sturge weber syndrome
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Sturge-Weber syndrome"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks and recent PubMed reviews. Here is the full synthesis:
Sturge-Weber Syndrome (SWS)
Also known as: Encephalotrigeminal Angiomatosis
SWS is a congenital, sporadic neurocutaneous (phacomatosis) disorder characterized by the triad of a facial port-wine stain, ipsilateral leptomeningeal angioma, and ocular abnormalities.
Epidemiology & Genetics
- Incidence: approximately 1 in 20,000 births
- Occurs sporadically in all races; no hereditary pattern
- Caused by a somatic (post-zygotic mosaic) activating mutation in GNAQ (chromosome 9q21.2), which encodes the alpha subunit of a heterotrimeric G-protein. The mutation reduces GTPase activity, increasing downstream cell signaling. Mutations in GNA11 have also been implicated.
- The mutation is not detectable on blood-based genetic testing (mosaic), so diagnosis relies on clinical and imaging findings.
- Pathogenesis: persistence of the primitive embryonal vascular plexus that normally regresses during the 9th fetal week (it develops in the 6th week around the cephalic neural tube and facial skin region).
Clinical Features (The Classic Triad)
1. Port-Wine Stain (Cutaneous Angioma)


- Involves the forehead and upper eyelid (V1 trigeminal distribution); may extend bilaterally or to trunk/limbs
- Usually obvious at birth; may thicken and develop nodular texture over time
- Reactive hypertrophy of adjacent bone and soft tissue may occur
- Only 10%-20% of children with an upper facial port-wine nevus have a leptomeningeal angioma
- Risk is higher when the forehead is involved + larger area of face covered (especially bilateral V1 or V1/V2/V3)
- A port-wine stain sparing the upper face rarely associates with intracranial angioma
2. Leptomeningeal Angioma (Neurological Features)
- Primarily parieto-occipital distribution, typically ipsilateral to the facial nevus
- Bilateral in at least 15% of patients (including some with unilateral facial nevus)
- The angioma causes abnormal venous drainage → chronic ischemia → cortical atrophy + calcification
Neurological manifestations:
| Feature | Detail |
|---|---|
| Epilepsy | 72-80% of unilateral; 93% of bilateral cases |
| Seizure onset | 75% in first year; 86% by age 2; 95% before age 5 |
| Seizure type | Initially focal motor or generalized tonic-clonic; also infantile spasms, myoclonic, atonic |
| Hemiparesis | Often develops acutely with first seizures; may be permanent |
| Homonymous hemianopia | Common (occipital region frequently involved) |
| Intellectual disability | ~50% of all patients; 92% of bilateral cases |
| Stroke-like episodes | TIA-like or single stroke episodes without seizures |
| Behavioral concerns | Frequent even in non-disabled patients |
- Seizure onset before age 2 years strongly predicts future intellectual disability and refractory epilepsy
- Children who never develop seizures usually maintain normal intelligence
- The condition tends to stabilize, leaving residual deficits without further deterioration
3. Ocular Features
- Glaucoma - the principal ocular complication; two age peaks: infancy and late childhood
- Buphthalmos (enlarged globe) - in some newborns
- Choroidal hemangioma - ipsilateral diffuse choroidal angioma
- Episcleral hemangioma
- Iris heterochromia - ipsilateral to the nevus
- Amblyopia, retinal detachment, progressive blindness if untreated
- Blood in the Schlemm canal on gonioscopy is a recognized sign
- Glaucoma can occur even in the absence of neurologic involvement
Classification (Roach Scale)
| Type | Features |
|---|---|
| Type I | Both facial angioma and leptomeningeal angioma |
| Type II | Facial angioma alone (no CNS involvement) |
| Type III | Isolated leptomeningeal angioma (no skin lesion) |
Imaging
MRI (modality of choice)
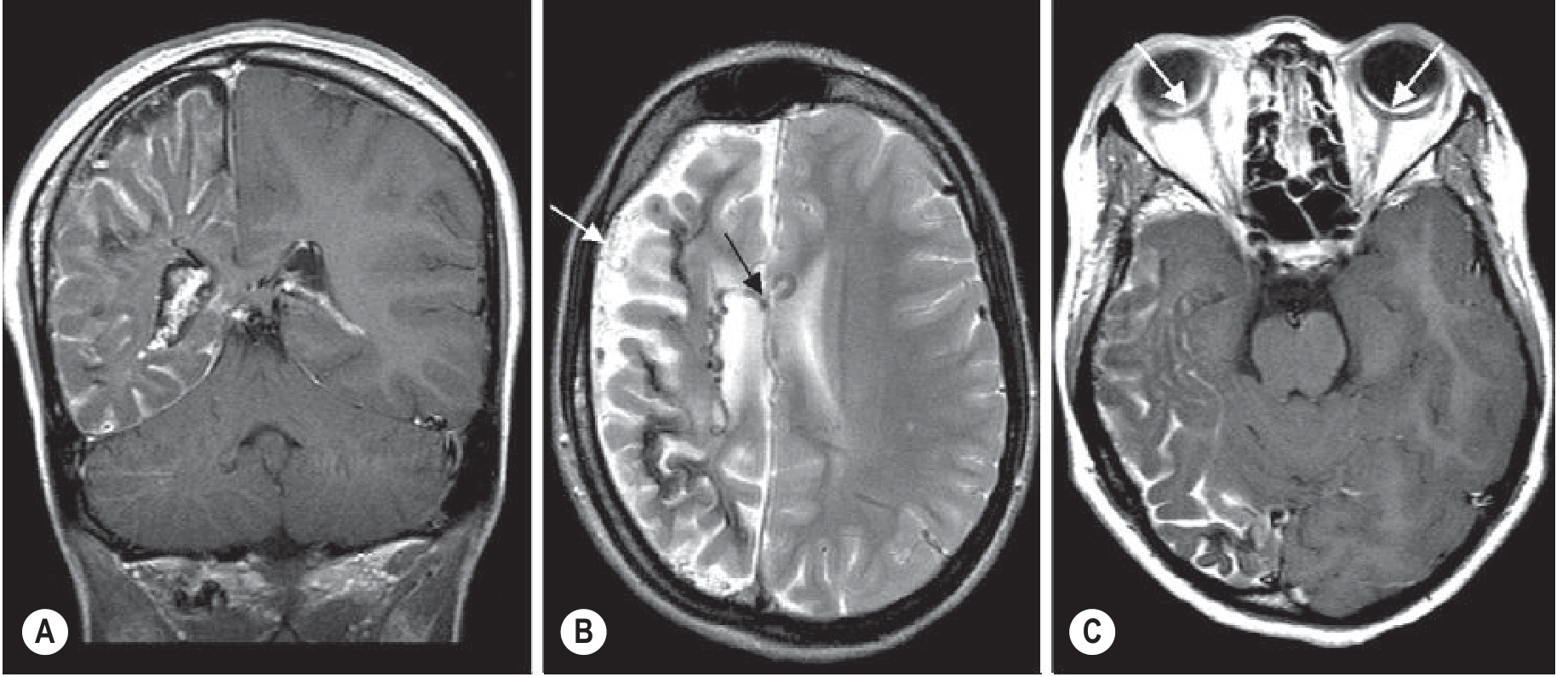
- Gadolinium-enhanced MRI: gold standard - shows diffuse pial enhancement of variable thickness (leptomeningeal angioma), ipsilateral hemispheric atrophy, enlarged choroid plexus, dilated transparenchymal veins
- In infants <2 years, the brain may look normal even on contrast MRI
- "Burnt out" cases: pial angioma no longer enhances; only chronically shrunken calcified hemisphere remains
- Polymicrogyria may be seen
CT
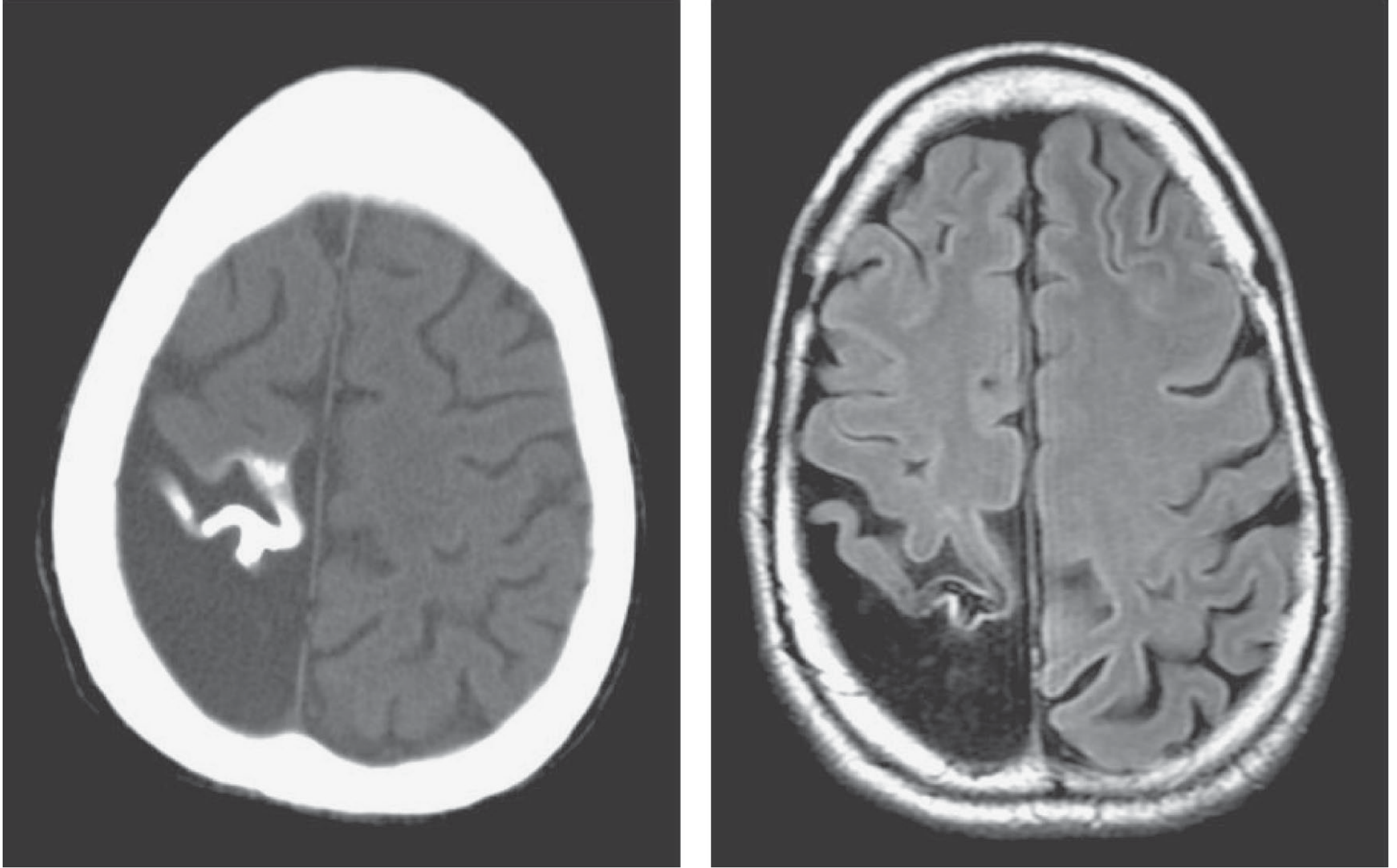
- Shows cortical calcification earlier than plain X-ray
- Classic "tram-track" (trolley-track) calcification in outer cortical layers - rare in neonates, develops by age 2
- T2* sequences / SWI on MRI also detect calcification
Other
- PET: reduced cortical metabolism near the angioma (increased in recent-onset seizures)
- SPECT: reduced perfusion; often shows abnormality beyond the CT/MRI extent
- Cerebral angiography: no longer routine; shows abnormal veins > arteries; sparse superficial cortical veins with enlarged deep medullary veins
Diagnosis
Diagnosis is clinical - based on the combination of:
- Port-wine stain (upper face/periorbital)
- Neuroimaging findings (leptomeningeal angioma, cortical atrophy, calcification)
- Characteristic neurological and ophthalmological features
Blood-based genetic testing is not useful (somatic mosaic mutation).
Key point: Most children with a facial port-wine nevus do NOT have an intracranial angioma. Early imaging (MRI preferred over CT in infancy) is warranted in those with significant upper facial port-wine stains to identify who needs prophylactic aspirin therapy.
Management
Seizures (Epilepsy)
- Antiepileptic drugs (AEDs) - first-line; generally the more extensive the lesion, the harder to control
- Surgical resection (lobectomy or hemispherectomy) - for refractory epilepsy; can improve seizure control and intellectual development. Patient selection: refractory seizures + clinical dysfunction of the area + failure of adequate AED trial
- Corpus callosotomy - for refractory tonic/atonic seizures with extensive disease
- Patients with less extensive lesions: limited resection preferred to preserve normal brain
Prophylaxis
- Low-dose aspirin - offered to reduce stroke-like episodes, seizures, and cognitive impairment; generally well-tolerated, but efficacy not firmly established by RCTs. Early imaging is now recommended so aspirin can be started early in confirmed cases.
Ophthalmological
- Screening for glaucoma must begin in infancy
- Periodic intraocular pressure measurement is mandatory when the nevus is near the eye
- Surgical management of glaucoma as needed
Skin (Port-Wine Stain)
- Pulsed-dye laser therapy - effective for decreasing skin discoloration; most effective when started early
- Topical preparations (imiquimod, rapamycin) alone or with adjuvant laser show promise
- Soft tissue debulking in severe cases
Recent Evidence
Recent reviews (2023-2026) have highlighted:
- Cannabidiol treatment for SWS-related epilepsy - 2024 review (PMID: 39598668) covers molecular pathways and CBD data
- Overview of history, genetics, and management (2024) - Ramirez & Julich, Seminars in Pediatric Neurology (PMID: 39389653)
- Systematic review of headache in SWS - 2024, Cephalalgia (PMID: 39043228) - headache is an under-recognized feature
- Biomarker development - 2025 review on emerging biomarkers (PMID: 40851064)
Summary Table
| Feature | Detail |
|---|---|
| Synonym | Encephalotrigeminal angiomatosis |
| Type | Sporadic phacomatosis (neurocutaneous syndrome) |
| Mutation | Somatic GNAQ (chr 9q21.2) |
| Incidence | ~1:20,000 |
| Skin | Port-wine stain (forehead/V1 distribution) |
| Brain | Leptomeningeal parieto-occipital angioma |
| Eye | Glaucoma, choroidal hemangioma |
| Pathophysiology | Abnormal venous drainage → ischemia → atrophy + calcification |
| Classic radiology sign | "Tram-track" cortical calcification |
| MRI finding | Pial enhancement + hemispheric atrophy + enlarged choroid plexus |
| Seizures | 72-93% of patients; onset usually <2 years |
| Treatment | AEDs, hemispherectomy for refractory cases, low-dose aspirin prophylaxis, pulsed-dye laser for PWS, glaucoma screening |
Sources: Bradley & Daroff's Neurology in Clinical Practice; Goldman-Cecil Medicine; Grainger & Allison's Diagnostic Radiology; Andrews' Diseases of the Skin; Kanski's Clinical Ophthalmology; Dermatology 2-Vol Set 5e
Pathology of it
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
I now have all the key pathology content from multiple authoritative sources. Let me compile the full answer:
Pathology of Sturge-Weber Syndrome
1. Molecular Pathogenesis
The fundamental molecular defect is a somatic (post-zygotic mosaic) gain-of-function mutation in GNAQ (chromosome 9q21.2), found in ~90% of affected individuals. The same mutation occurs in the port-wine stain and the leptomeningeal angioma.
What GNAQ does normally:
- Encodes the alpha subunit of a heterotrimeric G-protein (Gq class)
- Acts as a molecular switch - transmits signals from G protein-coupled receptors to downstream effectors
- Has intrinsic GTPase activity that "turns itself off"
Effect of the mutation:
- Most common substitution is at the R183 residue
- Reduces GTPase activity → the G-protein remains constitutively "stuck ON"
- Results in persistent activation of MAPK (mitogen-activated protein kinase) signaling → increased cell proliferation, decreased apoptosis
- Also activates ERK (extracellular signal-regulated kinase)
Why mosaic?
- A germline GNAQ mutation would be lethal; the mutation survives only because it occurs after fertilization in a subset of cells
- The mutation is present only in affected tissues (skin, meningeal endothelium) - NOT detectable in blood
Related mutations (same pathway):
- GNA11 (related G-protein α subunit) - also implicated in SWS and in blue nevi, nevus of Ota, uveal melanoma
- RASA1 and EPHB4 mutations - cause capillary malformation-AVM syndrome (different disease)
- Facial CM is thought to arise from clonal expansion of abnormal cells originating from the neural crest
2. Developmental / Embryological Basis
The leptomeningeal and facial vascular malformations share the same embryological origin:
- During the 6th fetal week, a primitive vascular plexus forms around the cephalic neural tube and the region destined to become facial skin
- Normally, this plexus regresses during the 9th fetal week
- In SWS, the GNAQ mutation leads to failure of regression of this plexus
- There is a close anatomical correlation between the embryonic vascular plexus of the eyelid/forehead and that of the occipitoparietal brain - which explains why upper eyelid involvement predicts intracranial lesions
3. Gross / Macroscopic Pathology
Skin - Port-Wine Stain (Capillary Malformation)
- A vascular birthmark composed of a permanent collection of dilated postcapillary venules in the dermis
- Present at birth as a flat, pink-to-red lesion
- With age: darkens, thickens, develops a cobblestoned surface (two-thirds of affected adults)
- May develop nodular elevations and pyogenic granulomas
- Reactive hypertrophy of adjacent connective tissue and bone can produce facial asymmetry and skeletal deformity (resembling Klippel-Trenaunay-Weber)
- The port-wine stain is not a true neoplasm - it is a vascular ectasia (permanent dilation of preexisting small vessels)
Brain - Leptomeningeal Angioma
- Ipsilateral venous angioma of the cortical leptomeninges, predominantly parieto-occipital
- The angioma consists largely of abnormal veins, not arteries - easily distinguished from true AVM
- Overlying leptomeninges show diffuse vascular engorgement with tortuous, thin-walled venous channels
- The underlying cerebral cortex is progressively destroyed: it is replaced by glial tissue that subsequently calcifies
- Enlarged choroid plexus on the ipsilateral side
- Cortical atrophy (hemiatrophy in advanced cases) - progressive and ipsilateral
- In "burnt out" cases: only a chronically shrunken, calcified hemisphere remains with no enhancing angioma
Calcification - the Hallmark
- Calcium is deposited in the 2nd and 3rd layers of the cerebral cortex (Wohlwill and Yakovlev's classic finding - established by Krabbe who corrected the earlier belief that it was in blood vessels)
- The calcification follows the gyral convolutions of the parietooccipital cortex
- Produces the classic "tram-track" (double-contoured, tramline) pattern on plain X-ray and CT
4. Microscopic (Histological) Pathology
Port-Wine Stain (Skin)
- Dilated postcapillary venules within the papillary and upper reticular dermis
- Also areas of increased number of normal-looking capillaries
- Endothelial cells are flat (not proliferating - distinguishing it from a true hemangioma)
- Factor VIII, fibronectin, and basement membrane proteins are normal
- S100 staining shows abnormal innervation - reduced sympathetic innervation of the papillary vascular plexus
- The vessel ectasia (progressive widening without proliferation) is believed to result from abnormal neural (sympathetic) modulation of the papillary plexus
- Waner Classification (grades I-IV) correlates degree of vessel ectasia with degree of sympathetic denervation
Leptomeningeal Angioma (Brain)
- Thin-walled venous channels in the leptomeninges
- Sparse superficial cortical veins with enlarged, tortuous subependymal and medullary veins acting as collaterals
- Cortex below the angioma shows: neuronal loss, gliosis, and intracortical calcification in layers II and III
- Microscopic hemorrhages may be present (though significant intracranial hemorrhage is rare)
- Evidence of chronic ischemia: the leptomeningeal angioma "steals" blood from the cortex, leading to progressive neuronal loss
- Polymicrogyria is occasionally seen in SWS
5. Pathophysiological Cascade (How the Lesion Progresses)
GNAQ somatic mutation
↓
Failure of regression of embryonal vascular plexus
↓
Leptomeningeal venous angioma (abnormal draining veins)
↓
Impaired cortical venous drainage → chronic venous hypertension
↓
Chronic cortical ischemia + hypoxia
↓
Neuronal loss → Gliosis → Cortical atrophy
↓
Calcium deposition in layers II and III of cortex
↓
Epilepsy → further ischemia (vascular "steal" during seizures)
↓
Progressive hemiparesis, hemianopia, intellectual disability
Two mechanisms have been proposed for progressive cortical damage:
- Vascular steal: blood is diverted to the meninges during seizures → progressive ischemia of the cerebral cortex beneath
- Seizures themselves are responsible for progressive deficits independent of ischemia
6. Ocular Pathology
- Glaucoma: episcleral vascular malformation increases episcleral venous pressure → impairs aqueous humor outflow through Schlemm's canal → raised IOP. Blood in the Schlemm canal on gonioscopy is a characteristic finding
- Buphthalmos: infantile glaucoma causes ocular enlargement before closure of growth plates in the sclera
- Choroidal hemangioma: diffuse, flat, orange-red choroidal hemangioma (capillary-venous malformation) - can cause exudative retinal detachment and vision loss
Imaging Correlation of Pathology
| Pathological Feature | Radiological Correlate |
|---|---|
| Cortical calcification (layers II-III) | Tram-track hyperdensity on CT |
| Leptomeningeal angioma | Diffuse pial/leptomeningeal enhancement on gadolinium MRI |
| Cortical atrophy | Hemispheric volume loss, sulcal widening on MRI |
| Enlarged choroid plexus | Ipsilateral choroid plexus enlargement on MRI |
| Abnormal deep veins | Prominent medullary/subependymal veins on T2/SWI |
| Polymicrogyria | Abnormal gyral pattern on MRI |
| Choroidal hemangioma | Enhancing bilateral choroidal lesions on post-contrast MRI |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Adams & Victor's Principles of Neurology 12th ed.; Fitzpatrick's Dermatology; Dermatology 2-Vol Set 5e; Bradley & Daroff's Neurology in Clinical Practice; Grainger & Allison's Diagnostic Radiology; Scott-Brown's Otorhinolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.