Hypertensive disorders in detail using this outline Classifications and definitions Etiology and pathophysiology Risk factors Diagnostic work up Management and action plan Complications And any other important component of the subject matter
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypertensive disorders" AND "pregnancy" AND "classification"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Hypertensive Disorders of Pregnancy (HDP)
1. Classifications and Definitions
Hypertensive disorders affect 5-15% of all pregnancies and are a leading cause of maternal and perinatal morbidity and mortality worldwide. The ACOG classification (Practice Bulletin No. 222, 2020) recognizes the following categories:
A. Gestational Hypertension
- New-onset BP ≥140/90 mmHg after 20 weeks' gestation in a previously normotensive woman
- No proteinuria and no end-organ damage
- Severe range: SBP ≥160 or DBP ≥110 mmHg (confirmed within minutes)
- Resolves by 12 weeks postpartum; if it persists, reclassified as chronic hypertension
- Occurs in 6-17% of nulliparous and 2-4% of parous patients
B. Preeclampsia
- Gestational hypertension (BP ≥140/90 mmHg after 20 weeks) PLUS:
- Proteinuria: >300 mg/24h, protein:creatinine ratio ≥0.3, or dipstick 2+; OR
- New-onset end-organ damage, any one of the following:
- Thrombocytopenia: platelets <100 × 10⁹/L
- Renal insufficiency: creatinine >1.1 mg/dL or doubling from baseline
- Impaired liver function: transaminases ≥2× upper limit of normal
- Pulmonary edema
- New-onset headache unresponsive to analgesics
- Visual disturbances
Sub-classifications:
- Without severe features - BP 140-159/90-109 mmHg, no end-organ criteria above
- With severe features - any of the criteria listed in the table below
- Early-onset (<34 weeks) vs. Late-onset (≥34 weeks) - early-onset carries the highest morbidity
Severe Features of Preeclampsia (ACOG):
| Feature | Threshold |
|---|---|
| Severe hypertension | SBP ≥160 or DBP ≥110 mmHg on 2 occasions ≥4h apart |
| Thrombocytopenia | Platelets <100,000/µL |
| Elevated liver enzymes | >2× upper limit of normal |
| Severe RUQ/epigastric pain | Unresponsive to medications |
| Renal insufficiency | Creatinine >1.1 mg/dL or doubling of baseline |
| Pulmonary edema | New onset |
| Neurologic symptoms | New headache, visual disturbances |
C. Eclampsia
- Preeclampsia PLUS new-onset generalized tonic-clonic, focal, or multifocal seizures not attributable to another condition (epilepsy, intracranial hemorrhage, drug use)
- Incidence in high-resource settings: 1 in 2,000-3,000 deliveries
- Often preceded by headache, visual disturbances, or epigastric pain
D. Chronic Hypertension
- Hypertension present before 20 weeks' gestation, or diagnosed before pregnancy, or failing to resolve by 12 weeks postpartum
- May be primary (essential) or secondary
E. Chronic Hypertension with Superimposed Preeclampsia
- New-onset proteinuria or new/worsening end-organ damage in a woman with known chronic hypertension
- Carries higher morbidity than either condition alone
F. White Coat Hypertension
- Elevated BP in clinical settings only (typically before 20 weeks)
- Requires ambulatory BP monitoring to confirm
- May progress to gestational hypertension
G. HELLP Syndrome
- A severe subtype/variant of preeclampsia characterized by:
- Hemolysis (microangiopathic hemolytic anemia)
- Elevated Liver enzymes
- Low Platelet count
- Occurs in 10-20% of women with severe preeclampsia and 0.2-0.9% of all pregnancies
- Mortality rate: 7.4-34%
- 20% of cases occur before 28 weeks; 30% occur postpartum
2. Etiology and Pathophysiology
The precise mechanisms are not fully understood. Current evidence supports a two-stage model:
Stage 1 - Abnormal Placentation (Silent Phase)
- In normal pregnancy, extravillous trophoblasts invade the spiral arteries, transforming them from narrow, high-resistance vessels into wide, low-resistance channels - maximizing uteroplacental perfusion
- In preeclampsia, this endovascular trophoblastic remodeling is deficient, resulting in:
- Shallow trophoblast invasion
- Persistence of high-resistance spiral arteries
- Chronic uteroplacental ischemia and hypoxia
- Genetic, immunologic (inadequate maternal tolerance of paternal antigens), and inflammatory mechanisms contribute
Stage 2 - Systemic Endothelial Dysfunction (Clinical Phase)
- The ischemic placenta releases factors into maternal circulation:
Anti-angiogenic excess:
- sFlt-1 (soluble fms-like tyrosine kinase 1) - a decoy receptor that sequesters VEGF and PlGF, causing widespread endothelial dysfunction
- Soluble endoglin (sEng) - antagonizes TGF-β signaling, further impairing endothelial function
- Decreased PlGF (placental growth factor) - an angiogenic factor
A ratio of sFlt-1/PlGF ≥40 is associated with increased risk of developing preeclampsia with severe features within 2 weeks of measurement.
Consequences of endothelial dysfunction:
- Increased systemic vascular resistance → hypertension
- Increased capillary permeability → proteinuria, edema
- Hemoconcentration (hallmark - NOT hypervolemia; volume expansion is hazardous)
- Increased afterload → cardiac compromise
- Platelet activation and consumption → thrombocytopenia
- Microangiopathic hemolysis → HELLP
- Cerebral dysautoregulation → seizure risk (eclampsia can occur at even modestly elevated BP)
- Hepatocellular ischemia → elevated liver enzymes, subcapsular hematoma
Exaggerated maternal inflammatory response also plays a key role, with elevated CRP, IL-1Ra, and IL-6 levels - especially pronounced in HELLP syndrome.
3. Risk Factors
Risk factors with pooled relative risks (from Brenner & Rector's The Kidney):
| Risk Factor | Pooled Relative Risk (95% CI) |
|---|---|
| Prior preeclampsia | 8.4 (7.1-9.9) |
| Previous acute kidney injury | 5.9 (3.6-9.7) |
| Chronic hypertension | 5.1 (4.0-6.5) |
| Pregestational diabetes mellitus | 3.7 (3.1-4.3) |
| Strong family CVD history (≥2 first-degree relatives) | 3.2 (1.4-7.7) |
| Multiple gestations | 2.9 (2.6-3.1) |
| Antiphospholipid antibody syndrome | 2.8 (1.8-4.3) |
| Obesity (pre-pregnancy BMI >30) | 2.8 (2.6-3.1) |
| Nulliparity | 2.1 (1.9-2.4) |
| Family history of preeclampsia | 2.4 (1.8-3.6) |
| Systemic lupus erythematosus | 2.5 (1.0-6.3) |
| Assisted reproductive technology (esp. oocyte donation) | 1.8 (1.6-2.1) |
| Chronic kidney disease | 1.8 (1.5-2.1) |
| Excessive gestational weight gain (>35 lbs) | 1.9 (1.7-2.0) |
| Advanced maternal age (>40 years) | 1.5 (1.2-2.0) |
Additional risk factors: trisomy 13, hydatidiform mole, low birth weight of the mother herself (born small), African American ethnicity (non-Hispanic Black women have disproportionately higher rates), teen pregnancy (controversial), socioeconomic disadvantage.
High-risk factors per ACOG (any one = start low-dose aspirin prophylaxis): chronic hypertension, prior preeclampsia, multifetal gestation, diabetes mellitus, renal disease, autoimmune disease, preterm birth <34 weeks.
4. Diagnostic Workup
Blood Pressure Measurement
- Use validated device; patient seated, arm at heart level, after 5 minutes rest
- Two readings ≥4 hours apart for non-severe range; can confirm within minutes for severe range (≥160/110)
Urinalysis and Proteinuria
- 24-hour urine protein: ≥300 mg diagnostic; quantification after initial diagnosis is not required to follow severity
- Spot protein:creatinine ratio: ≥0.3 is equivalent to 24h urine >300 mg
- Urine dipstick 2+ is acceptable if other methods unavailable
Laboratory Panel (Preeclampsia Workup)
| Test | Rationale |
|---|---|
| CBC with platelets | Thrombocytopenia (<100,000/µL) = severe feature |
| Serum creatinine | Renal insufficiency (>1.1 mg/dL) |
| Liver enzymes (AST/ALT) | ≥2× ULN = severe feature |
| LDH | Elevated in HELLP/hemolysis |
| Peripheral blood smear | Schistocytes in HELLP/microangiopathy |
| Uric acid | Often elevated; not diagnostic but supportive |
| Serum albumin | Assesses third-spacing |
| Coagulation studies (PT, aPTT, fibrinogen) | DIC screen in severe disease |
Fetal Assessment
- Ultrasound - fetal growth (for IUGR), amniotic fluid index
- Non-stress test (NST) - fetal well-being
- Biophysical profile (BPP) - twice weekly in severe disease
- Umbilical artery Doppler - reversed end-diastolic flow = urgent delivery consideration
Neuroimaging (Eclampsia)
- CT head - urgently if intracranial hemorrhage suspected
- MRI - posterior reversible encephalopathy syndrome (PRES): classically shows T2/FLAIR hyperintensities in occipital and parietal regions
Angiogenic Biomarkers (Emerging)
- sFlt-1/PlGF ratio ≥40 predicts preeclampsia with severe features within 2 weeks; being integrated into clinical protocols in many centers
HELLP Diagnosis (Tennessee Classification by Sibai)
- Class 1: platelets ≤50,000/µL
- Class 2: platelets 50,000-100,000/µL
- Class 3: platelets 100,000-150,000/µL (partial HELLP)
- LDH >600 IU/L, AST ≥70 IU/L, platelets <100,000/µL
5. Management and Action Plan
General Principles
- Delivery is the only definitive cure - timing balances maternal safety vs. fetal maturity
- Prevent seizures with magnesium sulfate
- Control severe hypertension within 30-60 minutes of sustained severe-range values
- Careful fluid management (hemoconcentration is the rule; over-hydration causes pulmonary edema)
A. Preeclampsia WITHOUT Severe Features
Delivery timing: At 37 weeks (or sooner if maternal/fetal deterioration)
Expectant management (up to 37 weeks):
- Inpatient or close outpatient monitoring
- BP checks twice weekly
- CBC, liver enzymes, creatinine weekly
- Daily fetal kick counts; NST twice weekly
- BPP as clinically indicated
- Restrict physical activity
Antihypertensives: Generally not needed (BP <160/110); initiate if BP approaches severe range
B. Preeclampsia WITH Severe Features
Delivery timing by gestational age:
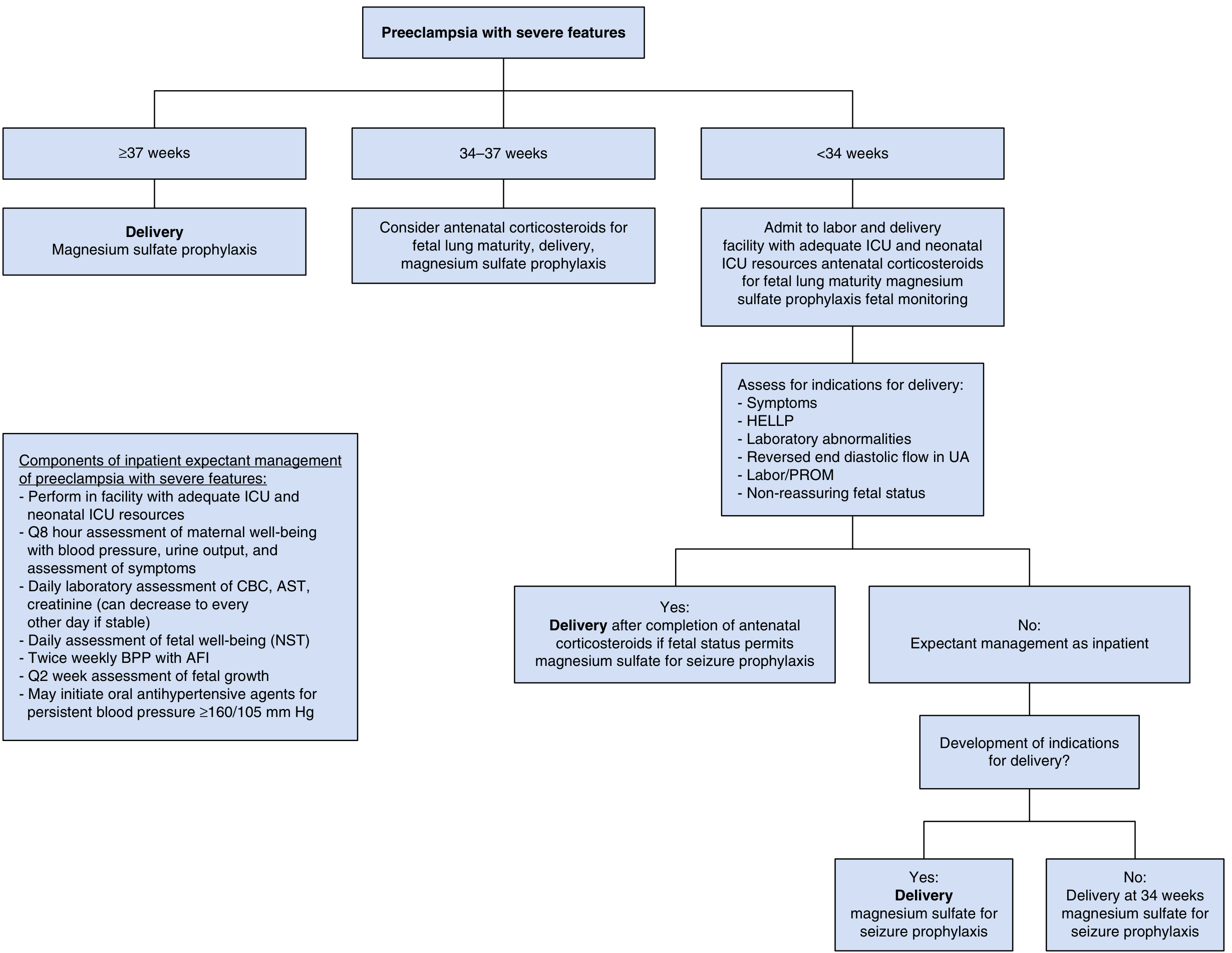
- ≥37 weeks: Deliver with magnesium sulfate prophylaxis
- 34-37 weeks: Consider antenatal corticosteroids for fetal lung maturity, then deliver
- <34 weeks: Admit to tertiary center with ICU/NICU resources; antenatal corticosteroids; expectant management unless indications for delivery arise
Indications to deliver before 34 weeks:
- Unrelenting symptoms (persistent severe headache, visual changes, epigastric pain)
- Laboratory deterioration (HELLP, worsening renal/liver function)
- Severe-range BP refractory to therapy
- Placental abruption
- Reversed end-diastolic flow on umbilical Doppler
- Non-reassuring fetal status
Inpatient expectant management components:
- BP, urine output, symptoms assessed every 8 hours
- Daily CBC, AST, creatinine (can space to every other day if stable)
- Daily NST, twice-weekly BPP with AFI
- Fetal growth assessment every 2 weeks
C. Acute Severe Hypertension (BP ≥160/110 mmHg) - Urgent Treatment
Goal: Lower BP within 30-60 minutes to reduce stroke risk
| Drug | Route | Dose |
|---|---|---|
| Labetalol (preferred IV) | IV | 10-20 mg; then 1-2 mg/min or 20-80 mg q10-30 min; max 300 mg |
| Hydralazine | IV | 5 mg initially; then 0.5-10 mg/hr or 5-10 mg q20-40 min; max 20 mg |
| Nifedipine IR | Oral | 10-20 mg initially; repeat at 20 min; then 10-20 mg q2-6h; max 180 mg |
(Source: Goldman-Cecil Medicine)
Note: ACE inhibitors and ARBs are contraindicated in pregnancy (stillbirth, fetal renal anomalies, oligohydramnios).
D. Chronic Hypertension in Pregnancy
Target BP: <140/90 mmHg (ACOG); reduces risk of superimposed preeclampsia and preterm birth
First-line agents:
- Labetalol (combined alpha/beta blocker) - most commonly used
- Extended-release Nifedipine (calcium channel blocker) - safe, no effect on uterine blood flow
- Methyldopa (centrally acting alpha-2 agonist) - the only agent with long-term infant safety data; limited by side effects (fatigue, orthostatic hypotension); iron supplementation interferes with absorption
Caution with beta-blockers: Pure beta-blockers (especially atenolol) increase risk of fetal growth restriction; labetalol is preferred over atenolol.
E. Magnesium Sulfate (Seizure Prophylaxis and Treatment)
Indications: Preeclampsia with severe features; eclampsia
Protocol:
- Loading dose: 4-6 g IV over 15-20 minutes
- Maintenance: 2 g/hour continuous infusion
- Continue for 24-48 hours postpartum
For eclamptic seizures:
- Give MgSO₄ empirically even while evaluation is underway
- If seizures persist: additional 2 g loading dose
- Avoid respiratory depressants
Toxicity monitoring:
- Loss of deep tendon reflexes (first sign; at ~7-10 mEq/L)
- Respiratory depression (at ~10-13 mEq/L)
- Cardiac arrest (at >15 mEq/L)
- MgSO₄ is renally cleared - women with renal impairment require close monitoring
Antidote: Calcium gluconate 1 g IV over 2-5 minutes
F. Postpartum Management
- Preeclampsia/eclampsia can present or worsen up to 6 weeks postpartum - most common in the first 48-72 hours after delivery
- Continue MgSO₄ for 24-48 hours after delivery
- Monitor BP closely; treat postpartum hypertension ≥150/100 mmHg
- Nifedipine, labetalol, and furosemide (if pulmonary edema) are compatible with breastfeeding
- Ambulatory BP monitoring and home BP checks recommended
G. Prevention - Low-Dose Aspirin
ACOG recommends 81 mg aspirin daily initiated at 12-16 weeks (no later than 20 weeks), continued until ≥36 weeks for women with:
High-risk factors (any one):
- Chronic hypertension
- Prior preeclampsia
- Multifetal gestation
- Pregestational diabetes
- Renal disease
- Autoimmune conditions
- Prior preterm birth <34 weeks
Moderate-risk factors (≥2 needed):
- Nulliparity
- BMI >30
- Family history of preeclampsia
- Age ≥35 years
- Personal/socioeconomic factors
A 2025 Cochrane review (PMID 41330480) further confirms calcium supplementation (especially in low-calcium-intake populations) reduces hypertensive disorders.
6. Complications
Maternal Complications
Neurologic:
- Eclampsia - generalized tonic-clonic seizures; post-ictal state with hypoxia, hypercapnia, lactic acidemia
- Cerebrovascular accidents (ischemic or hemorrhagic stroke) - cerebral dysautoregulation allows hypertensive injury at modest BP elevations
- PRES (posterior reversible encephalopathy syndrome) - occipital/parietal cortical edema; usually reversible with BP control
- Cortical blindness
Hepatic:
- HELLP syndrome (see below)
- Subcapsular hepatic hematoma - life-threatening; can rupture spontaneously
- Acute liver failure
Renal:
- Acute kidney injury (renal failure in ~50% of HELLP cases)
- Glomerular endotheliosis (pathognomonic histologic lesion - endothelial cell swelling causing near-occlusion of capillary lumens)
- Cortical necrosis in severe cases
Cardiopulmonary:
- Pulmonary edema - majority develop postpartum; worsened by aggressive fluid administration
- Cardiomyopathy (increased afterload, LV diastolic dysfunction)
Hematologic:
- DIC
- Microangiopathic hemolytic anemia
Other:
- Placental abruption
- Retinal detachment or Purtscher-like retinopathy
HELLP Syndrome - Detailed
- Occurs in 10-20% of severe preeclampsia; ~20% have no prior recognized preeclampsia
- Complications: renal failure, hepatic rupture, placental abruption, DIC, pulmonary edema, cerebrovascular events, permanent vision loss, fetal demise
- LDH:AST ratio in HELLP with preeclampsia is ~13:1 vs ~29:1 without preeclampsia (diagnostic aid)
- ADAMTS13 activity is reduced 30-60% in HELLP (but not <10% as in TTP)
- Management: Delivery is key; MgSO₄ seizure prophylaxis; antihypertensives; plasma exchange has no proven benefit; antenatal corticosteroids may accelerate recovery; screen for TTP/aHUS
- Usually resolves spontaneously after delivery
Fetal/Neonatal Complications
- Intrauterine growth restriction (IUGR) - from placental insufficiency
- Preterm birth - from iatrogenic delivery for maternal/fetal indications
- Placental abruption - abrupt placental separation
- Intrauterine fetal demise (stillbirth)
- Neonatal respiratory distress syndrome - from prematurity
- Low Apgar scores, hypoxic-ischemic encephalopathy
Long-Term Complications for the Mother
Women with HDP face substantially elevated long-term cardiovascular risks:
| Outcome | Risk |
|---|---|
| Chronic hypertension 2-7 years later | 36.5% (vs. 17% controls) |
| After early preeclampsia | ~50% develop HTN |
| After gestational hypertension | ~39% develop HTN |
| After late-onset preeclampsia | ~25% develop HTN |
| CVD (CAD, stroke, heart failure) | Risk ratio ~2x; up to 8x for early-onset PE |
| LV diastolic dysfunction | Detectable up to a decade after delivery |
| Chronic kidney disease | Elevated relative risk |
The American Heart Association recognizes a history of hypertension in pregnancy as an established cardiovascular risk factor. Relative risk for CVD diminishes post-menopause but absolute burden remains high.
7. Additional Important Components
Postpartum Surveillance (Long-Term)
- Annual BP checks for all women with prior HDP
- Cardiovascular risk factor modification (lifestyle, statins if indicated)
- Renal function monitoring
- Referral to cardiology or internist if high-risk
Differential Diagnosis of Hypertension in Pregnancy
- Chronic essential hypertension unmasked
- Secondary hypertension: renal artery stenosis, pheochromocytoma, Cushing syndrome, primary hyperaldosteronism, coarctation of aorta
- TTP vs. aHUS vs. HELLP (all can present with thrombocytopenia + renal failure in pregnancy)
- Antiphospholipid syndrome
Key Drug Contraindications in Pregnancy
| Drug Class | Status |
|---|---|
| ACE inhibitors (e.g., enalapril) | Contraindicated - fetal renal dysgenesis, oligohydramnios, stillbirth |
| ARBs (e.g., losartan) | Contraindicated - same mechanism |
| Direct renin inhibitors | Contraindicated |
| Atenolol (beta-blocker) | Avoid - high risk IUGR |
| Nitroprusside | Avoid if possible - fetal cyanide toxicity risk |
Anesthetic Considerations (for Delivery)
- Epidural/spinal anesthesia preferred over general anesthesia in preeclampsia - reduces BP response to intubation, avoids airway risks of edema
- Risk of spinal hematoma if platelets <70,000-100,000/µL (assess case-by-case)
- Aggressive fluid preloading with spinal should be avoided (risk of pulmonary edema)
ACOG vs. ESC/ESH Differences in Management
- US (ACOG): Target <140-150/90-100 mmHg for non-severe disease
- European (ESH/ESC): Target <140/90 mmHg
- Canadian guidelines: Target DBP <85 mmHg
- All agree on immediate treatment of BP ≥160/110 mmHg
Sources: Braunwald's Heart Disease (9780323722193), Goldman-Cecil Medicine (9780323930345), Creasy & Resnik's Maternal-Fetal Medicine (9780323828499), Harrison's Principles of Internal Medicine 22e (9781265977061), Brenner & Rector's The Kidney (9780323532655) | ACOG Practice Bulletin No. 222, 2020
compile all this into a pdf
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.