low-to-intermediate risk ACS with equivocal ECG and troponin
- Rules out significant coronary stenosis in the emergency department
Invasive Coronary Angiography
- Definitive investigation for STEMI (emergency) and high-risk NSTEMI
- Identifies the culprit lesion and guides PCI
- Shows "vulnerable plaque": eccentric stenosis with scalloped edges and narrow neck
Cardiac MRI
- Provides detailed assessment of myocardial viability, infarct size, and function
- Distinguishes MI from myocarditis when presentation is ambiguous (both can have troponin rise + ECG changes)
5. Key Diagnostic Criteria Summary
STEMI diagnosis = Chest pain + ST elevation in ≥2 contiguous leads + troponin rise (biomarkers confirm, but treatment initiated on ECG alone)
NSTEMI diagnosis = Chest pain + abnormally elevated troponin (>99th percentile) + no ST elevation (GOLDMAN-CECIL Medicine)
NSTEMI vs Unstable Angina = Same presentation but NSTEMI has elevated troponin; UA has normal troponin
Sources:
- Robbins & Kumar Basic Pathology (9th ed.)
- Harrison's Principles of Internal Medicine, 22nd ed. (2025)
- Ganong's Review of Medical Physiology, 26th ed.
- Washington Manual of Medical Therapeutics
- Goldman-Cecil Medicine, International ed.
This is a shared conversation. Sign in to Orris to start your own chat.