Types of Emphysema and Bronchitis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have everything needed for a thorough, well-illustrated answer. Here is the complete response:
Emphysema and Bronchitis
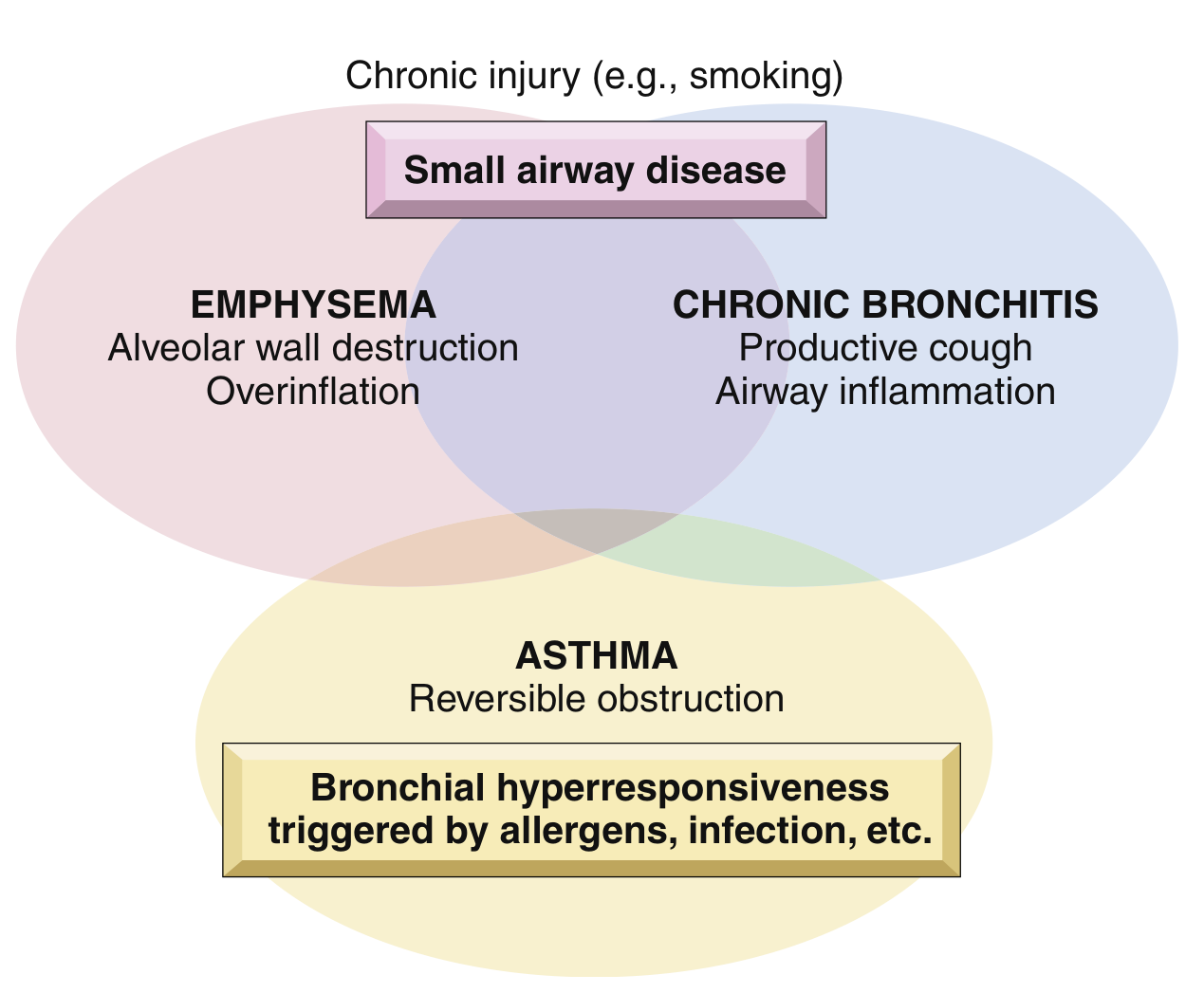
Overview - Overlap in COPD
These two conditions, along with asthma, form the spectrum of chronic obstructive lung disease, often coexisting in the same patient. They share a common trigger - chronic injury, especially cigarette smoking - but differ in their anatomic basis:
EMPHYSEMA
Definition: Permanent, irreversible enlargement of airspaces distal to the terminal bronchiole, accompanied by destruction of alveolar walls, without significant fibrosis. Unlike chronic bronchitis, emphysema is defined anatomically, not clinically.
The lung unit of reference is the acinus (the structure distal to terminal bronchioles, comprising respiratory bronchioles, alveolar ducts, and alveoli). A cluster of 3-5 acini forms a lobule.
Four Types of Emphysema
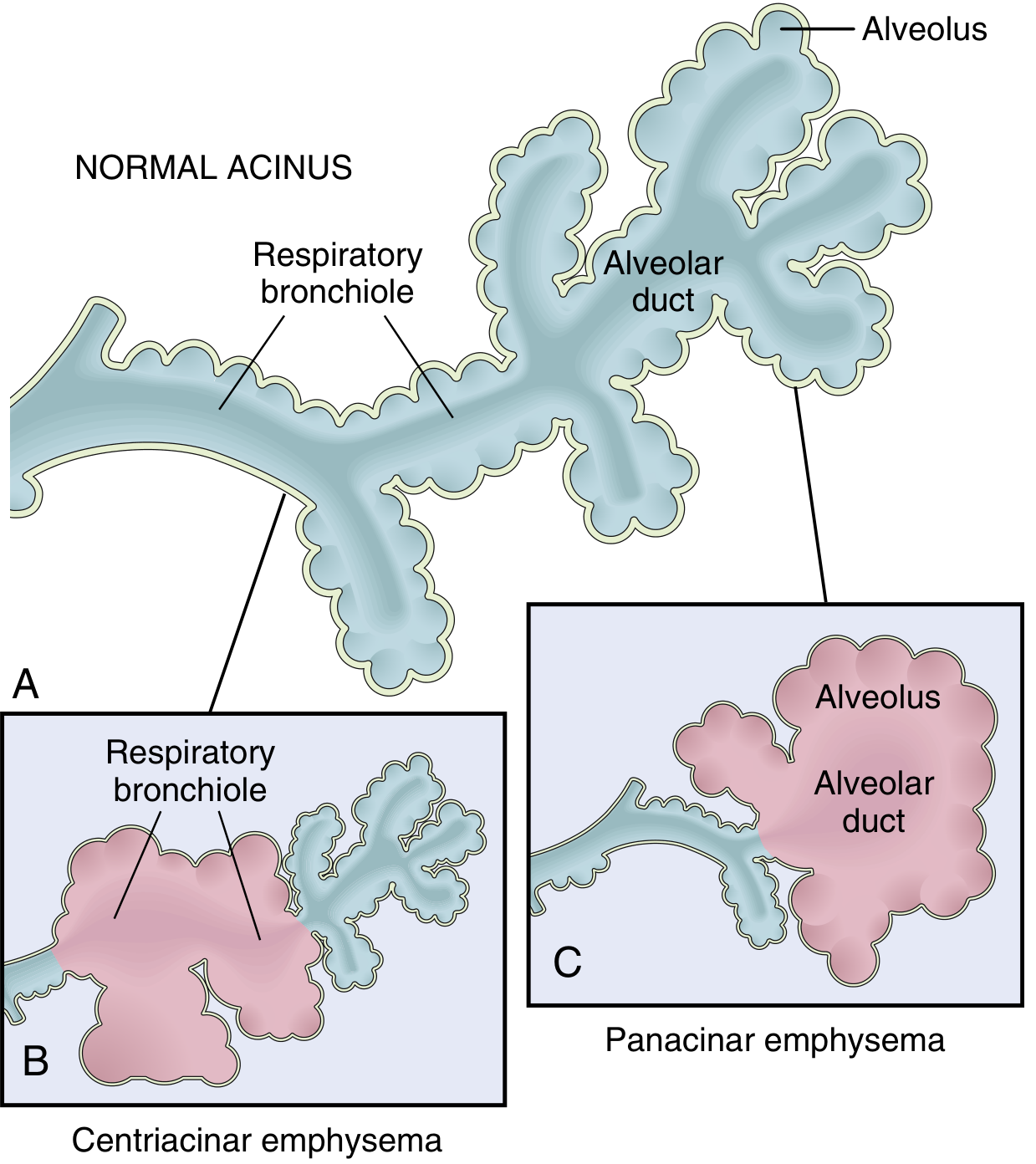
1. Centriacinar (Centrilobular) Emphysema
- Most common type - constitutes >95% of clinically significant cases
- The central/proximal parts of the acinus (respiratory bronchioles) are destroyed; distal alveoli are spared
- Both emphysematous and normal airspaces coexist within the same acinus
- Distribution: upper lobes, especially apical segments
- Association: heavy cigarette smokers; commonly accompanied by chronic bronchitis
- In advanced disease, distal acinus also becomes involved, making it difficult to distinguish from panacinar emphysema
2. Panacinar (Panlobular) Emphysema
- Acini are uniformly enlarged from the respiratory bronchiole all the way to the terminal blind alveoli - the entire acinus is affected
- Distribution: lower lung zones and anterior lung margins; worst at the bases
- Association: alpha-1 antitrypsin (α1-AT) deficiency - exacerbated by smoking
- Less common than centriacinar emphysema
3. Distal Acinar (Paraseptal) Emphysema
- The proximal acinus is normal; the distal part (alveolar ducts and alveolar sacs) is predominantly involved
- Located near the pleura, along lobular connective tissue septa, and at margins of lobules adjacent to areas of fibrosis or atelectasis
- More severe in the upper half of the lungs
- Characteristically forms enlarged air spaces (0.5 mm to >2 cm), sometimes progressing to bullae
- Cause unknown; comes to attention most often in young adults who present with spontaneous pneumothorax
4. Irregular Emphysema
- Acinus is irregularly involved, almost invariably associated with scarring (e.g., post-inflammatory or post-traumatic fibrosis)
- Clinically the least significant type - generally asymptomatic
- The most common form found at autopsy when carefully examined
Key point: Only centriacinar and panacinar emphysema cause clinically significant airflow obstruction and are associated with COPD.
Histopathology of Emphysema

Marked enlargement of airspaces, destruction of alveolar septa without significant fibrosis, with anthracotic pigment often visible.
Pathogenesis of Emphysema
The key mechanism is an imbalance between proteases and antiproteases in the lung:
- Cigarette smoke recruits neutrophils and macrophages into the lung, which release elastase and other proteases
- These degrade the elastin matrix of alveolar walls
- Normally, α1-antitrypsin (produced by the liver) inhibits elastase - when α1-AT is deficient (or inactivated by smoking), unchecked protease activity destroys alveolar walls
- Oxidative stress from smoking also directly damages lung tissue and inactivates antiproteases
BRONCHITIS
Types
Acute Bronchitis
- Acute inflammation of the bronchi, usually due to viral infection (rhinovirus, adenovirus, influenza)
- Self-limiting; presents with cough, mucoid sputum, low-grade fever
- Resolves in 1-3 weeks; not associated with COPD
- Antibiotics are generally not indicated unless secondary bacterial infection is confirmed
Chronic Bronchitis
- Defined clinically (not anatomically): persistent productive cough for at least 3 consecutive months in at least 2 consecutive years, in the absence of any other identifiable cause
- Common in cigarette smokers and urban dwellers in heavily polluted cities
Pathogenesis
Three main processes drive chronic bronchitis:
-
Mucus hypersecretion - the earliest and most characteristic feature
- Enlargement of submucosal mucous glands in trachea and large bronchi
- Increase in goblet cells in small airways
- Driven by inflammatory mediators (histamine, IL-13) and acquired CFTR dysfunction from smoking (producing dehydrated, abnormal mucus)
-
Inflammation - neutrophils, lymphocytes, and macrophages infiltrate the airways; eosinophils are NOT seen (unlike asthma)
-
Infection - does not initiate chronic bronchitis, but maintains it and triggers acute exacerbations
Morphology
- Hyperemia, swelling, and edema of bronchial mucosa
- Heavy mucinous or mucopurulent secretions filling bronchi
- Enlargement of submucosal mucous glands - the hallmark finding
- Reid index (ratio of mucous gland thickness to bronchial wall thickness between epithelium and cartilage) is normally ≤0.4; elevated in chronic bronchitis, proportional to disease severity
- Goblet cell hyperplasia, smooth muscle hypertrophy, peribronchial fibrosis
- In severe cases: bronchiolitis obliterans (complete obliteration of bronchiolar lumen by fibrosis)
Consequences
- Small airway disease (chronic bronchiolitis) is the primary cause of airflow obstruction - NOT the large-airway mucus hypersecretion
- Progressive: can lead to hypoxemia, pulmonary hypertension, and cor pulmonale
- Some patients with chronic bronchitis develop asthmatic bronchitis (with bronchospasm and wheezing due to airway hyperresponsiveness)
- Chronic bronchitis frequently coexists with centriacinar emphysema in heavy smokers
Comparison Summary
| Feature | Centriacinar Emphysema | Panacinar Emphysema | Paraseptal Emphysema | Chronic Bronchitis |
|---|---|---|---|---|
| Definition | Anatomic | Anatomic | Anatomic | Clinical |
| Part involved | Respiratory bronchioles (proximal acinus) | Entire acinus | Distal acinus | Large + small airways |
| Location | Upper lobes | Lower lobes / bases | Near pleura, upper lung | Diffuse |
| Cause | Smoking | α1-AT deficiency | Unknown | Smoking / pollutants |
| COPD significance | Yes (most common) | Yes | No | Yes |
| Key complication | Airflow obstruction | Airflow obstruction | Spontaneous pneumothorax / bullae | Cor pulmonale |
| Hallmark finding | Destruction of respiratory bronchioles | Uniform acinar enlargement | Bullae formation | Elevated Reid index |
Sources: Robbins & Kumar Basic Pathology (Robbins Pathology), p. 448-451; Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 634-638
This is a shared conversation. Sign in to Orris to start your own chat.