Latest management guidelines of hypertension
Reading File
Finding Sources
Searching PubMed
"hypertension" AND "guidelines"
Searching the Web
hypertension management guidelines 2024 2025 ACC AHA ESC
Finding Sources
Reading Article
Reading Article
Reading Web Page
hypertension management guidelines BP targets drug treatment lifestyle 2025
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
I have comprehensive information to provide a thorough, up-to-date answer. Let me compile everything now.
Latest Guidelines for the Management of Hypertension
Two major guidelines now frame contemporary hypertension management: the 2025 AHA/ACC/Multisociety Guideline (Jones DW et al., JACC / Hypertension, Aug 2025 — PMID 40811516) and the 2024 ESC Guidelines (McEvoy JW et al., Eur Heart J, Oct 2024 — PMID 39210715).
1. Classification & Diagnostic Thresholds
| Category | AHA/ACC 2025 | ESC 2024 |
|---|---|---|
| Normal BP | <120/<80 mmHg | <120/<70 mmHg |
| Elevated BP | 120–129 / <80 | 120–129 / 70–79 |
| Hypertension threshold | ≥130/≥80 | ≥140/≥90 |
| Stage 1 HTN | 130–139 / 80–89 | 140–159 / 90–99 (Grade 1) |
| Stage 2 HTN | ≥140/≥90 | 160–179 / 100–109 (Grade 2) |
| Severe HTN | — | ≥180/≥110 (Grade 3) |
The AHA/ACC's lower 130/80 threshold means many individuals classified as Stage 1 in the U.S. are considered "high-normal BP" or "elevated BP" by ESC criteria — an important transatlantic distinction.
2. BP Measurement
- Office BP: ≥2 readings, ≥2 occasions; automated oscillometric preferred
- Out-of-office confirmation: Ambulatory BP monitoring (ABPM) or home BP monitoring (HBPM) strongly recommended to exclude white coat hypertension and detect masked hypertension
- ABPM daytime average ≥130/80 (AHA/ACC) or ≥135/85 (ESC) = hypertension
3. BP Treatment Targets
| Population | AHA/ACC 2025 | ESC 2024 |
|---|---|---|
| Most adults | <130/80 mmHg | <130/80 mmHg (if tolerated) |
| Aged 65–79 | <130/80 | <130/80 (SBP target 120–129 if tolerated) |
| Aged ≥80 | Individualized; avoid <130 | SBP 130–139; consider ≥140 if frail |
| Diabetes | <130/80 | <130/80 |
| CKD | <130/80 | <130/80 |
| Established CVD | <130/80 | <130/80 |
| Stroke/TIA | <130/80 | <130/80 |
| Cognitive protection | <130 SBP (new in 2025) | — |
4. When to Start Pharmacotherapy
AHA/ACC 2025:
- BP ≥140/90 mmHg: Start medications immediately in all adults, regardless of CVD risk
- BP 130–139/80–89 + high CVD risk (PREVENT score ≥7.5%, diabetes, CKD, established CVD): Start medications immediately
- BP 130–139/80–89 + low CVD risk (PREVENT <7.5%): 3–6 months lifestyle modification trial → start medications if BP remains elevated
ESC 2024:
- BP ≥140/90 mmHg: Start medications in all adults <85 years regardless of risk
- BP 130–139/80–89 + high risk (CVD, diabetes, CKD, organ damage, SCORE2 ≥10%): Start medications
- BP 130–139/80–89 + low-moderate risk: Lifestyle intervention first; defer pharmacotherapy
The 2025 AHA/ACC replaces the Pooled Cohort Equation with the PREVENT™ model for 10-year CVD risk estimation.
5. Lifestyle Modifications (Both Guidelines — Class I)
Lifestyle changes can reduce SBP by 7–15 mmHg and are foundational at every stage:
| Intervention | Expected SBP Reduction |
|---|---|
| DASH/Mediterranean diet | ~6–11 mmHg |
| Sodium restriction (<1500 mg/day) | ~5–6 mmHg |
| Weight loss (per 5 kg) | ~4–5 mmHg |
| Aerobic exercise (90–150 min/week) | ~4–8 mmHg |
| Dynamic resistance training | ~4 mmHg |
| Alcohol reduction (≤2 drinks/day ♂, ≤1 ♀) | ~3–4 mmHg |
| Smoking cessation | Cardiovascular risk ↓ |
— Goldman-Cecil Medicine, 26th Ed.; Comprehensive Clinical Nephrology, 7th Ed.
6. Pharmacotherapy — First-Line Drug Classes
Both guidelines align on the same preferred classes:
- ACE inhibitors (ACEi) or Angiotensin Receptor Blockers (ARBs) — RAS blockade as the foundation
- Calcium Channel Blockers (CCBs) — dihydropyridines preferred (e.g., amlodipine)
- Thiazide/thiazide-like diuretics — chlorthalidone preferred in the U.S.; indapamide preferred in Europe
β-blockers are NOT first-line for uncomplicated hypertension but are used when there is a specific indication: heart failure with reduced EF, angina, post-MI, atrial fibrillation, or in younger pregnant women.
7. Treatment Algorithm (Stepped Approach)
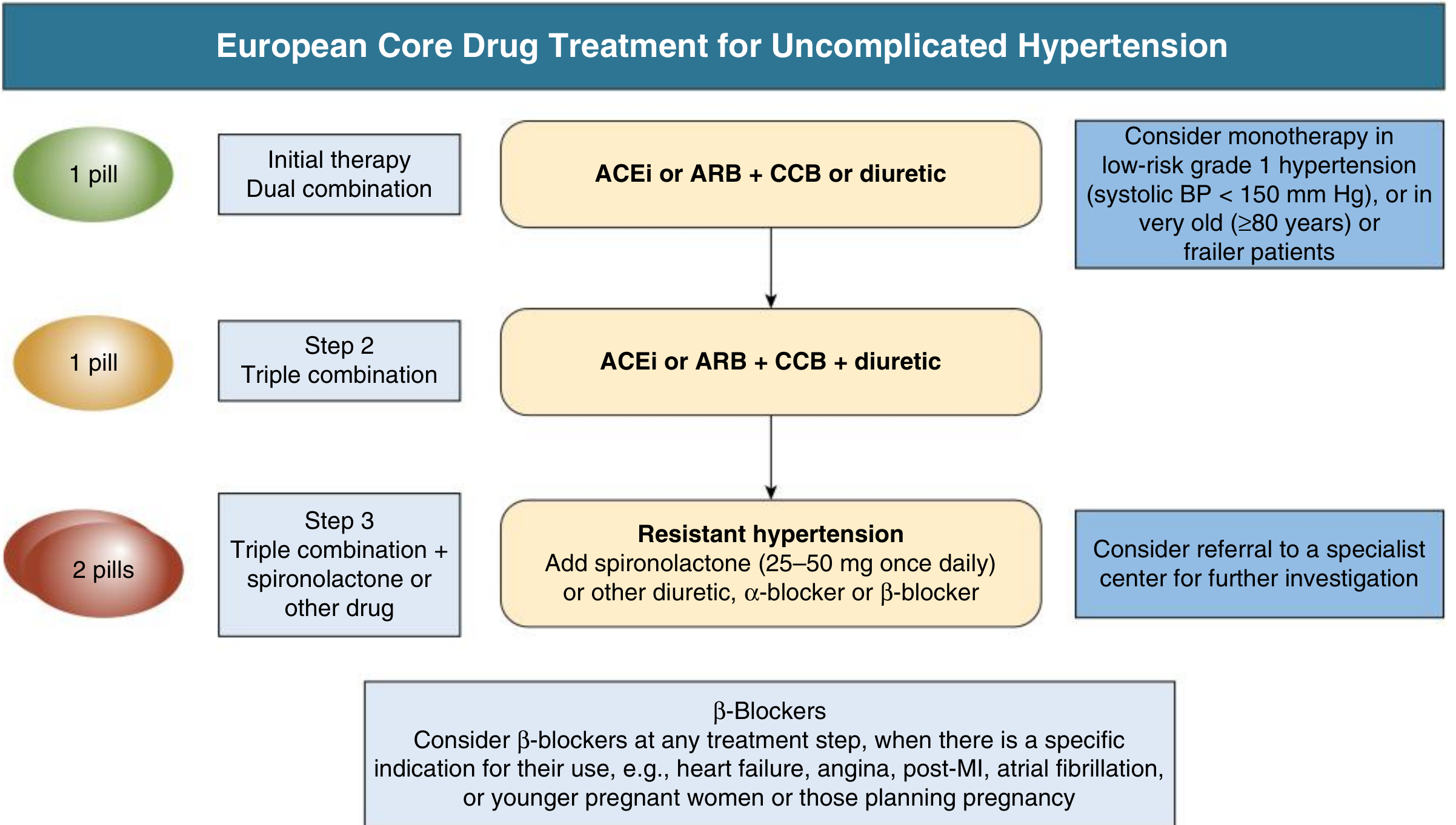
Step 1 — Initial therapy (dual combination as 1 pill):
- ACEi or ARB + CCB or thiazide-like diuretic
- Monotherapy only for: frail elderly, low-risk Grade 1 HTN with SBP <150 mmHg
Step 2 — Triple combination (as 1 pill):
- ACEi or ARB + CCB + thiazide-like diuretic
Step 3 — Resistant hypertension:
- Add spironolactone 25–50 mg/day (MRA, most evidence from PATHWAY-2 trial)
- Alternatively: another diuretic (amiloride, eplerenone), α-blocker, or β-blocker
- Refer to specialist
Single-pill combination (SPC) strategy is strongly advocated by ESC to reduce pill burden and improve adherence — the primary driver of poor BP control globally. — Comprehensive Clinical Nephrology, 7th Ed., p.531
8. Resistant Hypertension
Defined as: BP ≥130/80 (AHA/ACC) or ≥140/90 (ESC) despite ≥3 antihypertensive agents at optimal doses (including a diuretic).
Before diagnosing true resistance, exclude pseudo-resistance:
- Poor medication adherence
- White coat hypertension (confirm with ABPM)
- Incorrect cuff size
- Therapeutic inertia
Common secondary causes to screen:
| Cause | Notes |
|---|---|
| Primary aldosteronism | Most common; always screen with ARR |
| Obstructive sleep apnea | Very common; treat with CPAP |
| Renovascular disease | Atherosclerotic or FMD |
| CKD | Sodium retention |
| Pheochromocytoma | Rare but dangerous |
| Cushing syndrome | Check if stigmata present |
| Aortic coarctation | Consider in young patients |
Drug interactions raising BP: NSAIDs, oral contraceptives, sympathomimetics (decongestants), cyclosporine, corticosteroids, cocaine/amphetamines.
9. Special Populations
| Population | Key Recommendations |
|---|---|
| Diabetes | Target <130/80; ACEi/ARB first-line (renoprotective); SGLT2i reduce BP + CV/renal outcomes |
| CKD (non-proteinuric) | Target <130/80; ACEi/ARB first-line if proteinuria |
| CKD (proteinuria ≥300 mg/day) | ACEi or ARB mandatory; avoid ACEi + ARB combination |
| Heart failure (HFrEF) | ACEi/ARB/ARNi + β-blocker + MRA + SGLT2i (GDMT) |
| Post-MI / Stable CAD | ACEi/ARB + β-blocker; target <130/80 |
| Atrial fibrillation | Rate control with β-blocker; ACEi/ARB to reduce recurrence |
| Stroke/TIA | Restart antihypertensives after acute phase; target <130/80 |
| Elderly ≥65 years | Start low, go slow; avoid orthostatic hypotension; SPC improves adherence |
| Pregnancy | Labetalol, methyldopa, nifedipine (extended-release); ACEi/ARB contraindicated |
| Black patients | CCBs and thiazide-like diuretics more effective; ACEi monotherapy less effective |
10. Hypertensive Urgency & Emergency
| Condition | Definition | Management |
|---|---|---|
| Hypertensive urgency | SBP >180 or DBP >120, no acute organ damage | Oral agents; reduce BP gradually over 24–48h |
| Hypertensive emergency | Severe HTN + acute end-organ damage (encephalopathy, AKI, ACS, aortic dissection, pulmonary edema, retinopathy) | ICU; IV agents (nicardipine, labetalol, nitroprusside, clevidipine); reduce MAP by ≤25% in first hour |
11. Follow-up & Monitoring
- Re-evaluate at 1 month after initiating or adjusting therapy
- Once at target: every 3–6 months
- Annual labs: BMP (electrolytes, creatinine, eGFR), urine albumin-to-creatinine ratio
- ECG if LVH suspected
- Address cardiovascular risk factors holistically (statin, aspirin in select cases)
Key Differences: 2025 AHA/ACC vs. 2024 ESC at a Glance
| Feature | AHA/ACC 2025 | ESC 2024 |
|---|---|---|
| Diagnostic threshold | ≥130/80 | ≥140/90 |
| Risk calculator | PREVENT™ | SCORE2/SCORE2-OP |
| Initial therapy | Dual combination preferred | Dual SPC strongly preferred |
| BP target (most adults) | <130/80 | <130/80 |
| Resistant HTN threshold | ≥130/80 on ≥3 drugs | ≥140/90 on ≥3 drugs |
| Living guideline format | Yes (updated periodically) | No |
Sources:
This is a shared conversation. Sign in to Orris to start your own chat.