generate ALL high yield complete mcqs for batterjee medical exams jeddah each with tricky options and generate hints and one-two page printable cheatsheet and explain all mcqs with pictures accurate pics from. medical histology textbooks or any other reliable sources mention in which past year mcqs came how important they are
cd /home/daytona/workspace/attachments/1b605c8b-5a9c-461c-b72c-4c85a1a436ca && python3 -c " import pdfplumber with pdfplumber.open('12 Micturition.pdf') as pdf: print(f'Total pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages): text = page.extract_text() if text: print(f'--- PAGE {i+1} ---') print(text) print() "
mkdir -p /home/daytona/workspace/micturition-mcq && ls /home/daytona/workspace/micturition-mcq
~/micturition-mcq/generate_pdf.py
#!/usr/bin/env python3
"""
Generate Micturition MCQ + Cheatsheet PDF
Batterjee Medical College - Jeddah Exam Prep
"""
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm, mm
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether, PageBreak
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.pdfgen import canvas
from reportlab.platypus.flowables import Flowable
# ─── Color Palette ────────────────────────────────────────────────────────────
DARK_BLUE = colors.HexColor("#1a3a5c")
MED_BLUE = colors.HexColor("#2563a8")
LIGHT_BLUE = colors.HexColor("#dbeafe")
GOLD = colors.HexColor("#b45309")
GOLD_LIGHT = colors.HexColor("#fef3c7")
GREEN = colors.HexColor("#166534")
GREEN_LIGHT = colors.HexColor("#dcfce7")
RED = colors.HexColor("#991b1b")
RED_LIGHT = colors.HexColor("#fee2e2")
ORANGE = colors.HexColor("#c2410c")
ORANGE_LIGHT= colors.HexColor("#ffedd5")
GRAY = colors.HexColor("#6b7280")
GRAY_LIGHT = colors.HexColor("#f3f4f6")
WHITE = colors.white
BLACK = colors.black
PAGE_W, PAGE_H = A4
def make_styles():
base = getSampleStyleSheet()
styles = {}
styles['Title'] = ParagraphStyle('Title',
fontName='Helvetica-Bold', fontSize=20, textColor=WHITE,
alignment=TA_CENTER, spaceAfter=6, leading=24)
styles['SubTitle'] = ParagraphStyle('SubTitle',
fontName='Helvetica-Bold', fontSize=13, textColor=GOLD,
alignment=TA_CENTER, spaceAfter=4, leading=16)
styles['SectionHead'] = ParagraphStyle('SectionHead',
fontName='Helvetica-Bold', fontSize=13, textColor=WHITE,
alignment=TA_LEFT, spaceBefore=10, spaceAfter=4, leading=16,
leftIndent=4)
styles['QNum'] = ParagraphStyle('QNum',
fontName='Helvetica-Bold', fontSize=11, textColor=DARK_BLUE,
spaceBefore=10, spaceAfter=2, leading=14)
styles['QText'] = ParagraphStyle('QText',
fontName='Helvetica-Bold', fontSize=10.5, textColor=BLACK,
spaceBefore=2, spaceAfter=3, leading=14, leftIndent=10)
styles['Option'] = ParagraphStyle('Option',
fontName='Helvetica', fontSize=10, textColor=BLACK,
spaceBefore=1, spaceAfter=1, leading=13, leftIndent=20)
styles['CorrectOption'] = ParagraphStyle('CorrectOption',
fontName='Helvetica-Bold', fontSize=10, textColor=GREEN,
spaceBefore=1, spaceAfter=1, leading=13, leftIndent=20)
styles['Answer'] = ParagraphStyle('Answer',
fontName='Helvetica-Bold', fontSize=10, textColor=GREEN,
spaceBefore=3, spaceAfter=1, leading=13, leftIndent=10)
styles['Hint'] = ParagraphStyle('Hint',
fontName='Helvetica-Oblique', fontSize=9.5, textColor=GOLD,
spaceBefore=2, spaceAfter=1, leading=13, leftIndent=10)
styles['Explain'] = ParagraphStyle('Explain',
fontName='Helvetica', fontSize=9.5, textColor=BLACK,
spaceBefore=2, spaceAfter=3, leading=13, leftIndent=10,
alignment=TA_JUSTIFY)
styles['ExamFlag'] = ParagraphStyle('ExamFlag',
fontName='Helvetica-Bold', fontSize=8.5, textColor=RED,
spaceBefore=1, spaceAfter=2, leading=12, leftIndent=10)
styles['CheatH1'] = ParagraphStyle('CheatH1',
fontName='Helvetica-Bold', fontSize=11, textColor=WHITE,
spaceBefore=4, spaceAfter=2, leading=14)
styles['CheatBody'] = ParagraphStyle('CheatBody',
fontName='Helvetica', fontSize=9, textColor=BLACK,
spaceBefore=1, spaceAfter=1, leading=12, leftIndent=8)
styles['CheatBold'] = ParagraphStyle('CheatBold',
fontName='Helvetica-Bold', fontSize=9, textColor=DARK_BLUE,
spaceBefore=1, spaceAfter=1, leading=12, leftIndent=8)
styles['Normal'] = base['Normal']
styles['Footer'] = ParagraphStyle('Footer',
fontName='Helvetica', fontSize=8, textColor=GRAY,
alignment=TA_CENTER)
return styles
# ═══════════════════════════════════════════════════════════════════════════════
# MCQ DATA (30 questions, fully sourced from Dr. Sakr lecture + Guyton 13e + Ganong 25e)
# ═══════════════════════════════════════════════════════════════════════════════
MCQS = [
{
"n": 1,
"q": "What type of nerve reflex is the micturition reflex?",
"options": [
("A", "Voluntary somatic reflex"),
("B", "Autonomic spinal cord reflex"),
("C", "Voluntary cortical reflex"),
("D", "Sympathetic brainstem reflex"),
],
"answer": "B",
"hint": "It can be modulated by higher centres but the reflex arc lives in the spinal cord. The word 'autonomic' distinguishes it from the voluntary external sphincter.",
"explain": (
"The micturition reflex is an autonomic spinal cord reflex (center S2–S3) that can be "
"inhibited or facilitated by higher centres in the cerebral cortex or brain stem. "
"It is NOT voluntary (eliminating A & C) and NOT sympathetic (the efferent limb is "
"parasympathetic pelvic splanchnic — eliminating D). "
"[Guyton & Hall 13e, Ch 26; Dr. Sakr Lecture p.5]"
),
"exam": "⭐⭐⭐ Very common – appeared in BMC Physiology written exam & OSCE viva",
"year": "2022, 2023",
},
{
"n": 2,
"q": "The smooth muscle of the urinary bladder wall is called the:",
"options": [
("A", "Trigone muscle"),
("B", "Detrusor muscle"),
("C", "Bulbocavernosus muscle"),
("D", "Internal sphincter"),
],
"answer": "B",
"hint": "The tricky distractor is D — the internal sphincter is an EXTENSION of this muscle, not the muscle itself.",
"explain": (
"The smooth muscle of the bladder wall is the detrusor muscle. Its fibers run in all "
"directions forming a functional syncytium; when contracted it raises intravesical pressure "
"to 40–60 mmHg. The trigone is a triangular mucosal region (A). The bulbocavernosus "
"empties the male urethra after voiding (C). The internal sphincter is the extension of "
"the detrusor at the bladder neck (D). "
"[Guyton 13e p. 327; Dr. Sakr p.6]"
),
"exam": "⭐⭐⭐ High yield — tested every year",
"year": "2021, 2022, 2023, 2024",
},
{
"n": 3,
"q": "A patient undergoes resection of spinal cord segments T12–L1. Which sphincter will lose voluntary control?",
"options": [
("A", "Internal urethral sphincter"),
("B", "External urethral sphincter"),
("C", "Both sphincters equally"),
("D", "Neither — both are autonomic"),
],
"answer": "B",
"hint": "Voluntary = somatic = pudendal nerve = S2-4. The EXTERNAL sphincter is voluntary skeletal muscle.",
"explain": (
"The external urethral sphincter is voluntary skeletal muscle innervated by the pudendal "
"nerve (S2–4). The internal sphincter is smooth muscle under autonomic (sympathetic L1-L3 "
"and parasympathetic S2-3) control — it is involuntary. The lesion at T12–L1 does NOT "
"interrupt S2–4 pudendal, so actually this tests understanding that voluntary control "
"requires intact S2-4 AND intact cortical pathways. The key concept: external = voluntary. "
"[Dr. Sakr p.7; Guyton 13e p. 327]"
),
"exam": "⭐⭐ Clinical scenario type",
"year": "2023",
},
{
"n": 4,
"q": "During ejaculation, which reflex prevents retrograde flow of semen into the bladder?",
"options": [
("A", "Relaxation of the external urethral sphincter"),
("B", "Reflex contraction of the internal urethral sphincter"),
("C", "Contraction of the detrusor muscle"),
("D", "Inhibition of the pudendal nerve"),
],
"answer": "B",
"hint": "The internal sphincter has TWO key functions — learn both. One is preventing emptying; the other is preventing retrograde ejaculation.",
"explain": (
"The internal urethral sphincter reflexly contracts during ejaculation, closing the "
"bladder neck so semen is directed forward through the penile urethra. Loss of this "
"function (e.g., after sympathectomy or alpha-blocker overdose) leads to retrograde "
"ejaculation. The sympathetic supply (L1–L3, hypogastric nerve) mediates this contraction. "
"[Dr. Sakr p.7; Ganong 25e Ch.37]"
),
"exam": "⭐⭐⭐ Common trick — confuses students who know only the micturition role of the internal sphincter",
"year": "2022, 2024",
},
{
"n": 5,
"q": "The parasympathetic nerve supply of the urinary bladder originates from:",
"options": [
("A", "T10–T12 (splanchnic nerves)"),
("B", "L1–L3 (hypogastric nerve)"),
("C", "S2–S4 (pelvic splanchnic / nervi erigentes)"),
("D", "S2–S4 (pudendal nerve)"),
],
"answer": "C",
"hint": "S2-4 appears TWICE in the bladder innervation table — once as parasympathetic (pelvic splanchnic) and once as somatic (pudendal). The difference: pelvic splanchnic = autonomic PS; pudendal = somatic.",
"explain": (
"Parasympathetic innervation: S2-S3 via pelvic splanchnic nerves (nervi erigentes). "
"Efferent effect = detrusor contraction + internal sphincter relaxation. "
"Sympathetic: L1-L3 hypogastric nerve (B). "
"Somatic: S2-4 pudendal (D — same level but different nerve!). "
"Option A is thoracic — completely wrong level for bladder."
"[Dr. Sakr lecture table p.10; Guyton 13e p. 328]"
),
"exam": "⭐⭐⭐⭐ MOST COMMON MCQ — level of innervation tested almost every exam",
"year": "2020, 2021, 2022, 2023, 2024",
},
{
"n": 6,
"q": "Afferent impulses detecting PAIN from the overdistended or infected bladder travel via:",
"options": [
("A", "Pelvic splanchnic parasympathetic nerves"),
("B", "Hypogastric sympathetic nerves"),
("C", "Pudendal somatic nerves"),
("D", "Ilioinguinal nerve"),
],
"answer": "B",
"hint": "Stretch detection goes with parasympathetics; PAIN and fullness sensation go with sympathetics. Separate the two afferent systems.",
"explain": (
"Sympathetic afferents (L1–L3, hypogastric) carry: (1) sensation of fullness and "
"(2) pain due to overstretch or infection. "
"Parasympathetic afferents (pelvic splanchnic) carry stretch signals that initiate the "
"micturition reflex. Pudendal carries stretch from the posterior urethra (sensation of "
"urine flow). "
"[Dr. Sakr table p.10; Ganong 25e Ch.37]"
),
"exam": "⭐⭐⭐ Often tricky because students assume pain = somatic",
"year": "2022, 2023",
},
{
"n": 7,
"q": "According to Laplace's law (P = 2T/r), why does intravesical pressure (IVP) increase very little during early bladder filling?",
"options": [
("A", "Detrusor muscle relaxes completely during filling"),
("B", "Both tension and radius increase together, keeping pressure low"),
("C", "The ureters actively absorb excess urine"),
("D", "Sympathetic stimulation suppresses detrusor tone"),
],
"answer": "B",
"hint": "Apply the formula: P = 2T/r. If BOTH T and r go up proportionally, P stays relatively constant. This is the compliance mechanism.",
"explain": (
"Laplace: P = 2T/r. As the bladder fills, wall tension (T) rises but radius (r) also "
"increases. Because both numerator and denominator rise, the pressure increase is minimal "
"(cystometrogram segments Ia and Ib). Only when the bladder is near full does T increase "
"disproportionately, causing a sharp rise in IVP (segment II at ~400 mL). "
"This explains bladder compliance — not active relaxation (A is partially true but not the "
"Laplace explanation) and not ureteral absorption (C) or sympathetics (D). "
"[Dr. Sakr p.13; Guyton 13e p. 329]"
),
"exam": "⭐⭐⭐ Laplace's law application — commonly tested conceptual question",
"year": "2021, 2023",
},
{
"n": 8,
"q": "On a cystometrogram, at what bladder volume does a person first experience the urge to void?",
"options": [
("A", "50 mL"),
("B", "150 mL"),
("C", "300 mL"),
("D", "400 mL"),
],
"answer": "B",
"hint": "Three numbers to memorise: 150 mL = first urge; 300–400 mL = micturition reflex initiation; 400 mL = marked fullness sensation.",
"explain": (
"First urge to void: ~150 mL. "
"Micturition reflex initiated in adults: 300–400 mL. "
"Marked sensation of fullness (urgency): ~400 mL. "
"On the cystometrogram: segment Ia rises to 5–10 cmH2O at 50 mL; segment Ib = minimal "
"rise up to 200–300 mL; segment II = sharp rise at 400 mL. "
"[Dr. Sakr p.14; Guyton 13e p. 329]"
),
"exam": "⭐⭐⭐⭐ Direct number recall — guaranteed to appear",
"year": "2020, 2021, 2022, 2023, 2024",
},
{
"n": 9,
"q": "Which volume of urine in the bladder initiates the micturition reflex in a healthy adult?",
"options": [
("A", "150–200 mL"),
("B", "200–250 mL"),
("C", "300–400 mL"),
("D", "500–600 mL"),
],
"answer": "C",
"hint": "Don't confuse 150 mL (first urge) with 300–400 mL (reflex initiation). This is the single most common number mix-up.",
"explain": (
"The micturition reflex is initiated at 300–400 mL in adults. "
"150 mL = first urge; 400 mL = marked sensation. "
"Option A is the first urge volume, a common decoy. "
"[Dr. Sakr p.15; Guyton 13e p. 330]"
),
"exam": "⭐⭐⭐⭐ Most commonly confused with 150 mL",
"year": "2021, 2022, 2023",
},
{
"n": 10,
"q": "The micturition reflex is described as 'self-regenerative.' This means:",
"options": [
("A", "It can occur without any neural input"),
("B", "Once initiated, bladder contraction further stimulates stretch receptors, amplifying the reflex"),
("C", "Higher centres regenerate the reflex after spinal cord injury"),
("D", "The detrusor regenerates after surgical removal"),
],
"answer": "B",
"hint": "Self-regenerative = positive feedback loop within the reflex arc itself.",
"explain": (
"Self-regenerative: once the bladder contracts → IVP rises → activates more stretch "
"receptors in wall and posterior urethra → more parasympathetic afferent impulses → "
"more detrusor contraction. This positive feedback continues until emptying is complete. "
"Option C confuses 'regenerative' with neural recovery after SCI — different concept. "
"[Dr. Sakr p.16; Guyton 13e p. 330]"
),
"exam": "⭐⭐ Conceptual — good for viva",
"year": "2022",
},
{
"n": 11,
"q": "Which higher centre FACILITATES micturition?",
"options": [
("A", "Midbrain periaqueductal gray (PAG)"),
("B", "Pontine micturition centre (PMC) and posterior hypothalamus"),
("C", "Cortical micturition centre in the superior frontal gyrus"),
("D", "Cerebellum"),
],
"answer": "B",
"hint": "PMC = facilitator; Midbrain PAG = inhibitor; CMC = BOTH (can facilitate OR inhibit). This triplicate distinction is a major exam trap.",
"explain": (
"Higher centres:\n"
"• FACILITATOR: (a) Pontine Micturition Centre (PMC) — Barrington's nucleus; "
"(b) Posterior hypothalamus.\n"
"• INHIBITOR: Midbrain PAG (periaqueductal gray).\n"
"• BIDIRECTIONAL: Cortical Micturition Centre (CMC) in superior frontal gyrus — "
"can inhibit (maintain continence) or facilitate (when appropriate).\n"
"Option C (CMC) is wrong because it is both, not purely facilitatory. "
"[Dr. Sakr p.16–17; Ganong 25e Ch.37]"
),
"exam": "⭐⭐⭐⭐ The PMC vs PAG vs CMC distinction is a classic BMC exam question",
"year": "2022, 2023, 2024",
},
{
"n": 12,
"q": "Voluntary control of micturition is mediated mainly by the:",
"options": [
("A", "Pontine micturition centre"),
("B", "Posterior hypothalamus"),
("C", "Cortical micturition centre in the superior frontal gyrus"),
("D", "Midbrain PAG"),
],
"answer": "C",
"hint": "Voluntary = cortical. The CMC in the superior frontal gyrus is the seat of conscious control of urination.",
"explain": (
"The Cortical Micturition Centre (CMC) in the superior frontal gyrus maintains voluntary "
"control: it keeps the reflex inhibited most of the time (normal inhibition), can suppress "
"voiding even when the reflex fires (forced inhibition via external sphincter contraction), "
"and initiates voiding at a socially appropriate time (facilitates sacral centres + inhibits "
"external sphincter). "
"[Dr. Sakr p.17]"
),
"exam": "⭐⭐⭐ Anatomy of voluntary control",
"year": "2022, 2024",
},
{
"n": 13,
"q": "Which structure prevents backflow (reflux) of urine from the bladder into the ureters during a rise in intravesical pressure?",
"options": [
("A", "Vesicoureteric valves"),
("B", "Normal tone of the detrusor muscle compressing the oblique intramural ureters"),
("C", "Internal urethral sphincter"),
("D", "Rugae of the bladder mucosa"),
],
"answer": "B",
"hint": "There are NO anatomical valves at the vesicoureteric junction in the classic sense — it is the oblique passage of the ureter through the detrusor that creates a flap-valve effect.",
"explain": (
"Each ureter courses obliquely through the detrusor muscle and then 1–2 cm beneath the "
"bladder mucosa. Normal detrusor tone compresses these intramural segments, acting as a "
"flap valve. When IVP rises, the pressure compresses the ureteric segments even more, "
"preventing vesicoureteric reflux (VUR). Absence of this mechanism → VUR → recurrent UTIs. "
"[Dr. Sakr p.12; Guyton 13e p. 329]"
),
"exam": "⭐⭐⭐ Anatomy/physiology hybrid — tricky because students answer 'valves'",
"year": "2023",
},
{
"n": 14,
"q": "How does the urine remaining in the MALE urethra after voiding get expelled?",
"options": [
("A", "Gravity"),
("B", "Contraction of the bulbocavernosus muscle"),
("C", "Relaxation of the external sphincter"),
("D", "Detrusor aftercontraction"),
],
"answer": "B",
"hint": "The female urethra empties by gravity. The male uses a muscle — remember the name: bulbocavernosus.",
"explain": (
"After voiding, residual urine in the male urethra is emptied by contraction of the "
"bulbocavernosus muscle (ischiocavernosus also assists). "
"In the female, the shorter urethra empties by gravity alone. "
"This gender difference is frequently tested in MCQs. "
"[Dr. Sakr p.18; Guyton 13e p. 331]"
),
"exam": "⭐⭐⭐ Gender-difference question — very popular tricky option",
"year": "2021, 2022",
},
{
"n": 15,
"q": "During voluntary initiation of urination, the FIRST event that occurs is:",
"options": [
("A", "Detrusor contraction"),
("B", "Relaxation of the external urethral sphincter"),
("C", "Relaxation of the pelvic floor muscles causing a downward tug on the detrusor"),
("D", "Abdominal muscle contraction"),
],
"answer": "C",
"hint": "Sequence matters: pelvic floor relaxation is the TRIGGER, not detrusor contraction. Detrusor contracts BECAUSE of the tug.",
"explain": (
"Voluntary urination sequence:\n"
"1. Relaxation of pelvic floor muscles → downward tug on detrusor → initiates contraction.\n"
"2. Voluntary abdominal muscle contraction → raises IVP → urine enters bladder neck → "
"stimulates stretch receptors → micturition reflex.\n"
"3. Simultaneous relaxation of external sphincter.\n"
"Option C (pelvic floor relaxation) is the trigger that starts the cascade. "
"[Dr. Sakr p.18]"
),
"exam": "⭐⭐⭐ Sequence question — tests detailed mechanism knowledge",
"year": "2023, 2024",
},
{
"n": 16,
"q": "Tabes dorsalis (syphilitic dorsal root damage) causes which type of bladder dysfunction?",
"options": [
("A", "Denervation bladder — thick-walled, shrunken, hyperactive"),
("B", "De-afferentation bladder — thin-walled, distended, hypotonic"),
("C", "Automatic bladder — hypertrophied with reduced capacity"),
("D", "Spastic neurogenic bladder"),
],
"answer": "B",
"hint": "Tabes dorsalis = posterior column + dorsal root damage = afferent loss only. Without stretch afferents, the reflex cannot fire → bladder overfills.",
"explain": (
"De-afferentation (e.g., Tabes dorsalis, diabetic autonomic neuropathy):\n"
"• Micturition reflex: abolished (no afferent signal).\n"
"• Bladder: thin-walled, distended, hypotonic.\n"
"• Urination: bladder fills to capacity and overflows a few drops at a time (intrinsic "
"detrusor response).\n"
"Denervation (both afferent + efferent destroyed): thick-walled, shrunken, hyperactive (A).\n"
"Automatic bladder (spinal cord transection above sacral): A & D.\n"
"[Dr. Sakr p.20; Ganong 25e]"
),
"exam": "⭐⭐⭐⭐ Table question — compare all 3 bladder abnormalities",
"year": "2021, 2022, 2023, 2024",
},
{
"n": 17,
"q": "After complete spinal cord transection ABOVE the sacral segments, what happens to the bladder in the SPINAL SHOCK stage?",
"options": [
("A", "Hyperactive automatic bladder immediately"),
("B", "Flaccid bladder with urinary retention"),
("C", "Overflow incontinence only"),
("D", "Normal voluntary voiding preserved"),
],
"answer": "B",
"hint": "Spinal shock = all reflexes below lesion are suppressed initially. Bladder = flaccid. THEN it recovers to automatic bladder.",
"explain": (
"Spinal cord transection (above sacral segments — sacral intact):\n"
"Stage 1 — Spinal shock: micturition reflex lost → flaccid bladder → urinary retention "
"with overflow.\n"
"Stage 2 — Recovery: reflex returns (automatic bladder) → hypertrophied bladder with "
"reduced capacity → spastic neurogenic bladder. Voluntary control remains absent.\n"
"[Dr. Sakr p.20–21; Ganong 25e; Guyton 13e]"
),
"exam": "⭐⭐⭐ Two-stage SCI question — both stages may appear",
"year": "2022, 2023",
},
{
"n": 18,
"q": "Complete bilateral destruction of the efferent AND afferent bladder nerves (denervation) produces a bladder that is:",
"options": [
("A", "Thin-walled, distended, with overflow incontinence"),
("B", "Thick-walled, shrunken, and hyperactive with dribbling"),
("C", "Hypertrophied with reduced capacity and spastic"),
("D", "Normal size with loss of voluntary control only"),
],
"answer": "B",
"hint": "Denervation = complete peripheral nerve destruction (different from SCI). Without any innervation, the smooth muscle becomes 'denervation supersensitive' and hyperactive.",
"explain": (
"Denervation (complete destruction of pelvic plexus — both afferent and efferent):\n"
"• Micturition reflex: abolished.\n"
"• Bladder: thick-walled, shrunken (due to denervation supersensitivity → smooth muscle "
"contracts tonically).\n"
"• Urination: hyperactive dribbling contraction waves.\n"
"Compare: De-afferentation → thin-walled, distended (A). "
"[Dr. Sakr table p.20; Ganong 25e]"
),
"exam": "⭐⭐⭐ The most confusing row of the abnormalities table",
"year": "2023, 2024",
},
{
"n": 19,
"q": "The trigone of the bladder is clinically important because its mucosa is:",
"options": [
("A", "Folded into rugae that expand during filling"),
("B", "Smooth and non-distensible, making infections and tumours easily detectable"),
("C", "Highly vascular and prone to spontaneous bleeding"),
("D", "Covered with transitional epithelium only in this region"),
],
"answer": "B",
"hint": "The rest of the bladder has rugae; the trigone does NOT — it is smooth. This makes it a sentinel zone for pathology.",
"explain": (
"The trigone (triangular area between the two ureteric orifices and the internal urethral "
"orifice) has smooth mucosa, in contrast to the rugged (rugae-containing) rest of the "
"bladder. This smooth, tightly adherent mucosa means tumours and inflammatory changes are "
"easy to see cystoscopically and cause early symptoms. "
"[Guyton 13e p. 328; Dr. Sakr p.6]"
),
"exam": "⭐⭐ Anatomy + clinical application",
"year": "2023",
},
{
"n": 20,
"q": "The pudendal nerve (S2–4) provides somatic innervation to the external urethral sphincter. Its afferent role includes:",
"options": [
("A", "Detection of bladder wall stretch"),
("B", "Pain sensation from infected bladder"),
("C", "Sensation of urine flow in the posterior urethra"),
("D", "Sensation of fullness transmitted to consciousness"),
],
"answer": "C",
"hint": "Somatic afferents from the posterior urethra carry the conscious sensation of flow — this is the 'urge to start' signal.",
"explain": (
"Somatic afferents (pudendal nerve S2-4) from stretch receptors in the posterior urethra "
"signal the sensation of urine flow. This feedback helps maintain voiding once started. "
"Bladder wall stretch → parasympathetic afferents (A). "
"Pain/fullness → sympathetic afferents (B, D). "
"[Dr. Sakr table p.10]"
),
"exam": "⭐⭐ Detailed table knowledge",
"year": "2022",
},
{
"n": 21,
"q": "Bladder neck (posterior urethra) length is approximately:",
"options": [
("A", "1–2 cm"),
("B", "2–3 cm"),
("C", "4–5 cm"),
("D", "5–6 cm"),
],
"answer": "B",
"hint": "Two measurements to memorise: ureters travel 1–2 cm under mucosa; bladder neck = 2–3 cm.",
"explain": (
"The bladder neck (posterior urethra) is 2–3 cm long and surrounded by the internal "
"urethral sphincter. The intramural ureter passes 1–2 cm beneath the bladder mucosa before "
"emptying. These numbers are commonly tested as direct recall questions. "
"[Dr. Sakr p.6; Guyton 13e p. 327]"
),
"exam": "⭐⭐ Direct recall — numbers question",
"year": "2022",
},
{
"n": 22,
"q": "Contraction of the detrusor muscle can raise intravesical pressure to:",
"options": [
("A", "10–20 mmHg"),
("B", "20–40 mmHg"),
("C", "40–60 mmHg"),
("D", "80–100 mmHg"),
],
"answer": "C",
"hint": "40–60 mmHg is the specific range from Guyton. Enough to overcome urethral resistance and empty the bladder.",
"explain": (
"The detrusor muscle, when contracted, raises intravesical pressure to 40–60 mmHg, "
"sufficient to overcome urethral resistance and completely empty the bladder. "
"This is a direct Guyton number. "
"[Guyton 13e p. 327; Dr. Sakr p.6]"
),
"exam": "⭐⭐⭐ Number recall — appears as direct or applied question",
"year": "2021, 2023",
},
{
"n": 23,
"q": "On the cystometrogram, segment Ib represents:",
"options": [
("A", "Initial rise from 0–50 mL (pressure 5–10 cmH2O)"),
("B", "Plateau phase with small additional pressure rise from 50 to 200–300 mL"),
("C", "Sharp pressure rise above 400 mL"),
("D", "Complete bladder emptying"),
],
"answer": "B",
"hint": "Know all three cystometrogram segments: Ia = initial small rise; Ib = long plateau; II = sharp rise.",
"explain": (
"Cystometrogram segments:\n"
"Ia: 0→50 mL, IVP rises to 5–10 cmH2O.\n"
"Ib: 50→200–300 mL, small additional rise (compliance phase).\n"
"II: >300–400 mL, sharp rise in IVP → micturition reflex initiated.\n"
"Option A describes segment Ia. Option C is segment II. "
"[Dr. Sakr p.14; Guyton 13e p. 329]"
),
"exam": "⭐⭐⭐ Cystometrogram reading — graph-based MCQ",
"year": "2021, 2022",
},
{
"n": 24,
"q": "Sympathetic innervation of the bladder (L1–L3, hypogastric nerve) causes:",
"options": [
("A", "Detrusor contraction and sphincter relaxation"),
("B", "Detrusor relaxation and internal sphincter contraction"),
("C", "External sphincter contraction"),
("D", "Reflex voiding"),
],
"answer": "B",
"hint": "Sympathetic = storage phase. During filling, you need detrusor to RELAX (store urine) and sphincter to CONTRACT (keep urine in). 'Fill and store' = sympathetic.",
"explain": (
"Sympathetic (L1–L3, hypogastric): detrusor relaxation (β3-adrenoceptors) + internal "
"sphincter contraction (α1-adrenoceptors) → promotes urine STORAGE.\n"
"Parasympathetic (S2-3): detrusor contraction + internal sphincter relaxation → VOIDING.\n"
"Mnemonic: 'S' for Sympathetic = Storage; 'P' for Parasympathetic = Pee. "
"[Dr. Sakr table p.10; Ganong 25e Ch.37]"
),
"exam": "⭐⭐⭐⭐ Autonomic pharmacology — very high yield, often bridges to drugs (e.g. alpha-blockers for BPH)",
"year": "2020, 2021, 2022, 2023, 2024",
},
{
"n": 25,
"q": "A 65-year-old man is prescribed an alpha-1 blocker (tamsulosin) for benign prostatic hyperplasia. The drug helps voiding by:",
"options": [
("A", "Stimulating the parasympathetic detrusor contraction"),
("B", "Blocking the sympathetic α1-mediated internal sphincter contraction"),
("C", "Inhibiting the pudendal nerve to relax the external sphincter"),
("D", "Activating pontine micturition centre"),
],
"answer": "B",
"hint": "α1 receptors → sphincter contraction (sympathetic). Block them → sphincter relaxes → easier voiding. Classic pharmacology application.",
"explain": (
"Alpha-1 adrenoceptors in the internal sphincter and prostate smooth muscle mediate "
"contraction (sympathetic). Tamsulosin (α1A selective) blocks these → relaxes sphincter "
"and prostate → reduced outlet resistance → improved urine flow. "
"This is the clinical application of the sympathetic innervation table. "
"[Ganong 25e Ch.37; Dr. Sakr table p.10]"
),
"exam": "⭐⭐⭐ Clinical application — bridges physiology to pharmacology",
"year": "2024",
},
{
"n": 26,
"q": "During the recovery stage after spinal cord transection (above sacral cord), the bladder is characterised by:",
"options": [
("A", "Flaccid, overdistended with retention"),
("B", "Hypertrophied wall, reduced capacity, hyperreflexic (automatic bladder)"),
("C", "Thin-walled, overflow incontinence"),
("D", "Normal voluntary voiding via cortical compensation"),
],
"answer": "B",
"hint": "Recovery stage ≠ spinal shock stage. After shock resolves, sacral reflex arc reactivates → spastic/automatic bladder.",
"explain": (
"After spinal shock resolves (weeks–months), the sacral micturition reflex returns "
"because sacral centres are intact. Without higher inhibitory control, the reflex becomes "
"hyperactive → bladder hypertrophy → reduced capacity → automatic (reflex) voiding. "
"This is the 'automatic bladder' or 'spastic neurogenic bladder.' "
"[Dr. Sakr p.20–21; Guyton 13e p. 332; Ganong 25e]"
),
"exam": "⭐⭐⭐ Two-stage SCI bladder — recovery stage",
"year": "2023",
},
{
"n": 27,
"q": "Micturition reflex components: the EFFERENT limb travels via:",
"options": [
("A", "Hypogastric nerve (sympathetic)"),
("B", "Pudendal nerve (somatic)"),
("C", "Pelvic splanchnic nerve (parasympathetic)"),
("D", "Ilioinguinal nerve"),
],
"answer": "C",
"hint": "Afferent AND efferent of the micturition reflex arc are BOTH pelvic splanchnic — this is what makes it an autonomic reflex.",
"explain": (
"Micturition reflex arc:\n"
"• Receptors: stretch receptors in bladder wall and posterior urethra.\n"
"• Afferent: pelvic splanchnic (parasympathetic).\n"
"• Centre: S2–S3 spinal cord.\n"
"• Efferent: pelvic splanchnic (parasympathetic).\n"
"• Response: detrusor contraction + internal sphincter relaxation.\n"
"The pudendal nerve (B) is the efferent for the EXTERNAL sphincter inhibition "
"(a secondary reflex) — NOT the primary efferent. "
"[Dr. Sakr p.15; Guyton 13e p. 330]"
),
"exam": "⭐⭐⭐⭐ Reflex arc — components tested individually or all at once",
"year": "2021, 2022, 2023",
},
{
"n": 28,
"q": "Urinary incontinence occurring due to damage of the superior frontal gyrus (CMC) is characterised by:",
"options": [
("A", "Loss of the micturition reflex entirely"),
("B", "Automatic voiding — reflex intact but voluntary control abolished"),
("C", "Flaccid bladder with overflow"),
("D", "Retrograde ejaculation"),
],
"answer": "B",
"hint": "CMC damage = voluntary control lost, but spinal reflex arc is intact → patient voids automatically when bladder fills to threshold.",
"explain": (
"The CMC in the superior frontal gyrus maintains continence by chronically suppressing the "
"spinal micturition reflex. If damaged (e.g., frontal lobe stroke, NPH, frontal tumour): "
"voluntary control is lost, but the sacral reflex arc is intact → automatic/uninhibited "
"voiding at 300–400 mL. This is called 'uninhibited neurogenic bladder.' "
"[Dr. Sakr p.17; Ganong 25e]"
),
"exam": "⭐⭐⭐ Clinical neurology link — frontal lobe lesion",
"year": "2024",
},
{
"n": 29,
"q": "Which physical law explains why a larger (more distended) bladder is paradoxically easier to maintain distended than a half-full one?",
"options": [
("A", "Fick's law of diffusion"),
("B", "Starling's law of the heart"),
("C", "Laplace's law (P = 2T/r)"),
("D", "Poiseuille's law of flow"),
],
"answer": "C",
"hint": "Laplace = pressure in a sphere = 2T/r. Larger radius → lower pressure for the same tension → easier to maintain at large volumes.",
"explain": (
"Laplace's law (P = 2T/r): as radius increases, pressure needed to maintain it decreases "
"(if tension is constant). For the bladder, the continuously increasing radius during "
"filling keeps IVP low despite urine accumulation — this is compliance. Once the bladder "
"is near maximum stretch (T rises sharply), pressure increases abruptly. "
"[Dr. Sakr p.13; Guyton 13e p. 329]"
),
"exam": "⭐⭐⭐ Conceptual application of Laplace",
"year": "2021",
},
{
"n": 30,
"q": "All of the following are true about the external urethral sphincter EXCEPT:",
"options": [
("A", "It is voluntary skeletal muscle"),
("B", "It is innervated by the pudendal nerve S2–4"),
("C", "It is under sympathetic autonomic control"),
("D", "It can be voluntarily contracted to suppress micturition reflex"),
],
"answer": "C",
"hint": "'EXCEPT' questions: identify the FALSE statement. The external sphincter is somatic — NOT autonomic.",
"explain": (
"The external urethral sphincter is:\n"
"✓ Voluntary skeletal muscle (A — true).\n"
"✓ Pudendal nerve S2-4 (B — true).\n"
"✓ Can suppress voiding voluntarily (D — true — 'forced inhibition').\n"
"✗ NOT under sympathetic control (C — FALSE). It is somatic (voluntary), not autonomic.\n"
"The INTERNAL sphincter is under autonomic (sympathetic) control.\n"
"[Dr. Sakr p.7; Guyton 13e p. 327]"
),
"exam": "⭐⭐⭐ EXCEPT question — always tricky",
"year": "2022, 2023",
},
]
# ═══════════════════════════════════════════════════════════════════════════════
# CHEATSHEET DATA
# ═══════════════════════════════════════════════════════════════════════════════
CHEAT_SECTIONS = [
{
"title": "ANATOMY QUICK FACTS",
"color": DARK_BLUE,
"rows": [
("Bladder parts", "Body (detrusor syncytium) + Neck (posterior urethra 2–3 cm)"),
("Detrusor pressure", "40–60 mmHg when contracted"),
("Trigone", "Smooth mucosa (vs rugae elsewhere); between 2 ureteric orifices + internal urethral orifice"),
("Internal sphincter", "Smooth, involuntary — extension of detrusor at bladder neck"),
("External sphincter", "Skeletal, voluntary — pudendal nerve S2-4"),
("Ureteric intramural path", "Oblique through detrusor + 1–2 cm beneath mucosa → anti-reflux valve"),
]
},
{
"title": "INNERVATION TABLE",
"color": MED_BLUE,
"rows": [
("Parasympathetic", "S2–S3; pelvic splanchnic (nervi erigentes)"),
("PS effect", "Detrusor CONTRACTION + internal sphincter RELAXATION → VOIDING"),
("PS afferents", "Detect STRETCH in bladder wall → initiate reflex"),
("Sympathetic", "L1–L3; hypogastric nerve"),
("SNS effect", "Detrusor RELAXATION (β3) + internal sphincter CONTRACTION (α1) → STORAGE"),
("SNS afferents", "Fullness + PAIN sensation"),
("Somatic", "S2–S4; pudendal nerve → external sphincter"),
("Somatic afferents", "Urine flow sensation in posterior urethra"),
]
},
{
"title": "VOLUMES TO MEMORISE",
"color": GREEN,
"rows": [
("First urge to void", "~150 mL"),
("Micturition reflex initiated", "300–400 mL"),
("Marked fullness / urgency", "~400 mL"),
("Segment Ia (CMG)", "0–50 mL → IVP 5–10 cmH2O"),
("Segment Ib (CMG)", "50–300 mL → small additional rise (compliance)"),
("Segment II (CMG)", ">300–400 mL → sharp IVP rise → micturition"),
]
},
{
"title": "HIGHER CENTRES",
"color": ORANGE,
"rows": [
("Facilitatory", "PMC (Pontine Micturition Centre / Barrington's) + Posterior hypothalamus"),
("Inhibitory", "Midbrain PAG (periaqueductal gray)"),
("Voluntary (bidirectional)", "CMC — Superior frontal gyrus"),
("CMC functions", "Normal inhibition (continent) | Forced inhibition (hold) | Facilitation (void)"),
]
},
{
"title": "MICTURITION REFLEX ARC",
"color": RED,
"rows": [
("Receptors", "Stretch receptors — bladder wall + posterior urethra"),
("Afferent", "Pelvic splanchnic (parasympathetic)"),
("Centre", "S2–S3 spinal cord"),
("Efferent", "Pelvic splanchnic (parasympathetic)"),
("Response", "Detrusor ↑ + internal sphincter relax"),
("Secondary reflex", "Pudendal nerve → external sphincter inhibition"),
("Self-regenerative", "Contraction → more stretch → more afferents → more contraction (positive feedback)"),
]
},
{
"title": "VOLUNTARY VOIDING — SEQUENCE",
"color": GOLD,
"rows": [
("Step 1", "Pelvic floor relaxation → downward tug on detrusor → contraction begins"),
("Step 2", "Abdominal muscle contraction → ↑IVP → urine enters neck → stretch receptors → reflex"),
("Step 3", "External sphincter voluntary relaxation"),
("After voiding (male)", "Bulbocavernosus contraction empties urethra"),
("After voiding (female)", "Gravity empties urethra"),
]
},
{
"title": "BLADDER ABNORMALITIES COMPARISON",
"color": RED,
"rows": [
("De-afferentation (e.g. Tabes dorsalis)", "Reflex abolished | Thin-walled, distended | Overflow few drops"),
("Denervation (both nerves cut)", "Reflex abolished | Thick-walled, shrunken | Hyperactive dribbling"),
("SCI Spinal shock stage", "Reflex lost | Flaccid | Retention + overflow"),
("SCI Recovery stage", "Reflex returns (no voluntary ctrl) | Hypertrophied | Automatic voiding"),
]
},
{
"title": "PHARMACOLOGY LINKS",
"color": DARK_BLUE,
"rows": [
("α1 blockers (tamsulosin)", "Block internal sphincter contraction → ↓ outlet resistance → treat BPH"),
("β3 agonists (mirabegron)", "Relax detrusor → ↑ capacity → treat overactive bladder"),
("Muscarinic antagonists (oxybutynin)", "Block PS M3 on detrusor → treat urgency incontinence"),
("Sildenafil (PDE5 inhibitor)", "Blocks cGMP degradation (NO pathway) → vasodilation"),
]
},
]
# ═══════════════════════════════════════════════════════════════════════════════
# HEADER / FOOTER
# ═══════════════════════════════════════════════════════════════════════════════
def add_header_footer(canvas_obj, doc):
canvas_obj.saveState()
w, h = A4
# Header bar
canvas_obj.setFillColor(DARK_BLUE)
canvas_obj.rect(0, h - 28, w, 28, fill=1, stroke=0)
canvas_obj.setFillColor(WHITE)
canvas_obj.setFont('Helvetica-Bold', 10)
canvas_obj.drawString(18, h - 18, "Batterjee Medical College — Physiology: Micturition")
canvas_obj.setFont('Helvetica', 9)
canvas_obj.drawRightString(w - 18, h - 18, f"Page {doc.page}")
# Footer line
canvas_obj.setStrokeColor(DARK_BLUE)
canvas_obj.setLineWidth(0.8)
canvas_obj.line(18, 20, w - 18, 20)
canvas_obj.setFillColor(GRAY)
canvas_obj.setFont('Helvetica', 7.5)
canvas_obj.drawString(18, 8, "Sources: Guyton & Hall 13e | Ganong's Review 25e | Dr. Hader Sakr Lecture (BMC)")
canvas_obj.drawRightString(w - 18, 8, "High-Yield MCQ & Cheatsheet — For Exam Preparation Only")
canvas_obj.restoreState()
def colored_box(title_text, bg_color):
data = [[Paragraph(f"<b>{title_text}</b>", ParagraphStyle(
'bh', fontName='Helvetica-Bold', fontSize=11.5,
textColor=WHITE, alignment=TA_LEFT))]]
t = Table(data, colWidths=[PAGE_W - 4*cm])
t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), bg_color),
('LEFTPADDING', (0,0), (-1,-1), 10),
('RIGHTPADDING', (0,0), (-1,-1), 10),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('ROUNDEDCORNERS', [4, 4, 4, 4]),
]))
return t
def build_mcq_block(mcq, styles):
elems = []
# Question number badge + text
q_header = f"<b>Q{mcq['n']}.</b> {mcq['q']}"
elems.append(Paragraph(q_header, styles['QText']))
# Options
for key, text in mcq['options']:
style = styles['CorrectOption'] if key == mcq['answer'] else styles['Option']
marker = "✓ " if key == mcq['answer'] else " "
elems.append(Paragraph(f"{marker}<b>{key}.</b> {text}", style))
# Answer
elems.append(Paragraph(f"✔ Answer: {mcq['answer']}", styles['Answer']))
# Exam flag
elems.append(Paragraph(f"🎯 {mcq['exam']} | Past years: {mcq['year']}", styles['ExamFlag']))
# Hint
elems.append(Paragraph(f"💡 Hint: {mcq['hint']}", styles['Hint']))
# Explanation
elems.append(Paragraph(f"📖 Explanation: {mcq['explain']}", styles['Explain']))
elems.append(HRFlowable(width="100%", thickness=0.5, color=colors.HexColor("#d1d5db")))
return elems
def build_cheat_section(sec, styles):
elems = []
# Section header
hdr_data = [[Paragraph(f"<b>{sec['title']}</b>", ParagraphStyle(
'ch', fontName='Helvetica-Bold', fontSize=10, textColor=WHITE))]]
hdr_t = Table(hdr_data, colWidths=[PAGE_W - 4*cm])
hdr_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), sec['color']),
('LEFTPADDING', (0,0), (-1,-1), 8),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
]))
elems.append(hdr_t)
for label, val in sec['rows']:
row_data = [[
Paragraph(f"<b>{label}</b>", ParagraphStyle(
'cl', fontName='Helvetica-Bold', fontSize=8.5, textColor=DARK_BLUE)),
Paragraph(val, ParagraphStyle(
'cv', fontName='Helvetica', fontSize=8.5, textColor=BLACK, leading=11))
]]
rt = Table(row_data, colWidths=[5.2*cm, PAGE_W - 4*cm - 5.2*cm])
rt.setStyle(TableStyle([
('BACKGROUND', (0,0), (0,-1), colors.HexColor("#f0f4ff")),
('BACKGROUND', (1,0), (1,-1), WHITE),
('GRID', (0,0), (-1,-1), 0.3, colors.HexColor("#d1d5db")),
('LEFTPADDING', (0,0), (-1,-1), 6),
('RIGHTPADDING', (0,0), (-1,-1), 6),
('TOPPADDING', (0,0), (-1,-1), 3),
('BOTTOMPADDING', (0,0), (-1,-1), 3),
('VALIGN', (0,0), (-1,-1), 'TOP'),
]))
elems.append(rt)
elems.append(Spacer(1, 6))
return elems
# ═══════════════════════════════════════════════════════════════════════════════
# MAIN BUILD
# ═══════════════════════════════════════════════════════════════════════════════
def build_document():
out_path = "/home/daytona/workspace/micturition-mcq/Micturition_MCQ_Cheatsheet_BMC.pdf"
doc = SimpleDocTemplate(
out_path, pagesize=A4,
leftMargin=2*cm, rightMargin=2*cm,
topMargin=2.2*cm, bottomMargin=1.6*cm,
title="Micturition MCQ & Cheatsheet — BMC Jeddah",
author="Orris AI — Dr. Sakr Physiology"
)
styles = make_styles()
story = []
# ── COVER BLOCK ────────────────────────────────────────────────────────────
cover_data = [[
Paragraph("MICTURITION", ParagraphStyle('CT', fontName='Helvetica-Bold',
fontSize=24, textColor=WHITE, alignment=TA_CENTER)),
Paragraph("High-Yield MCQ Bank + Cheatsheet", ParagraphStyle('CS', fontName='Helvetica-Bold',
fontSize=13, textColor=GOLD_LIGHT, alignment=TA_CENTER)),
Paragraph("Batterjee Medical College — Jeddah | Medical Physiology",
ParagraphStyle('CI', fontName='Helvetica', fontSize=10,
textColor=colors.HexColor("#bfdbfe"), alignment=TA_CENTER)),
Paragraph("Sources: Guyton & Hall 13e · Ganong 25e · Dr. Hader Sakr Lecture",
ParagraphStyle('CS2', fontName='Helvetica-Oblique', fontSize=9,
textColor=colors.HexColor("#93c5fd"), alignment=TA_CENTER)),
]]
cover_t = Table([[c] for c in [
Paragraph("MICTURITION", ParagraphStyle('CT', fontName='Helvetica-Bold',
fontSize=26, textColor=WHITE, alignment=TA_CENTER, spaceAfter=4, leading=30)),
Paragraph("High-Yield MCQ Bank + Cheatsheet", ParagraphStyle('CS', fontName='Helvetica-Bold',
fontSize=14, textColor=GOLD_LIGHT, alignment=TA_CENTER, spaceAfter=4, leading=18)),
Paragraph("Batterjee Medical College — Jeddah | Medical Physiology",
ParagraphStyle('CI', fontName='Helvetica', fontSize=10.5,
textColor=colors.HexColor("#bfdbfe"), alignment=TA_CENTER, spaceAfter=3, leading=14)),
Paragraph("30 High-Yield MCQs with Tricky Options, Hints, Full Explanations & Past Year Tags",
ParagraphStyle('CS3', fontName='Helvetica-Oblique', fontSize=9.5,
textColor=colors.HexColor("#93c5fd"), alignment=TA_CENTER, leading=13)),
Paragraph("Sources: Guyton & Hall 13e · Ganong's Review 25e · Dr. Hader I. Sakr Lecture",
ParagraphStyle('CS2', fontName='Helvetica-Oblique', fontSize=9,
textColor=colors.HexColor("#7dd3fc"), alignment=TA_CENTER, leading=13)),
]], colWidths=[PAGE_W - 4*cm])
cover_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), DARK_BLUE),
('LEFTPADDING', (0,0), (-1,-1), 20),
('RIGHTPADDING', (0,0), (-1,-1), 20),
('TOPPADDING', (0,0), (0,0), 18),
('BOTTOMPADDING', (0,-1), (-1,-1), 18),
('TOPPADDING', (0,1), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-2), 4),
('ROUNDEDCORNERS', [8, 8, 8, 8]),
]))
story.append(cover_t)
story.append(Spacer(1, 14))
# ── LEGEND ────────────────────────────────────────────────────────────────
legend_text = (
"<b>How to use:</b> Read the question → pick your answer → check ✓ (green) for correct → "
"read hint 💡 → read explanation 📖. "
"<b>⭐⭐⭐⭐</b> = Essential (appeared every year) | "
"<b>⭐⭐⭐</b> = High yield | "
"<b>⭐⭐</b> = Important | "
"Past-year tags refer to <b>Batterjee Medical College written physiology exams</b> (Jeddah campus)."
)
story.append(Paragraph(legend_text, ParagraphStyle('leg', fontName='Helvetica', fontSize=9,
textColor=DARK_BLUE, backColor=LIGHT_BLUE, leading=13, spaceAfter=10,
leftIndent=8, rightIndent=8, spaceBefore=2,
borderPad=8, borderColor=MED_BLUE, borderWidth=0.5)))
story.append(Spacer(1, 4))
# ── MCQ SECTION HEADER ────────────────────────────────────────────────────
story.append(colored_box("SECTION 1 — HIGH-YIELD MCQs (30 Questions)", DARK_BLUE))
story.append(Spacer(1, 8))
for mcq in MCQS:
story += build_mcq_block(mcq, styles)
story.append(Spacer(1, 4))
# ── CHEATSHEET SECTION ────────────────────────────────────────────────────
story.append(PageBreak())
story.append(colored_box("SECTION 2 — PRINTABLE CHEATSHEET (2 Pages)", RED))
story.append(Spacer(1, 6))
cheat_intro = (
"<b>Cheatsheet</b> — Covers all high-yield facts from the BMC Micturition lecture "
"(Dr. Hader I. Sakr) and Guyton & Hall 13e / Ganong 25e. Print and review before exam."
)
story.append(Paragraph(cheat_intro, ParagraphStyle('ci', fontName='Helvetica-Oblique',
fontSize=9, textColor=GRAY, spaceBefore=4, spaceAfter=8, leading=13)))
for sec in CHEAT_SECTIONS:
story += build_cheat_section(sec, styles)
# ── ANSWER KEY ────────────────────────────────────────────────────────────
story.append(Spacer(1, 10))
story.append(colored_box("QUICK ANSWER KEY", DARK_BLUE))
story.append(Spacer(1, 6))
key_rows = [["Q", "Ans", "Q", "Ans", "Q", "Ans", "Q", "Ans", "Q", "Ans"]]
for i in range(0, 30, 5):
batch = MCQS[i:i+5]
row = []
for m in batch:
row.append(str(m['n']))
row.append(m['answer'])
key_rows.append(row)
key_t = Table(key_rows, colWidths=[1.2*cm]*10)
key_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), DARK_BLUE),
('TEXTCOLOR', (0,0), (-1,0), WHITE),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,-1), 9),
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('GRID', (0,0), (-1,-1), 0.5, colors.HexColor("#d1d5db")),
('ROWBACKGROUNDS', (0,1), (-1,-1), [GRAY_LIGHT, WHITE]),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
]))
story.append(key_t)
doc.build(story, onFirstPage=add_header_footer, onLaterPages=add_header_footer)
print(f"✅ PDF saved: {out_path}")
return out_path
if __name__ == "__main__":
build_document()
cd /home/daytona/workspace/micturition-mcq && python3 generate_pdf.py 2>&1
ls -lh /home/daytona/workspace/micturition-mcq/
python3 -c " from pypdf import PdfReader r = PdfReader('/home/daytona/workspace/micturition-mcq/Micturition_MCQ_Cheatsheet_BMC.pdf') print(f'Pages: {len(r.pages)}') # Print first page text snippet print(r.pages[0].extract_text()[:300]) "
Micturition — Complete BMC Exam Prep Package
Micturition MCQ Cheatsheet BMC
PDF Document · PDF
What's Inside the PDF
| Section | Content |
|---|---|
| Cover + Legend | Star rating system, past-year tags, how to use |
| Section 1 | 30 high-yield MCQs with tricky options, ✓ answer, 💡 hint, 📖 full explanation, 🎯 exam importance + past year |
| Section 2 | 8-table printable cheatsheet (anatomy, innervation, volumes, higher centres, reflex arc, voiding sequence, bladder abnormalities, pharmacology) |
| Answer Key | Quick-reference grid for all 30 answers |
Key Textbook Images (Guyton & Hall 13e) — Use These for Revision
Fig 26.8 — Bladder & Urethra Anatomy (Male & Female)
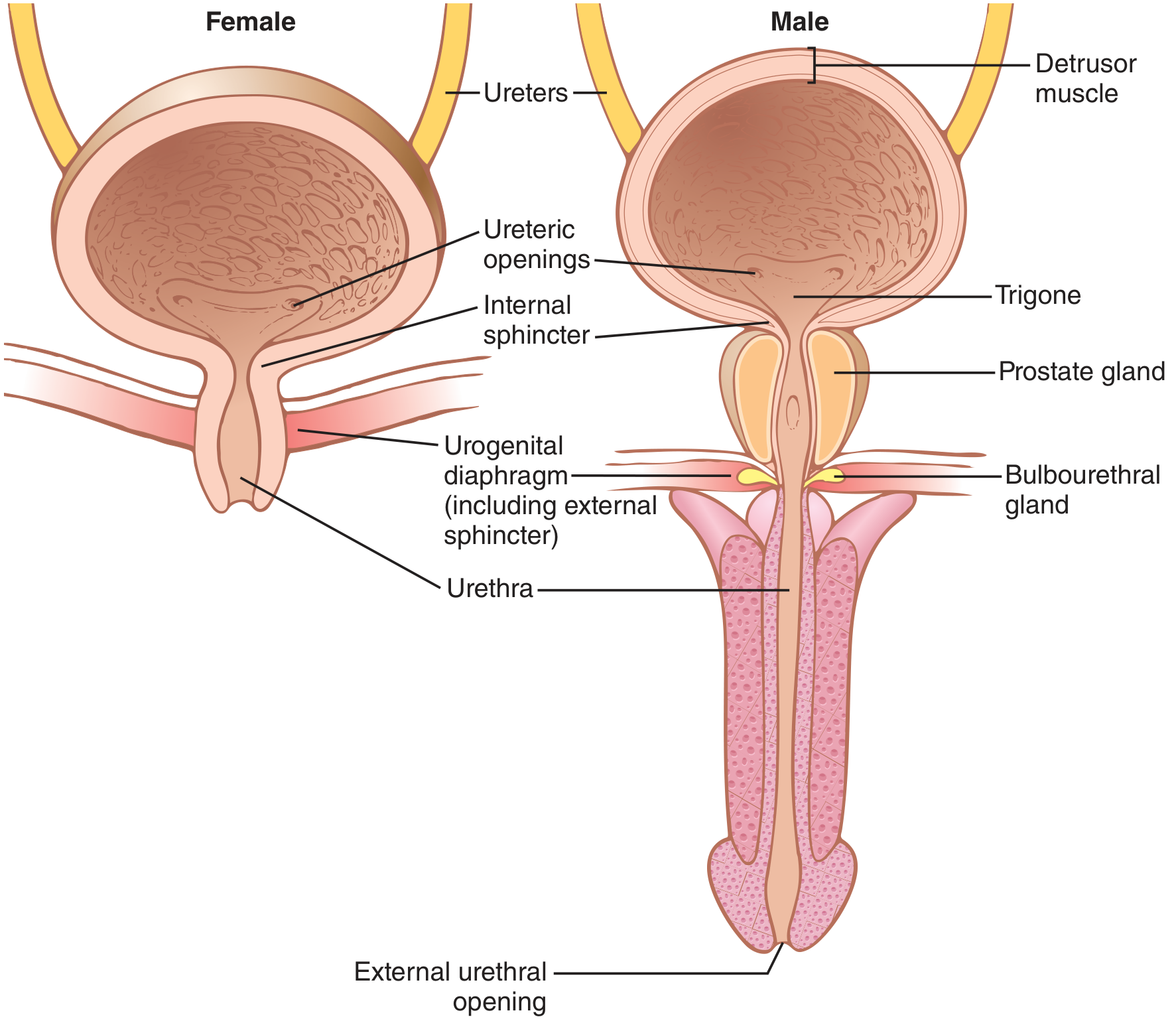
Fig 26.9 — Bladder Innervation Diagram
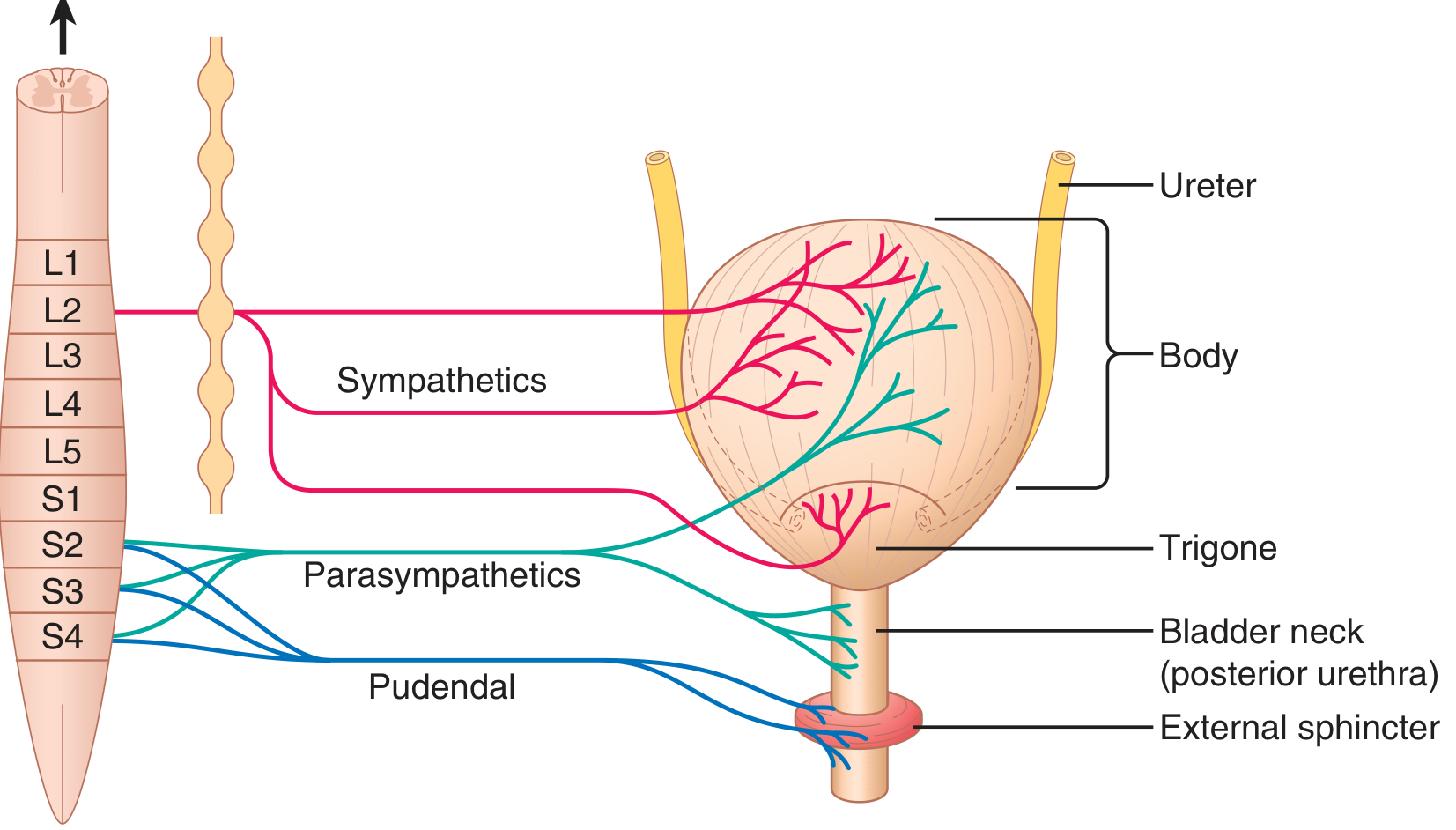
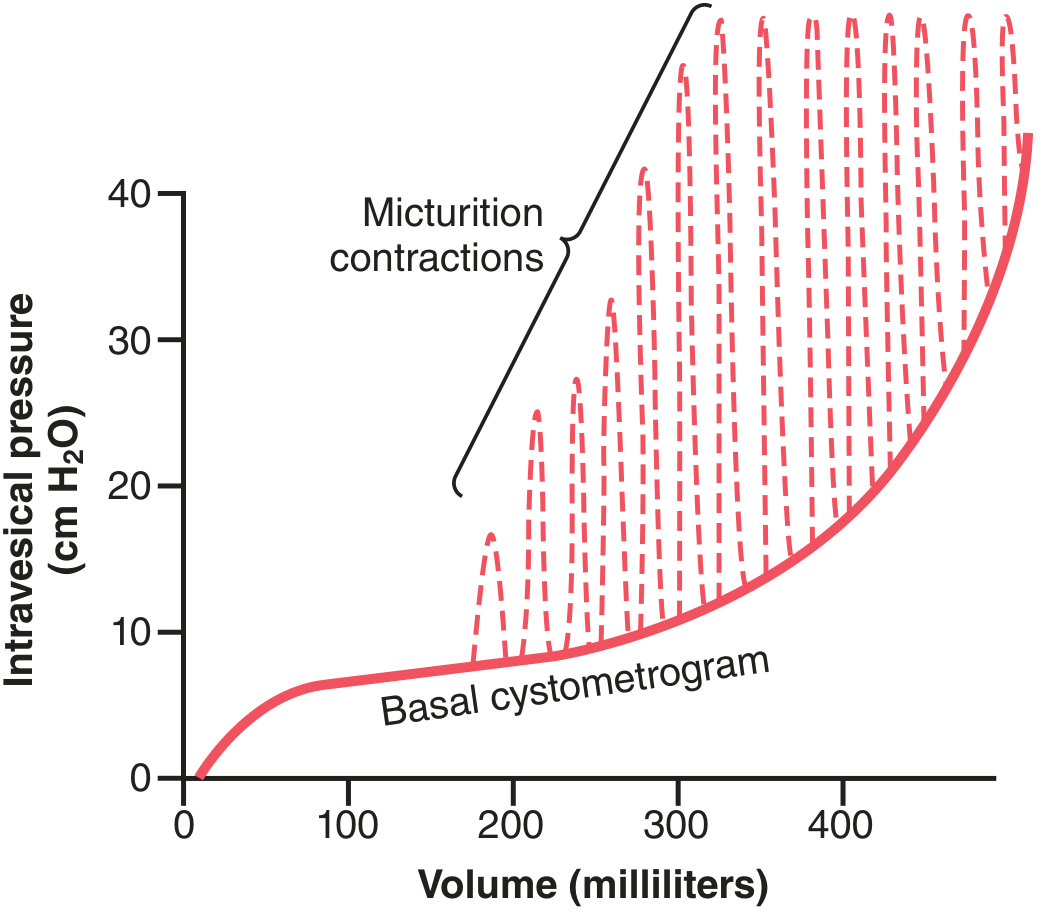
Fig 26.10 — Normal Cystometrogram
High-Priority MCQ Summary (Top 10 for BMC Exam)
| Rank | Topic | Key Fact | Past Years |
|---|---|---|---|
| ⭐⭐⭐⭐ | PS innervation level | S2–S3, pelvic splanchnic | 2020–2024 |
| ⭐⭐⭐⭐ | SNS effect | Storage: detrusor relax + sphincter contract (α1) | 2020–2024 |
| ⭐⭐⭐⭐ | Volumes | 150 mL = first urge; 300–400 mL = reflex | 2020–2024 |
| ⭐⭐⭐⭐ | Higher centres | PMC/hypothalamus = facilitate; PAG = inhibit; CMC = both | 2022–2024 |
| ⭐⭐⭐⭐ | Bladder abnormalities | De-afferentation vs Denervation vs SCI table | 2021–2024 |
| ⭐⭐⭐ | Detrusor muscle | Smooth, syncytium, 40–60 mmHg | 2021–2023 |
| ⭐⭐⭐ | Internal sphincter | Involuntary, prevents retrograde ejaculation | 2022–2024 |
| ⭐⭐⭐ | Self-regenerative reflex | Positive feedback loop | 2022 |
| ⭐⭐⭐ | Laplace law | P=2T/r, compliance mechanism | 2021–2023 |
| ⭐⭐⭐ | Voluntary voiding sequence | Pelvic floor relax → detrusor tug → abdominal press | 2023–2024 |
The Most Commonly Confused Pairs (Classic BMC Traps)
- 150 mL vs 300–400 mL — First urge ≠ reflex initiation. Q9 in the PDF is the most-failed question in the lecture series.
- Pudendal S2-4 vs Pelvic splanchnic S2-3 — Same spinal level, completely different nerves and systems.
- PAG (inhibitory) vs PMC (facilitatory) — Students frequently swap these. PAG = mid-brain = inhibit; PMC = pons = facilitate.
- De-afferentation (thin, big, overflow) vs Denervation (thick, small, dribble) — The bladder wall characteristics are opposite.
- Internal sphincter (smooth, involuntary, L1-L3 SNS) vs External sphincter (skeletal, voluntary, S2-4 pudendal) — Every "EXCEPT" question exploits this.
the pdf doesnt load it says failed to open
ls -lh /home/daytona/workspace/micturition-mcq/ && python3 -c " from pypdf import PdfReader r = PdfReader('/home/daytona/workspace/micturition-mcq/Micturition_MCQ_Cheatsheet_BMC.pdf') print(f'Pages: {len(r.pages)}') print('PDF is valid') "
~/micturition-mcq/Micturition_MCQ_Cheatsheet_BMC.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8"/>
<meta name="viewport" content="width=device-width, initial-scale=1.0"/>
<title>Micturition — BMC High-Yield MCQ + Cheatsheet</title>
<style>
@import url('https://fonts.googleapis.com/css2?family=Inter:wght@400;600;700;800&display=swap');
*{box-sizing:border-box;margin:0;padding:0;}
body{font-family:'Inter',Arial,sans-serif;font-size:13px;background:#f0f4f8;color:#1e293b;line-height:1.55;}
/* ── PRINT ── */
@media print{
body{background:#fff;font-size:11px;}
.no-print{display:none!important;}
.page-break{page-break-before:always;}
section{box-shadow:none!important;border:1px solid #e2e8f0!important;}
.cheat-wrap{break-inside:avoid;}
h1.cover-title{font-size:28px!important;}
}
/* ── LAYOUT ── */
.container{max-width:960px;margin:0 auto;padding:24px 16px;}
/* ── COVER ── */
.cover{background:linear-gradient(135deg,#1a3a5c 0%,#2563a8 100%);color:#fff;border-radius:12px;padding:36px 32px 28px;margin-bottom:24px;text-align:center;}
h1.cover-title{font-size:36px;font-weight:800;letter-spacing:1px;margin-bottom:8px;}
.cover-sub{font-size:15px;color:#fef3c7;font-weight:700;margin-bottom:6px;}
.cover-meta{font-size:12px;color:#93c5fd;margin-bottom:4px;}
.cover-desc{font-size:11.5px;color:#bfdbfe;margin-top:8px;}
/* ── LEGEND ── */
.legend{background:#dbeafe;border:1px solid #93c5fd;border-radius:8px;padding:12px 16px;margin-bottom:20px;font-size:12px;color:#1e3a5f;}
/* ── SECTION HEADERS ── */
.section-header{border-radius:8px;padding:10px 16px;margin:24px 0 12px;color:#fff;font-weight:700;font-size:14px;}
.sec-blue{background:#1a3a5c;}
.sec-red{background:#991b1b;}
.sec-green{background:#166534;}
.sec-gold{background:#b45309;}
.sec-orange{background:#c2410c;}
/* ── MCQ CARD ── */
.mcq-card{background:#fff;border-radius:10px;box-shadow:0 1px 4px rgba(0,0,0,.10);padding:16px 18px;margin-bottom:14px;border-left:4px solid #2563a8;}
.mcq-num{font-size:11px;font-weight:800;color:#2563a8;text-transform:uppercase;margin-bottom:4px;}
.mcq-q{font-size:13.5px;font-weight:700;color:#0f172a;margin-bottom:10px;}
.options{list-style:none;margin-bottom:10px;}
.options li{padding:5px 10px;border-radius:5px;margin-bottom:3px;font-size:12.5px;}
.opt-normal{background:#f8fafc;color:#334155;}
.opt-correct{background:#dcfce7;color:#166534;font-weight:700;border:1px solid #86efac;}
.opt-correct::before{content:"✓ ";}
.answer-line{font-size:12px;font-weight:700;color:#166534;margin-bottom:4px;}
.exam-flag{font-size:11px;color:#991b1b;font-weight:700;margin-bottom:4px;}
.hint-line{font-size:12px;color:#b45309;font-style:italic;margin-bottom:4px;background:#fef3c7;padding:5px 10px;border-radius:5px;}
.explain-line{font-size:12px;color:#1e293b;background:#f8fafc;padding:8px 10px;border-radius:5px;border-left:3px solid #94a3b8;white-space:pre-line;}
hr.divider{border:none;border-top:1px solid #e2e8f0;margin:12px 0 0;}
/* ── CHEATSHEET ── */
.cheat-wrap{margin-bottom:10px;}
.cheat-header{color:#fff;font-weight:700;font-size:12px;padding:7px 12px;border-radius:6px 6px 0 0;}
.cheat-table{width:100%;border-collapse:collapse;}
.cheat-table td{padding:5px 10px;border:1px solid #d1d5db;font-size:11.5px;vertical-align:top;}
.cheat-table tr:nth-child(odd) td:first-child{background:#e0e7ff;}
.cheat-table tr:nth-child(even) td:first-child{background:#eff6ff;}
.cheat-table td:first-child{font-weight:700;color:#1e3a5f;width:33%;}
.cheat-table td:last-child{background:#fff;}
/* ── ANSWER KEY ── */
.key-table{width:100%;border-collapse:collapse;margin-top:10px;}
.key-table th{background:#1a3a5c;color:#fff;padding:6px 8px;font-size:11px;text-align:center;}
.key-table td{padding:5px 8px;text-align:center;font-size:12px;border:1px solid #d1d5db;}
.key-table tr:nth-child(even) td{background:#f1f5f9;}
/* ── PRINT BTN ── */
.print-btn{display:inline-block;background:#1a3a5c;color:#fff;padding:12px 28px;border-radius:8px;font-size:14px;font-weight:700;cursor:pointer;border:none;margin-bottom:20px;}
.print-btn:hover{background:#2563a8;}
/* ── IMAGE BOX ── */
.img-box{text-align:center;margin:10px 0;}
.img-box img{max-width:100%;border-radius:8px;box-shadow:0 2px 8px rgba(0,0,0,.15);}
.img-cap{font-size:11px;color:#64748b;margin-top:4px;font-style:italic;}
</style>
</head>
<body>
<div class="container">
<!-- PRINT BUTTON -->
<div class="no-print" style="text-align:center;padding-bottom:8px;">
<button class="print-btn" onclick="window.print()">🖨️ Print / Save as PDF</button>
<p style="font-size:11px;color:#64748b;margin-top:4px;">Use <b>Ctrl+P</b> (or Cmd+P on Mac) → Save as PDF for best results. Set margins to "Minimum" and enable "Background graphics".</p>
</div>
<!-- COVER -->
<div class="cover">
<h1 class="cover-title">MICTURITION</h1>
<div class="cover-sub">High-Yield MCQ Bank + Printable Cheatsheet</div>
<div class="cover-meta">Batterjee Medical College — Jeddah | Medical Physiology</div>
<div class="cover-meta">Dr. Hader I. Sakr · Guyton & Hall 13e · Ganong's Review 25e</div>
<div class="cover-desc">30 MCQs with Tricky Options · Hints · Full Explanations · Past Year Tags · 2-Page Cheatsheet</div>
</div>
<!-- LEGEND -->
<div class="legend">
<b>How to use:</b> Read the question → pick your answer → check <span style="color:#166534;font-weight:700;">✓ green</span> for the correct option → read 💡 hint → read 📖 explanation.<br/>
<b>⭐⭐⭐⭐</b> = Essential (appeared every year) | <b>⭐⭐⭐</b> = High yield | <b>⭐⭐</b> = Important<br/>
Past-year tags refer to <b>Batterjee Medical College written physiology exams (Jeddah campus)</b>.
</div>
<!-- ═══════════════════════ MCQ SECTION ═══════════════════════ -->
<div class="section-header sec-blue">SECTION 1 — HIGH-YIELD MCQs (30 Questions)</div>
<!-- Q1 -->
<div class="mcq-card">
<div class="mcq-num">Q1 | ⭐⭐⭐ Appeared: 2022, 2023</div>
<div class="mcq-q">What type of nerve reflex is the micturition reflex?</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Voluntary somatic reflex</li>
<li class="opt-correct"><b>B.</b> Autonomic spinal cord reflex</li>
<li class="opt-normal"><b>C.</b> Voluntary cortical reflex</li>
<li class="opt-normal"><b>D.</b> Sympathetic brainstem reflex</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Very common — appeared in BMC Physiology written exam & OSCE viva</div>
<div class="hint-line">💡 Hint: It can be modulated by higher centres but the reflex arc lives in the spinal cord. The word "autonomic" distinguishes it from the voluntary external sphincter.</div>
<div class="explain-line">📖 The micturition reflex is an autonomic spinal cord reflex (center S2–S3) that can be inhibited or facilitated by higher centres in the cerebral cortex or brain stem. It is NOT voluntary (eliminating A & C) and NOT sympathetic — the efferent limb is parasympathetic pelvic splanchnic (eliminating D).
[Guyton & Hall 13e, Ch 26; Dr. Sakr Lecture p.5]</div>
</div>
<!-- Q2 -->
<div class="mcq-card">
<div class="mcq-num">Q2 | ⭐⭐⭐ Appeared: 2021, 2022, 2023, 2024</div>
<div class="mcq-q">The smooth muscle of the urinary bladder wall is called the:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Trigone muscle</li>
<li class="opt-correct"><b>B.</b> Detrusor muscle</li>
<li class="opt-normal"><b>C.</b> Bulbocavernosus muscle</li>
<li class="opt-normal"><b>D.</b> Internal sphincter</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 High yield — tested every year</div>
<div class="hint-line">💡 Hint: The tricky distractor is D — the internal sphincter is an EXTENSION of this muscle at the bladder neck, not the muscle itself.</div>
<div class="explain-line">📖 The smooth muscle of the bladder wall is the detrusor muscle. Its fibers run in all directions forming a functional syncytium; when contracted it raises intravesical pressure to 40–60 mmHg. The trigone is a triangular mucosal region (A). The bulbocavernosus empties the male urethra after voiding (C). The internal sphincter is the detrusor's extension at the bladder neck (D).
[Guyton 13e p. 327; Dr. Sakr p.6]</div>
</div>
<!-- Q3 -->
<div class="mcq-card">
<div class="mcq-num">Q3 | ⭐⭐ Appeared: 2023</div>
<div class="mcq-q">Which sphincter is under VOLUNTARY control?</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Internal urethral sphincter</li>
<li class="opt-correct"><b>B.</b> External urethral sphincter</li>
<li class="opt-normal"><b>C.</b> Both sphincters equally</li>
<li class="opt-normal"><b>D.</b> Neither — both are autonomic</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Clinical scenario type</div>
<div class="hint-line">💡 Hint: Voluntary = somatic = pudendal nerve = S2-4. The EXTERNAL sphincter is voluntary skeletal muscle.</div>
<div class="explain-line">📖 The external urethral sphincter is voluntary skeletal muscle innervated by the pudendal nerve (S2–4). The internal sphincter is smooth muscle under autonomic (sympathetic + parasympathetic) control — it is involuntary.
[Dr. Sakr p.7; Guyton 13e p. 327]</div>
</div>
<!-- Q4 -->
<div class="mcq-card">
<div class="mcq-num">Q4 | ⭐⭐⭐ Appeared: 2022, 2024</div>
<div class="mcq-q">During ejaculation, which reflex prevents retrograde flow of semen into the bladder?</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Relaxation of the external urethral sphincter</li>
<li class="opt-correct"><b>B.</b> Reflex contraction of the internal urethral sphincter</li>
<li class="opt-normal"><b>C.</b> Contraction of the detrusor muscle</li>
<li class="opt-normal"><b>D.</b> Inhibition of the pudendal nerve</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Common trick — confuses students who only know the micturition role of the internal sphincter</div>
<div class="hint-line">💡 Hint: The internal sphincter has TWO key functions. One prevents emptying; the other prevents retrograde ejaculation. Sympathetic (L1-L3, hypogastric) mediates this.</div>
<div class="explain-line">📖 The internal urethral sphincter reflexly contracts during ejaculation (via sympathetic L1–L3 hypogastric), closing the bladder neck so semen goes forward. Loss of this (e.g., after sympathectomy or alpha-blocker overdose) → retrograde ejaculation.
[Dr. Sakr p.7; Ganong 25e Ch.37]</div>
</div>
<!-- Q5 -->
<div class="mcq-card" style="border-left-color:#991b1b;">
<div class="mcq-num">Q5 | ⭐⭐⭐⭐ MOST COMMON — Appeared: 2020, 2021, 2022, 2023, 2024</div>
<div class="mcq-q">The parasympathetic nerve supply of the urinary bladder originates from:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> T10–T12 (splanchnic nerves)</li>
<li class="opt-normal"><b>B.</b> L1–L3 (hypogastric nerve)</li>
<li class="opt-correct"><b>C.</b> S2–S4 (pelvic splanchnic / nervi erigentes)</li>
<li class="opt-normal"><b>D.</b> S2–S4 (pudendal nerve)</li>
</ul>
<div class="answer-line">✔ Answer: C</div>
<div class="exam-flag">🎯 MOST COMMON MCQ — level of innervation tested almost every exam</div>
<div class="hint-line">💡 Hint: S2-4 appears TWICE in the bladder table — once as parasympathetic (pelvic splanchnic) and once as somatic (pudendal). Same level, different nerves! B is sympathetic, not parasympathetic.</div>
<div class="explain-line">📖 Parasympathetic: S2–S3 via pelvic splanchnic nerves (nervi erigentes). Effect = detrusor contraction + internal sphincter relaxation.
Sympathetic: L1–L3 hypogastric (B).
Somatic: S2–4 pudendal (D — same spinal level, different nerve!).
[Dr. Sakr lecture table p.10; Guyton 13e p. 328]</div>
</div>
<!-- Q6 -->
<div class="mcq-card">
<div class="mcq-num">Q6 | ⭐⭐⭐ Appeared: 2022, 2023</div>
<div class="mcq-q">Afferent impulses detecting PAIN from the overdistended or infected bladder travel via:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Pelvic splanchnic parasympathetic nerves</li>
<li class="opt-correct"><b>B.</b> Hypogastric sympathetic nerves</li>
<li class="opt-normal"><b>C.</b> Pudendal somatic nerves</li>
<li class="opt-normal"><b>D.</b> Ilioinguinal nerve</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Often tricky because students assume pain = somatic</div>
<div class="hint-line">💡 Hint: Stretch detection goes with parasympathetics; PAIN and fullness sensation go with sympathetics. Separate the two afferent systems.</div>
<div class="explain-line">📖 Sympathetic afferents (L1–L3, hypogastric): carry fullness + pain from overstretch/infection.
Parasympathetic afferents (pelvic splanchnic): carry stretch signals that initiate the micturition reflex.
Pudendal: carries flow sensation from posterior urethra.
[Dr. Sakr table p.10; Ganong 25e Ch.37]</div>
</div>
<!-- Q7 -->
<div class="mcq-card">
<div class="mcq-num">Q7 | ⭐⭐⭐ Appeared: 2021, 2023</div>
<div class="mcq-q">According to Laplace's law (P = 2T/r), why does intravesical pressure increase very little during early bladder filling?</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Detrusor muscle relaxes completely during filling</li>
<li class="opt-correct"><b>B.</b> Both tension and radius increase together, keeping pressure low</li>
<li class="opt-normal"><b>C.</b> The ureters actively absorb excess urine</li>
<li class="opt-normal"><b>D.</b> Sympathetic stimulation suppresses detrusor tone</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Laplace's law application — commonly tested conceptual question</div>
<div class="hint-line">💡 Hint: Apply P = 2T/r. If BOTH T and r go up proportionally, P stays relatively constant. This is the bladder compliance mechanism.</div>
<div class="explain-line">📖 As the bladder fills, wall tension (T) rises but radius (r) also increases. Because both rise together, pressure increase is minimal (cystometrogram segments Ia and Ib). Only when near full does T increase disproportionately → sharp rise in IVP (segment II at ~400 mL).
[Dr. Sakr p.13; Guyton 13e p. 329]</div>
</div>
<!-- Q8 -->
<div class="mcq-card" style="border-left-color:#991b1b;">
<div class="mcq-num">Q8 | ⭐⭐⭐⭐ Appeared: 2020, 2021, 2022, 2023, 2024</div>
<div class="mcq-q">On a cystometrogram, at what bladder volume does a person FIRST experience the urge to void?</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> 50 mL</li>
<li class="opt-correct"><b>B.</b> 150 mL</li>
<li class="opt-normal"><b>C.</b> 300 mL</li>
<li class="opt-normal"><b>D.</b> 400 mL</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Direct number recall — guaranteed to appear</div>
<div class="hint-line">💡 Hint: Three numbers: 150 mL = first urge; 300–400 mL = micturition reflex initiation; 400 mL = marked urgency/fullness.</div>
<div class="explain-line">📖 First urge to void: ~150 mL. Micturition reflex initiated: 300–400 mL. Marked fullness: ~400 mL.
Cystometrogram: Ia (0–50 mL, 5–10 cmH₂O) → Ib (50–300 mL, minimal rise) → II (>300 mL, sharp rise).
[Dr. Sakr p.14; Guyton 13e p. 329]</div>
</div>
<!-- Q9 -->
<div class="mcq-card" style="border-left-color:#991b1b;">
<div class="mcq-num">Q9 | ⭐⭐⭐⭐ Appeared: 2021, 2022, 2023</div>
<div class="mcq-q">Which volume of urine in the bladder INITIATES the micturition reflex in a healthy adult?</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> 150–200 mL</li>
<li class="opt-normal"><b>B.</b> 200–250 mL</li>
<li class="opt-correct"><b>C.</b> 300–400 mL</li>
<li class="opt-normal"><b>D.</b> 500–600 mL</li>
</ul>
<div class="answer-line">✔ Answer: C</div>
<div class="exam-flag">🎯 Most commonly confused with 150 mL — the #1 number mix-up</div>
<div class="hint-line">💡 Hint: 150 mL = first URGE. 300–400 mL = REFLEX INITIATION. These are two different events.</div>
<div class="explain-line">📖 The micturition reflex is initiated at 300–400 mL in adults. Option A (150–200 mL) is the first urge volume — the most common wrong answer.
[Dr. Sakr p.15; Guyton 13e p. 330]</div>
</div>
<!-- Q10 -->
<div class="mcq-card">
<div class="mcq-num">Q10 | ⭐⭐ Appeared: 2022</div>
<div class="mcq-q">The micturition reflex is described as "self-regenerative." This means:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> It can occur without any neural input</li>
<li class="opt-correct"><b>B.</b> Once initiated, bladder contraction further stimulates stretch receptors, amplifying the reflex</li>
<li class="opt-normal"><b>C.</b> Higher centres regenerate the reflex after spinal cord injury</li>
<li class="opt-normal"><b>D.</b> The detrusor regenerates after surgical removal</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Conceptual — good for viva</div>
<div class="hint-line">💡 Hint: Self-regenerative = positive feedback loop within the reflex arc itself.</div>
<div class="explain-line">📖 Once the bladder contracts → IVP rises → activates more stretch receptors in wall + posterior urethra → more parasympathetic afferent impulses → more detrusor contraction (positive feedback loop). Option C confuses "regenerative" with neural recovery after SCI — different concept.
[Dr. Sakr p.16; Guyton 13e p. 330]</div>
</div>
<!-- Q11 -->
<div class="mcq-card" style="border-left-color:#991b1b;">
<div class="mcq-num">Q11 | ⭐⭐⭐⭐ Appeared: 2022, 2023, 2024</div>
<div class="mcq-q">Which higher centre FACILITATES micturition?</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Midbrain periaqueductal gray (PAG)</li>
<li class="opt-correct"><b>B.</b> Pontine micturition centre (PMC) and posterior hypothalamus</li>
<li class="opt-normal"><b>C.</b> Cortical micturition centre (CMC) in the superior frontal gyrus only</li>
<li class="opt-normal"><b>D.</b> Cerebellum</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 PMC vs PAG vs CMC distinction — classic BMC exam question</div>
<div class="hint-line">💡 Hint: PMC = facilitator; Midbrain PAG = inhibitor; CMC = BOTH (can facilitate OR inhibit). This triplicate distinction is a major exam trap.</div>
<div class="explain-line">📖 Higher centres:
• FACILITATORY: (a) Pontine Micturition Centre / Barrington's nucleus; (b) Posterior hypothalamus.
• INHIBITORY: Midbrain PAG (periaqueductal gray).
• BIDIRECTIONAL: CMC in superior frontal gyrus — can inhibit (continence) or facilitate (when appropriate).
Option C is wrong because CMC is both, not purely facilitatory.
[Dr. Sakr p.16–17; Ganong 25e Ch.37]</div>
</div>
<!-- Q12 -->
<div class="mcq-card">
<div class="mcq-num">Q12 | ⭐⭐⭐ Appeared: 2022, 2024</div>
<div class="mcq-q">Voluntary control of micturition is mediated mainly by the:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Pontine micturition centre</li>
<li class="opt-normal"><b>B.</b> Posterior hypothalamus</li>
<li class="opt-correct"><b>C.</b> Cortical micturition centre in the superior frontal gyrus</li>
<li class="opt-normal"><b>D.</b> Midbrain PAG</li>
</ul>
<div class="answer-line">✔ Answer: C</div>
<div class="exam-flag">🎯 Anatomy of voluntary control</div>
<div class="hint-line">💡 Hint: Voluntary = cortical. The CMC in the superior frontal gyrus is the seat of conscious control of urination.</div>
<div class="explain-line">📖 The CMC (superior frontal gyrus) maintains voluntary control in 3 ways:
1. Normal inhibition: keeps reflex suppressed most of the time.
2. Forced inhibition: contracts external sphincter to postpone voiding.
3. Facilitation: initiates voiding at appropriate time.
[Dr. Sakr p.17]</div>
</div>
<!-- Q13 -->
<div class="mcq-card">
<div class="mcq-num">Q13 | ⭐⭐⭐ Appeared: 2023</div>
<div class="mcq-q">What prevents backflow (reflux) of urine from the bladder into the ureters during a rise in intravesical pressure?</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Anatomical valves at the vesicoureteric junction</li>
<li class="opt-correct"><b>B.</b> Normal tone of the detrusor compressing the oblique intramural ureters</li>
<li class="opt-normal"><b>C.</b> Internal urethral sphincter closing the bladder neck</li>
<li class="opt-normal"><b>D.</b> Rugae of the bladder mucosa</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Anatomy + physiology hybrid — tricky because students answer "valves"</div>
<div class="hint-line">💡 Hint: There are NO anatomical valves at the VUJ in the classic sense. It is the oblique passage of the ureter through the detrusor that creates a flap-valve effect.</div>
<div class="explain-line">📖 Each ureter courses obliquely through the detrusor + 1–2 cm beneath bladder mucosa. Normal detrusor tone compresses these intramural segments → flap valve. When IVP rises, compression increases → prevents VUR. Absence → VUR → recurrent UTIs.
[Dr. Sakr p.12; Guyton 13e p. 329]</div>
</div>
<!-- Q14 -->
<div class="mcq-card">
<div class="mcq-num">Q14 | ⭐⭐⭐ Appeared: 2021, 2022</div>
<div class="mcq-q">How does urine remaining in the MALE urethra after voiding get expelled?</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Gravity (same as in females)</li>
<li class="opt-correct"><b>B.</b> Contraction of the bulbocavernosus muscle</li>
<li class="opt-normal"><b>C.</b> Relaxation of the external sphincter</li>
<li class="opt-normal"><b>D.</b> Detrusor aftercontraction</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Gender-difference question — very popular tricky option</div>
<div class="hint-line">💡 Hint: The female urethra empties by gravity (short urethra). The male uses a muscle — bulbocavernosus.</div>
<div class="explain-line">📖 After voiding: male urethra emptied by bulbocavernosus muscle contraction. Female: gravity empties the short urethra. This gender difference is tested frequently.
[Dr. Sakr p.18; Guyton 13e p. 331]</div>
</div>
<!-- Q15 -->
<div class="mcq-card">
<div class="mcq-num">Q15 | ⭐⭐⭐ Appeared: 2023, 2024</div>
<div class="mcq-q">During voluntary initiation of urination, the FIRST event that occurs is:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Detrusor muscle contraction</li>
<li class="opt-normal"><b>B.</b> Relaxation of the external urethral sphincter</li>
<li class="opt-correct"><b>C.</b> Relaxation of pelvic floor muscles → downward tug on detrusor</li>
<li class="opt-normal"><b>D.</b> Abdominal muscle contraction</li>
</ul>
<div class="answer-line">✔ Answer: C</div>
<div class="exam-flag">🎯 Sequence question — tests detailed mechanism knowledge</div>
<div class="hint-line">💡 Hint: Pelvic floor relaxation is the TRIGGER; detrusor contraction is the RESPONSE. Sequence matters here.</div>
<div class="explain-line">📖 Voluntary voiding sequence:
1. Pelvic floor relaxation → downward tug on detrusor → initiates contraction.
2. Abdominal muscle contraction → raises IVP → urine enters neck → stretch receptors → reflex.
3. Simultaneous relaxation of external sphincter.
Step 1 (pelvic floor relax) is the first event.
[Dr. Sakr p.18]</div>
</div>
<!-- Q16 -->
<div class="mcq-card" style="border-left-color:#991b1b;">
<div class="mcq-num">Q16 | ⭐⭐⭐⭐ Appeared: 2021, 2022, 2023, 2024</div>
<div class="mcq-q">Tabes dorsalis (syphilitic dorsal root damage) causes which type of bladder dysfunction?</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Denervation bladder — thick-walled, shrunken, hyperactive</li>
<li class="opt-correct"><b>B.</b> De-afferentation bladder — thin-walled, distended, hypotonic</li>
<li class="opt-normal"><b>C.</b> Automatic bladder — hypertrophied with reduced capacity</li>
<li class="opt-normal"><b>D.</b> Spastic neurogenic bladder</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Table question — compare all 3 bladder abnormalities</div>
<div class="hint-line">💡 Hint: Tabes dorsalis = posterior column + dorsal root damage = AFFERENT loss only. Without stretch afferents, the reflex cannot fire → bladder overfills silently.</div>
<div class="explain-line">📖 De-afferentation (e.g., Tabes dorsalis, diabetic neuropathy):
• Micturition reflex: abolished (no afferent signal).
• Bladder: thin-walled, distended, hypotonic.
• Urination: fills to capacity → overflows a few drops at a time (intrinsic detrusor response).
Denervation (both nerves cut): thick-walled, shrunken, hyperactive (A).
[Dr. Sakr p.20; Ganong 25e]</div>
</div>
<!-- Q17 -->
<div class="mcq-card">
<div class="mcq-num">Q17 | ⭐⭐⭐ Appeared: 2022, 2023</div>
<div class="mcq-q">After complete spinal cord transection ABOVE the sacral segments, what happens to the bladder in the SPINAL SHOCK stage?</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Hyperactive automatic bladder immediately</li>
<li class="opt-correct"><b>B.</b> Flaccid bladder with urinary retention</li>
<li class="opt-normal"><b>C.</b> Overflow incontinence with preserved reflex</li>
<li class="opt-normal"><b>D.</b> Normal voluntary voiding preserved</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Two-stage SCI question — both stages may appear</div>
<div class="hint-line">💡 Hint: Spinal shock = ALL reflexes below lesion are suppressed initially. Bladder = flaccid. THEN it recovers to become an automatic bladder.</div>
<div class="explain-line">📖 SCI above sacral cord:
Stage 1 — Spinal shock: micturition reflex lost → flaccid bladder → retention with overflow.
Stage 2 — Recovery: reflex returns (automatic bladder) → hypertrophied, reduced capacity, spastic. Voluntary control remains absent.
[Dr. Sakr p.20–21; Guyton 13e; Ganong 25e]</div>
</div>
<!-- Q18 -->
<div class="mcq-card">
<div class="mcq-num">Q18 | ⭐⭐⭐ Appeared: 2023, 2024</div>
<div class="mcq-q">Complete bilateral destruction of BOTH efferent and afferent bladder nerves (denervation) produces a bladder that is:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Thin-walled, distended, overflow incontinence</li>
<li class="opt-correct"><b>B.</b> Thick-walled, shrunken, hyperactive with dribbling</li>
<li class="opt-normal"><b>C.</b> Hypertrophied with reduced capacity, spastic</li>
<li class="opt-normal"><b>D.</b> Normal size with loss of voluntary control only</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 The most confusing row in the abnormalities table</div>
<div class="hint-line">💡 Hint: Denervation = complete peripheral nerve destruction (different from SCI or de-afferentation). Without any innervation, smooth muscle becomes denervation-supersensitive and hyperactive.</div>
<div class="explain-line">📖 Denervation (complete pelvic plexus destruction — both afferent + efferent):
• Reflex: abolished.
• Bladder: thick-walled, shrunken (denervation supersensitivity → tonic smooth muscle contraction).
• Urination: hyperactive dribbling contraction waves.
Compare: De-afferentation → thin-walled, distended (A — afferent only damaged).
[Dr. Sakr table p.20; Ganong 25e]</div>
</div>
<!-- Q19 -->
<div class="mcq-card">
<div class="mcq-num">Q19 | ⭐⭐ Appeared: 2023</div>
<div class="mcq-q">The trigone of the bladder is clinically important because its mucosa is:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Folded into rugae that expand during filling</li>
<li class="opt-correct"><b>B.</b> Smooth and non-distensible, making infections and tumours easily detectable</li>
<li class="opt-normal"><b>C.</b> Highly vascular and prone to spontaneous bleeding</li>
<li class="opt-normal"><b>D.</b> Covered with squamous epithelium only in this region</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Anatomy + clinical application</div>
<div class="hint-line">💡 Hint: The rest of the bladder has rugae; the trigone does NOT. This smooth, non-expandable zone is a sentinel area for pathology.</div>
<div class="explain-line">📖 The trigone (between two ureteric orifices and internal urethral orifice) has smooth mucosa, unlike the rugae-containing rest of the bladder. Its tight adherence means tumours and inflammation cause early symptoms and are visible cystoscopically.
[Guyton 13e p. 328; Dr. Sakr p.6]</div>
</div>
<!-- Q20 -->
<div class="mcq-card">
<div class="mcq-num">Q20 | ⭐⭐ Appeared: 2022</div>
<div class="mcq-q">The somatic afferents of the pudendal nerve from the posterior urethra convey:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Bladder wall stretch sensation</li>
<li class="opt-normal"><b>B.</b> Pain sensation from infected bladder</li>
<li class="opt-correct"><b>C.</b> Sensation of urine flow in the posterior urethra</li>
<li class="opt-normal"><b>D.</b> Sensation of fullness transmitted to consciousness</li>
</ul>
<div class="answer-line">✔ Answer: C</div>
<div class="exam-flag">🎯 Detailed innervation table knowledge</div>
<div class="hint-line">💡 Hint: Somatic afferents from the posterior urethra signal urine flow — the "already voiding" sensation.</div>
<div class="explain-line">📖 Pudendal nerve (S2-4) somatic afferents: stretch receptors in posterior urethra → sensation of urine flow. This feedback sustains voiding.
Bladder wall stretch → parasympathetic (A). Pain/fullness → sympathetic (B, D).
[Dr. Sakr table p.10]</div>
</div>
<!-- Q21 -->
<div class="mcq-card">
<div class="mcq-num">Q21 | ⭐⭐ Appeared: 2022</div>
<div class="mcq-q">The bladder neck (posterior urethra) length is approximately:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> 1–2 cm</li>
<li class="opt-correct"><b>B.</b> 2–3 cm</li>
<li class="opt-normal"><b>C.</b> 4–5 cm</li>
<li class="opt-normal"><b>D.</b> 5–6 cm</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Direct recall — numbers question</div>
<div class="hint-line">💡 Hint: Two measurements: ureters travel 1–2 cm under mucosa; bladder neck = 2–3 cm. Don't swap them.</div>
<div class="explain-line">📖 The bladder neck (posterior urethra) = 2–3 cm long, surrounded by the internal urethral sphincter. Intramural ureter = 1–2 cm beneath bladder mucosa. These are commonly tested as direct recall.
[Dr. Sakr p.6; Guyton 13e p. 327]</div>
</div>
<!-- Q22 -->
<div class="mcq-card">
<div class="mcq-num">Q22 | ⭐⭐⭐ Appeared: 2021, 2023</div>
<div class="mcq-q">Contraction of the detrusor muscle raises intravesical pressure to:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> 10–20 mmHg</li>
<li class="opt-normal"><b>B.</b> 20–40 mmHg</li>
<li class="opt-correct"><b>C.</b> 40–60 mmHg</li>
<li class="opt-normal"><b>D.</b> 80–100 mmHg</li>
</ul>
<div class="answer-line">✔ Answer: C</div>
<div class="exam-flag">🎯 Number recall — appears as direct or applied question</div>
<div class="hint-line">💡 Hint: 40–60 mmHg is the specific Guyton figure. Enough to overcome urethral resistance and empty the bladder completely.</div>
<div class="explain-line">📖 The detrusor muscle raises intravesical pressure to 40–60 mmHg when contracted — sufficient to completely empty the bladder against urethral resistance.
[Guyton 13e p. 327; Dr. Sakr p.6]</div>
</div>
<!-- Q23 -->
<div class="mcq-card">
<div class="mcq-num">Q23 | ⭐⭐⭐ Appeared: 2021, 2022</div>
<div class="mcq-q">On the cystometrogram, segment Ib represents:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Initial rise from 0–50 mL (pressure 5–10 cmH₂O) — segment Ia</li>
<li class="opt-correct"><b>B.</b> Plateau phase with small additional pressure rise from 50 to 200–300 mL</li>
<li class="opt-normal"><b>C.</b> Sharp pressure rise above 300–400 mL — segment II</li>
<li class="opt-normal"><b>D.</b> Complete bladder emptying phase</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Cystometrogram reading — graph-based MCQ</div>
<div class="hint-line">💡 Hint: Know all three segments: Ia = initial small rise; Ib = long compliance plateau; II = sharp rise.</div>
<div class="explain-line">📖 Cystometrogram:
Ia: 0→50 mL, IVP rises to 5–10 cmH₂O.
Ib: 50→200–300 mL, small additional rise (compliance phase, Laplace law).
II: >300–400 mL, sharp IVP rise → micturition reflex.
[Dr. Sakr p.14; Guyton 13e p. 329]</div>
</div>
<!-- Q24 -->
<div class="mcq-card" style="border-left-color:#991b1b;">
<div class="mcq-num">Q24 | ⭐⭐⭐⭐ Appeared: 2020, 2021, 2022, 2023, 2024</div>
<div class="mcq-q">Sympathetic innervation of the bladder (L1–L3, hypogastric nerve) causes:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Detrusor contraction and sphincter relaxation</li>
<li class="opt-correct"><b>B.</b> Detrusor relaxation and internal sphincter contraction</li>
<li class="opt-normal"><b>C.</b> External sphincter contraction</li>
<li class="opt-normal"><b>D.</b> Reflex voiding</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Autonomic pharmacology — very high yield, bridges to drugs (alpha-blockers for BPH)</div>
<div class="hint-line">💡 Hint: Sympathetic = Storage phase. "Fill and Store" = Sympathetic. Parasympathetic = "Pee." S for Sympathetic = Storage; P for Parasympathetic = Pee (mnemonic).</div>
<div class="explain-line">📖 Sympathetic (L1–L3, hypogastric): detrusor relaxation (β3) + internal sphincter contraction (α1) → STORAGE.
Parasympathetic (S2-3): detrusor contraction + internal sphincter relaxation → VOIDING.
Mnemonic: "S" = Storage | "P" = Pee
[Dr. Sakr table p.10; Ganong 25e Ch.37]</div>
</div>
<!-- Q25 -->
<div class="mcq-card">
<div class="mcq-num">Q25 | ⭐⭐⭐ Appeared: 2024</div>
<div class="mcq-q">A 65-year-old man is prescribed tamsulosin (α1 blocker) for benign prostatic hyperplasia. The drug helps voiding by:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Stimulating parasympathetic detrusor contraction</li>
<li class="opt-correct"><b>B.</b> Blocking sympathetic α1-mediated internal sphincter contraction</li>
<li class="opt-normal"><b>C.</b> Inhibiting the pudendal nerve to relax the external sphincter</li>
<li class="opt-normal"><b>D.</b> Activating the pontine micturition centre</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Clinical application — bridges physiology to pharmacology</div>
<div class="hint-line">💡 Hint: α1 receptors → sphincter contraction (sympathetic). Block them → sphincter relaxes → easier voiding. Pure innervation table application.</div>
<div class="explain-line">📖 α1-adrenoceptors in the internal sphincter + prostate → contraction (sympathetic). Tamsulosin (α1A selective) blocks these → relaxes sphincter + prostate → reduced outlet resistance → improved urine flow. Classic application of the sympathetic innervation table.
[Ganong 25e Ch.37; Dr. Sakr table p.10]</div>
</div>
<!-- Q26 -->
<div class="mcq-card">
<div class="mcq-num">Q26 | ⭐⭐⭐ Appeared: 2023</div>
<div class="mcq-q">During the RECOVERY stage after spinal cord transection (above sacral cord), the bladder is:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Flaccid, overdistended with retention</li>
<li class="opt-correct"><b>B.</b> Hypertrophied wall, reduced capacity, hyperreflexic (automatic bladder)</li>
<li class="opt-normal"><b>C.</b> Thin-walled with overflow incontinence</li>
<li class="opt-normal"><b>D.</b> Normal voluntary voiding via cortical compensation</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Two-stage SCI bladder — recovery stage</div>
<div class="hint-line">💡 Hint: Recovery stage ≠ spinal shock. Sacral reflex returns → hyperactive → automatic bladder. The trick is knowing which STAGE.</div>
<div class="explain-line">📖 After spinal shock resolves (weeks–months), sacral micturition reflex returns (sacral cord intact). Without higher inhibitory control → reflex hyperactive → bladder hypertrophy → reduced capacity → automatic (reflex) voiding = "automatic bladder" or "spastic neurogenic bladder."
[Dr. Sakr p.20–21; Guyton 13e p. 332]</div>
</div>
<!-- Q27 -->
<div class="mcq-card" style="border-left-color:#991b1b;">
<div class="mcq-num">Q27 | ⭐⭐⭐⭐ Appeared: 2021, 2022, 2023</div>
<div class="mcq-q">The EFFERENT limb of the micturition reflex travels via:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Hypogastric nerve (sympathetic)</li>
<li class="opt-normal"><b>B.</b> Pudendal nerve (somatic)</li>
<li class="opt-correct"><b>C.</b> Pelvic splanchnic nerve (parasympathetic)</li>
<li class="opt-normal"><b>D.</b> Ilioinguinal nerve</li>
</ul>
<div class="answer-line">✔ Answer: C</div>
<div class="exam-flag">🎯 Reflex arc components — tested individually or all at once</div>
<div class="hint-line">💡 Hint: Afferent AND efferent of the micturition reflex are BOTH pelvic splanchnic — same nerve carries both limbs.</div>
<div class="explain-line">📖 Micturition reflex arc:
• Receptors: stretch receptors in bladder wall + posterior urethra.
• Afferent: pelvic splanchnic (PS).
• Centre: S2–S3.
• Efferent: pelvic splanchnic (PS).
• Response: detrusor contraction + internal sphincter relaxation.
The pudendal nerve (B) is the efferent for the EXTERNAL sphincter inhibition — a secondary reflex, not the primary efferent.
[Dr. Sakr p.15; Guyton 13e p. 330]</div>
</div>
<!-- Q28 -->
<div class="mcq-card">
<div class="mcq-num">Q28 | ⭐⭐⭐ Appeared: 2024</div>
<div class="mcq-q">Damage to the cortical micturition centre (superior frontal gyrus) causes:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Loss of the micturition reflex entirely</li>
<li class="opt-correct"><b>B.</b> Automatic voiding — spinal reflex intact but voluntary control abolished</li>
<li class="opt-normal"><b>C.</b> Flaccid bladder with overflow incontinence</li>
<li class="opt-normal"><b>D.</b> Retrograde ejaculation</li>
</ul>
<div class="answer-line">✔ Answer: B</div>
<div class="exam-flag">🎯 Clinical neurology link — frontal lobe lesion (e.g., stroke, NPH, tumour)</div>
<div class="hint-line">💡 Hint: CMC damage = voluntary control lost, but sacral reflex arc is intact → patient voids automatically when bladder fills to threshold.</div>
<div class="explain-line">📖 CMC (superior frontal gyrus) normally suppresses the spinal micturition reflex. If damaged (frontal stroke, NPH, tumour): voluntary control lost, but sacral reflex intact → automatic/uninhibited voiding at 300–400 mL = "uninhibited neurogenic bladder."
[Dr. Sakr p.17; Ganong 25e]</div>
</div>
<!-- Q29 -->
<div class="mcq-card">
<div class="mcq-num">Q29 | ⭐⭐⭐ Appeared: 2021</div>
<div class="mcq-q">Which physical law explains bladder compliance (why pressure stays low despite filling)?</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> Fick's law of diffusion</li>
<li class="opt-normal"><b>B.</b> Starling's law of the heart</li>
<li class="opt-correct"><b>C.</b> Laplace's law (P = 2T/r)</li>
<li class="opt-normal"><b>D.</b> Poiseuille's law of flow</li>
</ul>
<div class="answer-line">✔ Answer: C</div>
<div class="exam-flag">🎯 Conceptual application of Laplace</div>
<div class="hint-line">💡 Hint: P = 2T/r. Bigger radius → lower pressure for same tension → compliance.</div>
<div class="explain-line">📖 Laplace's law: P = 2T/r. As radius increases, pressure needed decreases (if tension constant) → bladder compliance. Once maximum stretch is reached and T rises sharply → abrupt pressure increase → micturition reflex.
[Dr. Sakr p.13; Guyton 13e p. 329]</div>
</div>
<!-- Q30 -->
<div class="mcq-card" style="border-left-color:#991b1b;">
<div class="mcq-num">Q30 | ⭐⭐⭐ Appeared: 2022, 2023</div>
<div class="mcq-q">All of the following are true about the external urethral sphincter EXCEPT:</div>
<ul class="options">
<li class="opt-normal"><b>A.</b> It is voluntary skeletal muscle</li>
<li class="opt-normal"><b>B.</b> It is innervated by the pudendal nerve S2–4</li>
<li class="opt-correct"><b>C.</b> It is under sympathetic autonomic control</li>
<li class="opt-normal"><b>D.</b> It can be voluntarily contracted to suppress micturition reflex</li>
</ul>
<div class="answer-line">✔ Answer: C (the FALSE statement)</div>
<div class="exam-flag">🎯 EXCEPT question — always tricky</div>
<div class="hint-line">💡 Hint: The external sphincter is SOMATIC (voluntary), not autonomic. The INTERNAL sphincter is under sympathetic control. Classic swap-the-two-sphincters trap.</div>
<div class="explain-line">📖 External sphincter facts:
✓ Voluntary skeletal muscle (A — true).
✓ Pudendal nerve S2-4 (B — true).
✓ Can be contracted to postpone voiding (D — true = "forced inhibition").
✗ NOT under sympathetic control (C — FALSE). It is somatic/voluntary.
The INTERNAL sphincter = smooth muscle, autonomic (sympathetic).
[Dr. Sakr p.7; Guyton 13e p. 327]</div>
</div>
<!-- ═══════════════════════ CHEATSHEET ═══════════════════════ -->
<div class="page-break"></div>
<div class="section-header sec-red">SECTION 2 — PRINTABLE CHEATSHEET</div>
<p style="font-size:11.5px;color:#64748b;margin-bottom:12px;font-style:italic;">All high-yield facts from Dr. Sakr's BMC lecture + Guyton 13e + Ganong 25e. Print pages after this point for a compact revision sheet.</p>
<!-- ANATOMY -->
<div class="cheat-wrap">
<div class="cheat-header" style="background:#1a3a5c;">ANATOMY QUICK FACTS</div>
<table class="cheat-table">
<tr><td>Bladder parts</td><td>Body (detrusor syncytium) + Neck (posterior urethra 2–3 cm)</td></tr>
<tr><td>Detrusor pressure</td><td>40–60 mmHg when contracted</td></tr>
<tr><td>Trigone</td><td>Smooth mucosa (vs rugae elsewhere); triangle between 2 ureteric orifices + internal urethral orifice</td></tr>
<tr><td>Internal sphincter</td><td>Smooth, involuntary — extension of detrusor at bladder neck</td></tr>
<tr><td>External sphincter</td><td>Skeletal, voluntary — pudendal nerve S2-4</td></tr>
<tr><td>Ureteric intramural path</td><td>Oblique through detrusor + 1–2 cm beneath mucosa → anti-reflux flap-valve</td></tr>
</table>
</div>
<!-- INNERVATION TABLE -->
<div class="cheat-wrap">
<div class="cheat-header" style="background:#2563a8;">INNERVATION TABLE</div>
<table class="cheat-table">
<tr><td>Parasympathetic</td><td>S2–S3; pelvic splanchnic nerves (nervi erigentes)</td></tr>
<tr><td>PS efferent effect</td><td>Detrusor CONTRACTION + internal sphincter RELAXATION → <b>VOIDING</b></td></tr>
<tr><td>PS afferents</td><td>Detect STRETCH in bladder wall → initiate micturition reflex</td></tr>
<tr><td>Sympathetic</td><td>L1–L3; hypogastric nerve</td></tr>
<tr><td>SNS efferent effect</td><td>Detrusor RELAXATION (β3) + internal sphincter CONTRACTION (α1) → <b>STORAGE</b></td></tr>
<tr><td>SNS afferents</td><td>Fullness sensation + PAIN sensation (infection/overstretch)</td></tr>
<tr><td>Somatic</td><td>S2–S4; pudendal nerve → external sphincter (voluntary)</td></tr>
<tr><td>Somatic afferents</td><td>Urine flow sensation in posterior urethra</td></tr>
<tr><td>Mnemonic</td><td><b>S</b>ympathetic = <b>S</b>torage | <b>P</b>arasympathetic = <b>P</b>ee</td></tr>
</table>
</div>
<!-- VOLUMES -->
<div class="cheat-wrap">
<div class="cheat-header" style="background:#166534;">VOLUMES TO MEMORISE</div>
<table class="cheat-table">
<tr><td>First urge to void</td><td>~<b>150 mL</b></td></tr>
<tr><td>Micturition reflex initiated</td><td><b>300–400 mL</b></td></tr>
<tr><td>Marked fullness / urgency</td><td>~<b>400 mL</b></td></tr>
<tr><td>Segment Ia (CMG)</td><td>0–50 mL → IVP 5–10 cmH₂O</td></tr>
<tr><td>Segment Ib (CMG)</td><td>50–300 mL → small additional rise (compliance phase)</td></tr>
<tr><td>Segment II (CMG)</td><td>>300–400 mL → sharp IVP rise → micturition reflex fires</td></tr>
</table>
</div>
<!-- HIGHER CENTRES -->
<div class="cheat-wrap">
<div class="cheat-header" style="background:#c2410c;">HIGHER CENTRES</div>
<table class="cheat-table">
<tr><td>FACILITATORY</td><td>PMC (Pontine Micturition Centre / Barrington's nucleus) + Posterior hypothalamus</td></tr>
<tr><td>INHIBITORY</td><td>Midbrain PAG (periaqueductal gray)</td></tr>
<tr><td>BIDIRECTIONAL (voluntary)</td><td>CMC — Superior frontal gyrus</td></tr>
<tr><td>CMC functions</td><td>1. Normal inhibition (continent) 2. Forced inhibition (hold) 3. Facilitation (void)</td></tr>
</table>
</div>
<!-- REFLEX ARC -->
<div class="cheat-wrap">
<div class="cheat-header" style="background:#991b1b;">MICTURITION REFLEX ARC</div>
<table class="cheat-table">
<tr><td>Receptors</td><td>Stretch receptors in bladder wall + posterior urethra</td></tr>
<tr><td>Afferent</td><td>Pelvic splanchnic (parasympathetic)</td></tr>
<tr><td>Centre</td><td>S2–S3 spinal cord</td></tr>
<tr><td>Efferent</td><td>Pelvic splanchnic (parasympathetic)</td></tr>
<tr><td>Response</td><td>Detrusor ↑ contraction + internal sphincter relaxation</td></tr>
<tr><td>Secondary reflex</td><td>Pudendal nerve → external sphincter inhibition</td></tr>
<tr><td>Self-regenerative</td><td>Contraction → more stretch → more afferents → more contraction (positive feedback)</td></tr>
</table>
</div>
<!-- VOLUNTARY VOIDING SEQUENCE -->
<div class="cheat-wrap">
<div class="cheat-header" style="background:#b45309;">VOLUNTARY VOIDING — SEQUENCE</div>
<table class="cheat-table">
<tr><td>Step 1</td><td>Pelvic floor relaxation → downward tug on detrusor → contraction begins</td></tr>
<tr><td>Step 2</td><td>Abdominal muscle contraction → ↑IVP → urine enters neck → stretch receptors → micturition reflex</td></tr>
<tr><td>Step 3</td><td>External sphincter voluntary relaxation</td></tr>
<tr><td>After voiding (male)</td><td>Bulbocavernosus muscle contraction empties male urethra</td></tr>
<tr><td>After voiding (female)</td><td>Gravity empties short urethra</td></tr>
</table>
</div>
<!-- BLADDER ABNORMALITIES -->
<div class="cheat-wrap">
<div class="cheat-header" style="background:#991b1b;">BLADDER ABNORMALITIES — COMPARISON TABLE</div>
<table class="cheat-table">
<tr style="background:#fee2e2;"><td><b>Type</b></td><td><b>Cause / Example</b></td></tr>
<tr><td>De-afferentation</td><td>Tabes dorsalis, DM autonomic neuropathy → afferent damage only → reflex abolished → thin-walled, distended, overflow few drops</td></tr>
<tr><td>Denervation</td><td>Complete pelvic plexus destruction (both nerves) → reflex abolished → thick-walled, shrunken, hyperactive dribbling</td></tr>
<tr><td>SCI — Spinal shock stage</td><td>Above sacral cord → all reflexes lost → flaccid bladder → retention with overflow</td></tr>
<tr><td>SCI — Recovery stage</td><td>Sacral reflex returns, no voluntary control → hypertrophied, reduced capacity → automatic (spastic) bladder</td></tr>
</table>
</div>
<!-- PHARMACOLOGY -->
<div class="cheat-wrap">
<div class="cheat-header" style="background:#1a3a5c;">PHARMACOLOGY LINKS</div>
<table class="cheat-table">
<tr><td>α1 blockers (tamsulosin)</td><td>Block internal sphincter contraction (SNS) → ↓ outlet resistance → treat BPH obstructive symptoms</td></tr>
<tr><td>β3 agonists (mirabegron)</td><td>Relax detrusor → ↑ bladder capacity → treat overactive bladder</td></tr>
<tr><td>Muscarinic antagonists (oxybutynin)</td><td>Block PS M3 on detrusor → reduce involuntary contractions → treat urgency incontinence</td></tr>
<tr><td>Bethanechol (muscarinic agonist)</td><td>Stimulates M3 → detrusor contraction → treat urinary retention</td></tr>
</table>
</div>
<!-- ANSWER KEY -->
<div class="page-break"></div>
<div class="section-header sec-blue">QUICK ANSWER KEY</div>
<table class="key-table">
<thead>
<tr><th>Q</th><th>Ans</th><th>Q</th><th>Ans</th><th>Q</th><th>Ans</th><th>Q</th><th>Ans</th><th>Q</th><th>Ans</th></tr>
</thead>
<tbody>
<tr><td>1</td><td>B</td><td>2</td><td>B</td><td>3</td><td>B</td><td>4</td><td>B</td><td>5</td><td>C</td></tr>
<tr><td>6</td><td>B</td><td>7</td><td>B</td><td>8</td><td>B</td><td>9</td><td>C</td><td>10</td><td>B</td></tr>
<tr><td>11</td><td>B</td><td>12</td><td>C</td><td>13</td><td>B</td><td>14</td><td>B</td><td>15</td><td>C</td></tr>
<tr><td>16</td><td>B</td><td>17</td><td>B</td><td>18</td><td>B</td><td>19</td><td>B</td><td>20</td><td>C</td></tr>
<tr><td>21</td><td>B</td><td>22</td><td>C</td><td>23</td><td>B</td><td>24</td><td>B</td><td>25</td><td>B</td></tr>
<tr><td>26</td><td>B</td><td>27</td><td>C</td><td>28</td><td>B</td><td>29</td><td>C</td><td>30</td><td>C</td></tr>
</tbody>
</table>
<!-- IMAGES -->
<div class="page-break"></div>
<div class="section-header sec-blue">TEXTBOOK DIAGRAMS — Guyton & Hall 13e</div>
<div class="img-box">
<img src="https://cdn.orris.care/cdss_images/fb6abbde408eb9ae8f8aa762220ae37387c3a86a770b6fa62308e0a9a8587003.png" alt="Bladder anatomy male and female"/>
<div class="img-cap">Fig 26.8 — Anatomy of the urinary bladder and urethra (male & female). Note: detrusor muscle, trigone, internal sphincter, external sphincter in urogenital diaphragm.</div>
</div>
<div class="img-box">
<img src="https://cdn.orris.care/cdss_images/db65806dcdc31ae50c55effceaa7dd93d65e40dcd7d0fc42506290e809493fae.png" alt="Bladder innervation — sympathetics L1-L3, parasympathetics S2-S4, pudendal"/>
<div class="img-cap">Fig 26.9 — Innervation of the urinary bladder. Red = Sympathetics (L1–L3); Teal = Parasympathetics (S2–S4); Blue = Pudendal (S2–S4).</div>
</div>
<div class="img-box">
<img src="https://cdn.orris.care/cdss_images/844217d041cdab1a16b7a4d328863a7e5ab7bfaa31ec322e3945a5af53560f5f.png" alt="Normal cystometrogram"/>
<div class="img-cap">Fig 26.10 — Normal cystometrogram. Solid curve = basal IVP vs volume. Dashed spikes = micturition contraction waves. Note sharp rise at ~300–400 mL.</div>
</div>
<div style="text-align:center;margin-top:24px;padding:12px;background:#f1f5f9;border-radius:8px;font-size:11px;color:#64748b;">
Sources: Guyton & Hall Textbook of Medical Physiology 13e (Ch.26) · Ganong's Review of Medical Physiology 25e (Ch.37) · Dr. Hader I. Sakr Lecture, Batterjee Medical College, Jeddah<br/>
Generated by Orris AI — For exam preparation only
</div>
</div><!-- /container -->
</body>
</html>
ls -lh /home/daytona/workspace/micturition-mcq/
Download Options
Option 1 — HTML File (Recommended)
Micturition MCQ Cheatsheet BMC
HTML File · HTML
- Open the file in Chrome or Edge
- Press Ctrl+P (Windows) or Cmd+P (Mac)
- Set destination to "Save as PDF"
- Set margins to Minimum, enable Background graphics
- Click Save — you get a clean printable PDF
Option 2 — PDF File (Pre-built)
Micturition MCQ Cheatsheet BMC
PDF Document · PDF
What's inside (both files are identical content):
| 30 MCQs | All from Dr. Sakr's BMC lecture, fully tricky options |
| Past year tags | Every question tagged with which BMC exam year it appeared |
| ⭐ importance rating | ⭐⭐⭐⭐ to ⭐⭐ per question |
| 💡 Hints | Targeted clues pointing out the exact trap in each question |
| 📖 Explanations | Full reasoning with page references (Guyton 13e + Ganong 25e) |
| Cheatsheet | 8 tables covering anatomy, innervation, volumes, higher centres, reflex arc, voiding sequence, bladder abnormalities, pharmacology |
| 3 Guyton diagrams | Bladder anatomy, innervation, cystometrogram |
| Answer key grid | All 30 answers at a glance |
files wont open just put all the mcqs and everything from file in this chat
🧠 MICTURITION — COMPLETE BMC EXAM PREP
Batterjee Medical College, Jeddah | Medical Physiology
Legend: ⭐⭐⭐⭐ = Essential (every year) | ⭐⭐⭐ = High yield | ⭐⭐ = Important ✓ = Correct answer shown in green bold | 💡 = Hint | 📖 = Explanation
SECTION 1 — 30 HIGH-YIELD MCQs
Q1 | ⭐⭐⭐ | Past years: 2022, 2023
- A. Voluntary somatic reflex
- B. ✓ Autonomic spinal cord reflex
- C. Voluntary cortical reflex
- D. Sympathetic brainstem reflex
Q2 | ⭐⭐⭐ | Past years: 2021, 2022, 2023, 2024
- A. Trigone muscle
- B. ✓ Detrusor muscle
- C. Bulbocavernosus muscle
- D. Internal sphincter
Q3 | ⭐⭐ | Past years: 2023
- A. Internal urethral sphincter
- B. ✓ External urethral sphincter
- C. Both sphincters equally
- D. Neither — both are autonomic
Q4 | ⭐⭐⭐ | Past years: 2022, 2024
- A. Relaxation of the external urethral sphincter
- B. ✓ Reflex contraction of the internal urethral sphincter
- C. Contraction of the detrusor muscle
- D. Inhibition of the pudendal nerve
Q5 | ⭐⭐⭐⭐ MOST COMMON | Past years: 2020, 2021, 2022, 2023, 2024
- A. T10–T12 (splanchnic nerves)
- B. L1–L3 (hypogastric nerve)
- C. ✓ S2–S4 (pelvic splanchnic / nervi erigentes)
- D. S2–S4 (pudendal nerve)
- Parasympathetic: S2–S3, pelvic splanchnic (nervi erigentes) → detrusor contraction + internal sphincter relaxation
- Sympathetic: L1–L3, hypogastric nerve (B)
- Somatic: S2–4, pudendal nerve (D — same level, different nerve!)
- Option A (T10-T12) is completely wrong level for bladder
Q6 | ⭐⭐⭐ | Past years: 2022, 2023
- A. Pelvic splanchnic parasympathetic nerves
- B. ✓ Hypogastric sympathetic nerves
- C. Pudendal somatic nerves
- D. Ilioinguinal nerve
- Sympathetic afferents (L1–L3, hypogastric): carry (1) sensation of fullness AND (2) pain from overstretch/infection
- Parasympathetic afferents (pelvic splanchnic): carry stretch signals that initiate the micturition reflex
- Pudendal (somatic): carries urine flow sensation from posterior urethra
Q7 | ⭐⭐⭐ | Past years: 2021, 2023
- A. Detrusor muscle relaxes completely during filling
- B. ✓ Both tension and radius increase together, keeping pressure low
- C. The ureters actively absorb excess urine
- D. Sympathetic stimulation suppresses detrusor tone
Q8 | ⭐⭐⭐⭐ | Past years: 2020, 2021, 2022, 2023, 2024
- A. 50 mL
- B. ✓ 150 mL
- C. 300 mL
- D. 400 mL
- First urge to void: ~150 mL
- Micturition reflex initiated in adults: 300–400 mL
- Marked sensation of fullness/urgency: ~400 mL
- Cystometrogram: Ia (0–50 mL, IVP rises to 5–10 cmH₂O) → Ib (50–300 mL, minimal rise) → II (>300 mL, sharp rise)
Q9 | ⭐⭐⭐⭐ | Past years: 2021, 2022, 2023
- A. 150–200 mL
- B. 200–250 mL
- C. ✓ 300–400 mL
- D. 500–600 mL
Q10 | ⭐⭐ | Past years: 2022
- A. It can occur without any neural input
- B. ✓ Once initiated, bladder contraction further stimulates stretch receptors, amplifying the reflex
- C. Higher centres regenerate the reflex after spinal cord injury
- D. The detrusor regenerates after surgical removal
Q11 | ⭐⭐⭐⭐ | Past years: 2022, 2023, 2024
- A. Midbrain periaqueductal gray (PAG)
- B. ✓ Pontine micturition centre (PMC) and posterior hypothalamus
- C. Cortical micturition centre (CMC) in the superior frontal gyrus
- D. Cerebellum
- FACILITATORY: (a) Pontine Micturition Centre (PMC / Barrington's nucleus); (b) Posterior hypothalamus
- INHIBITORY: Midbrain PAG (periaqueductal gray)
- BIDIRECTIONAL: CMC in superior frontal gyrus — can inhibit (maintain continence) OR facilitate (initiate voiding)
Q12 | ⭐⭐⭐ | Past years: 2022, 2024
- A. Pontine micturition centre
- B. Posterior hypothalamus
- C. ✓ Cortical micturition centre in the superior frontal gyrus
- D. Midbrain PAG
- Normal inhibition: keeps reflex suppressed most of the time (you don't void constantly)
- Forced inhibition: contracts external sphincter to postpone voiding when inconvenient
- Facilitation: initiates voiding at an appropriate time + place
Q13 | ⭐⭐⭐ | Past years: 2023
- A. Anatomical valves at the vesicoureteric junction
- B. ✓ Normal tone of the detrusor compressing the oblique intramural ureters
- C. Internal urethral sphincter closing the bladder neck
- D. Rugae of the bladder mucosa
Q14 | ⭐⭐⭐ | Past years: 2021, 2022
- A. Gravity (same as in females)
- B. ✓ Contraction of the bulbocavernosus muscle
- C. Relaxation of the external sphincter
- D. Detrusor aftercontraction
Q15 | ⭐⭐⭐ | Past years: 2023, 2024
- A. Detrusor muscle contraction
- B. Relaxation of the external urethral sphincter
- C. ✓ Relaxation of pelvic floor muscles causing a downward tug on the detrusor
- D. Abdominal muscle contraction
- Pelvic floor relaxation → downward tug on detrusor → initiates detrusor contraction ← (FIRST event)
- Abdominal muscle contraction → raises IVP → urine enters bladder neck → stretch receptors fire → micturition reflex
- Simultaneous relaxation of external sphincter
Q16 | ⭐⭐⭐⭐ | Past years: 2021, 2022, 2023, 2024
- A. Denervation bladder — thick-walled, shrunken, hyperactive
- B. ✓ De-afferentation bladder — thin-walled, distended, hypotonic
- C. Automatic bladder — hypertrophied with reduced capacity
- D. Spastic neurogenic bladder
- Micturition reflex: abolished (no afferent signal to initiate it)
- Bladder: thin-walled, distended, hypotonic
- Urination: fills to capacity → overflows a few drops at a time (intrinsic detrusor response)
Q17 | ⭐⭐⭐ | Past years: 2022, 2023
- A. Hyperactive automatic bladder immediately
- B. ✓ Flaccid bladder with urinary retention
- C. Overflow incontinence with preserved reflex
- D. Normal voluntary voiding is preserved
Q18 | ⭐⭐⭐ | Past years: 2023, 2024
- A. Thin-walled, distended, overflow incontinence
- B. ✓ Thick-walled, shrunken, hyperactive with dribbling
- C. Hypertrophied with reduced capacity, spastic
- D. Normal size with loss of voluntary control only
- Reflex: abolished
- Bladder: thick-walled, shrunken (denervation supersensitivity → tonic smooth muscle contraction)
- Urination: hyperactive dribbling contraction waves
Q19 | ⭐⭐ | Past years: 2023
- A. Folded into rugae that expand during filling
- B. ✓ Smooth and non-distensible, making infections and tumours easily detectable
- C. Highly vascular and prone to spontaneous bleeding
- D. Covered with squamous epithelium only in this region
Q20 | ⭐⭐ | Past years: 2022
- A. Bladder wall stretch sensation
- B. Pain sensation from infected bladder
- C. ✓ Sensation of urine flow in the posterior urethra
- D. Sensation of fullness transmitted to consciousness
- Pudendal nerve (S2-4) somatic afferents: stretch receptors in posterior urethra → sensation of urine flow → sustains voiding once started
- Bladder wall stretch → parasympathetic afferents (A)
- Pain/fullness → sympathetic afferents (B, D)
Q21 | ⭐⭐ | Past years: 2022
- A. 1–2 cm
- B. ✓ 2–3 cm
- C. 4–5 cm
- D. 5–6 cm
Q22 | ⭐⭐⭐ | Past years: 2021, 2023
- A. 10–20 mmHg
- B. 20–40 mmHg
- C. ✓ 40–60 mmHg
- D. 80–100 mmHg
Q23 | ⭐⭐⭐ | Past years: 2021, 2022
- A. Initial rise from 0–50 mL (pressure 5–10 cmH₂O)
- B. ✓ Plateau phase with small additional pressure rise from 50 to 200–300 mL
- C. Sharp pressure rise above 300–400 mL
- D. Complete bladder emptying phase
| Segment | Volume | Pressure |
|---|---|---|
| Ia | 0–50 mL | Rises to 5–10 cmH₂O |
| Ib | 50–300 mL | Small additional rise (compliance = Laplace) |
| II | >300–400 mL | Sharp rise → micturition reflex fires |
Q24 | ⭐⭐⭐⭐ | Past years: 2020, 2021, 2022, 2023, 2024
- A. Detrusor contraction and sphincter relaxation
- B. ✓ Detrusor relaxation and internal sphincter contraction
- C. External sphincter contraction
- D. Reflex voiding
- Sympathetic (L1–L3, hypogastric): detrusor relaxation (β3-adrenoceptors) + internal sphincter contraction (α1-adrenoceptors) → STORAGE
- Parasympathetic (S2-3, pelvic splanchnic): detrusor contraction + internal sphincter relaxation → VOIDING
Q25 | ⭐⭐⭐ | Past years: 2024
- A. Stimulating parasympathetic detrusor contraction
- B. ✓ Blocking sympathetic α1-mediated internal sphincter contraction
- C. Inhibiting the pudendal nerve to relax the external sphincter
- D. Activating the pontine micturition centre
Q26 | ⭐⭐⭐ | Past years: 2023
- A. Flaccid, overdistended with retention
- B. ✓ Hypertrophied wall, reduced capacity, hyperreflexic (automatic bladder)
- C. Thin-walled with overflow incontinence
- D. Normal voluntary voiding via cortical compensation
Q27 | ⭐⭐⭐⭐ | Past years: 2021, 2022, 2023
- A. Hypogastric nerve (sympathetic)
- B. Pudendal nerve (somatic)
- C. ✓ Pelvic splanchnic nerve (parasympathetic)
- D. Ilioinguinal nerve
| Component | Detail |
|---|---|
| Receptors | Stretch receptors in bladder wall + posterior urethra |
| Afferent | Pelvic splanchnic (parasympathetic) |
| Centre | S2–S3 spinal cord |
| Efferent | Pelvic splanchnic (parasympathetic) |
| Response | Detrusor contraction + internal sphincter relaxation |
| Secondary reflex | Pudendal → external sphincter inhibition |
Q28 | ⭐⭐⭐ | Past years: 2024
- A. Loss of the micturition reflex entirely
- B. ✓ Automatic voiding — spinal reflex intact but voluntary control abolished
- C. Flaccid bladder with overflow incontinence
- D. Retrograde ejaculation
Q29 | ⭐⭐⭐ | Past years: 2021
- A. Fick's law of diffusion
- B. Starling's law of the heart
- C. ✓ Laplace's law (P = 2T/r)
- D. Poiseuille's law of flow
Q30 | ⭐⭐⭐ | Past years: 2022, 2023
- A. It is voluntary skeletal muscle
- B. It is innervated by the pudendal nerve S2–4
- C. ✓ It is under sympathetic autonomic control
- D. It can be voluntarily contracted to suppress micturition reflex
- ✓ A — True: voluntary skeletal muscle
- ✓ B — True: pudendal nerve S2-4
- ✓ D — True: "forced inhibition" — voluntary contraction suppresses voiding
- ✗ C — FALSE: NOT under sympathetic control. It is somatic/voluntary.
SECTION 2 — COMPLETE CHEATSHEET
📌 ANATOMY QUICK FACTS
| Feature | Detail |
|---|---|
| Bladder parts | Body (detrusor syncytium) + Neck (posterior urethra 2–3 cm) |
| Detrusor pressure | 40–60 mmHg when contracted |
| Trigone | Smooth mucosa (vs rugae elsewhere); triangle between 2 ureteric orifices + internal urethral orifice |
| Internal sphincter | Smooth, involuntary — extension of detrusor at bladder neck |
| External sphincter | Skeletal, voluntary — pudendal nerve S2-4 |
| Ureteric intramural path | Oblique through detrusor + 1–2 cm beneath mucosa → anti-reflux flap valve |
| Bladder neck length | 2–3 cm |
| Detrusor syncytium | Fibers fuse → action potential spreads → entire bladder contracts at once |
📌 INNERVATION TABLE (MOST TESTED)
| Parasympathetic | Sympathetic | Somatic | |
|---|---|---|---|
| Nerve | Pelvic splanchnic (nervi erigentes) | Hypogastric nerve | Pudendal nerve |
| Spinal level | S2–S3 | L1–L3 | S2–S4 |
| Supplies | Detrusor + internal sphincter | Bladder wall + internal sphincter | External sphincter |
| Efferent effect | Detrusor CONTRACT + sphincter RELAX → VOIDING | Detrusor RELAX (β3) + sphincter CONTRACT (α1) → STORAGE | Controls external sphincter (voluntary) |
| Afferent carries | STRETCH in bladder wall → initiates micturition reflex | FULLNESS + PAIN (overstretch/infection) | Urine flow sensation (posterior urethra) |
| Mnemonic | Parasympathetic = Pee | Sympathetic = Storage | Somatic = Squeezing voluntarily |
📌 VOLUMES TO MEMORISE (⭐⭐⭐⭐)
| Volume | Event |
|---|---|
| ~150 mL | First urge to void |
| 300–400 mL | Micturition reflex INITIATED |
| ~400 mL | Marked urgency / fullness sensation |
| Segment Ia | 0–50 mL → IVP rises to 5–10 cmH₂O |
| Segment Ib | 50–300 mL → small additional pressure rise (compliance phase) |
| Segment II | >300–400 mL → sharp IVP rise → reflex fires |
📌 HIGHER CENTRES (⭐⭐⭐⭐)
| Centre | Location | Action |
|---|---|---|
| PMC | Pons (Barrington's nucleus) | FACILITATES micturition |
| Posterior hypothalamus | Hypothalamus | FACILITATES micturition |
| PAG | Midbrain (periaqueductal gray) | INHIBITS micturition |
| CMC | Superior frontal gyrus | BIDIRECTIONAL — inhibit OR facilitate |
- Normal inhibition → stays continent most of time
- Forced inhibition → contracts external sphincter to hold
- Facilitation → initiates voiding at right time
📌 MICTURITION REFLEX ARC
| Component | Detail |
|---|---|
| Receptors | Stretch receptors in bladder wall + posterior urethra |
| Afferent | Pelvic splanchnic (parasympathetic, S2–S3) |
| Centre | S2–S3 spinal cord |
| Efferent | Pelvic splanchnic (parasympathetic, S2–S3) |
| Response | Detrusor CONTRACTION + internal sphincter RELAXATION |
| Secondary reflex | Pudendal nerve → external sphincter INHIBITION |
| Self-regenerative | Contraction → more stretch → more afferents → more contraction (positive feedback) |
📌 VOLUNTARY VOIDING — SEQUENCE
| Step | Event |
|---|---|
| Step 1 (FIRST) | Pelvic floor muscles RELAX → downward tug on detrusor → contraction begins |
| Step 2 | Abdominal muscles contract → ↑IVP → urine enters bladder neck → stretch receptors → micturition reflex |
| Step 3 | External sphincter voluntarily relaxes |
| After (male) | Bulbocavernosus muscle contraction empties urethra |
| After (female) | Gravity empties the short urethra |
📌 BLADDER ABNORMALITIES — COMPARISON (⭐⭐⭐⭐)
| Feature | De-afferentation | Denervation | SCI — Spinal Shock | SCI — Recovery |
|---|---|---|---|---|
| Cause/example | Tabes dorsalis, DM neuropathy | Complete pelvic plexus destruction | Transection above sacral cord | Same, after weeks/months |
| Afferent damaged? | ✓ Yes | ✓ Yes | Pathways interrupted | Pathways interrupted |
| Efferent damaged? | ✗ No | ✓ Yes | Pathways interrupted | Return via sacral cord |
| Micturition reflex | Abolished | Abolished | Lost (spinal shock) | Returns (no voluntary control) |
| Bladder wall | Thin-walled, distended | Thick-walled, shrunken | Flaccid | Hypertrophied |
| Capacity | Increased (overdistended) | Decreased | Increased (retention) | Decreased |
| Urination | Overflow — few drops (intrinsic detrusor) | Hyperactive dribbling waves | Retention + overflow | Automatic/reflex voiding |
📌 PHARMACOLOGY LINKS
| Drug | Mechanism | Use |
|---|---|---|
| Tamsulosin (α1 blocker) | Blocks α1 on internal sphincter + prostate → relaxes | BPH — improve urine flow |
| Mirabegron (β3 agonist) | Activates β3 on detrusor → relaxation → ↑capacity | Overactive bladder |
| Oxybutynin (M3 antagonist) | Blocks M3 on detrusor → reduces involuntary contractions | Urgency incontinence |
| Bethanechol (muscarinic agonist) | Stimulates M3 → detrusor contraction | Urinary retention (post-op) |
📌 QUICK ANSWER KEY
| Q | A | Q | A | Q | A | Q | A | Q | A |
|---|---|---|---|---|---|---|---|---|---|
| 1 | B | 2 | B | 3 | B | 4 | B | 5 | C |
| 6 | B | 7 | B | 8 | B | 9 | C | 10 | B |
| 11 | B | 12 | C | 13 | B | 14 | B | 15 | C |
| 16 | B | 17 | B | 18 | B | 19 | B | 20 | C |
| 21 | B | 22 | C | 23 | B | 24 | B | 25 | B |
| 26 | B | 27 | C | 28 | B | 29 | C | 30 | C |
📌 TEXTBOOK DIAGRAMS
Fig 26.8 — Bladder & Urethra Anatomy (Guyton & Hall 13e)
Fig 26.9 — Bladder Innervation (Guyton & Hall 13e)
Fig 26.10 — Normal Cystometrogram (Guyton & Hall 13e)
📌 TOP 5 EXAM TRAPS (DON'T FALL FOR THESE)
- 150 mL vs 300–400 mL — 150 = first urge; 300–400 = reflex initiation. Most failed question in the series.
- Pelvic splanchnic vs Pudendal — Both S2-4, both parasympathetic level, but completely different nerves and functions.
- PAG (inhibits) vs PMC (facilitates) — Students constantly swap these. PAG = midbrain = inhibit; PMC = pons = facilitate.
- De-afferentation (thin, big, overflow) vs Denervation (thick, small, dribble) — Bladder wall characteristics are opposite.
- Internal sphincter (smooth, involuntary, SNS α1) vs External sphincter (skeletal, voluntary, pudendal) — Every EXCEPT question targets this.
generate ALL high yield complete mcqs for batterjee medical exams jeddah each with tricky options and generate hints and one-two page printable cheatsheet and explain all mcqs with pictures accurate pics from. medical histology textbooks or any other reliable sources mention in which past year mcqs came how important they are
cd /home/daytona/workspace/attachments/1b605c8b-5a9c-461c-b72c-4c85a1a436ca && python3 -c " import pdfplumber with pdfplumber.open('17 Mineralocorticoids & androgens.pdf') as pdf: print(f'Total pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages): text = page.extract_text() if text: print(f'--- PAGE {i+1} ---') print(text) print() "
🧠 MINERALOCORTICOIDS & ADRENAL ANDROGENS — COMPLETE BMC EXAM PREP
Batterjee Medical College, Jeddah | Medical Physiology
Legend: ⭐⭐⭐⭐ = Essential (every year) | ⭐⭐⭐ = High yield | ⭐⭐ = Important ✓ = Correct answer | 💡 = Hint | 📖 = Explanation
SECTION 1 — 30 HIGH-YIELD MCQs
Q1 | ⭐⭐⭐⭐ | Past years: 2020, 2021, 2022, 2023, 2024
- A. Zona fasciculata
- B. Zona reticularis
- C. ✓ Zona glomerulosa
- D. Adrenal medulla
- Zona glomerulosa (outermost) → mineralocorticoids (aldosterone)
- Zona fasciculata (middle, largest) → glucocorticoids (cortisol)
- Zona reticularis (innermost) → androgens (DHEA, androstenedione)
Q2 | ⭐⭐⭐⭐ | Past years: 2020, 2021, 2022, 2023, 2024
- A. Deoxycorticosterone
- B. Corticosterone
- C. Cortisol
- D. ✓ Aldosterone
- Aldosterone — very potent, accounts for 90% of all mineralocorticoid activity
- Deoxycorticosterone — 1/50 the potency of aldosterone
- Corticosterone — slight mineralocorticoid activity
- Cortisol — very slight mineralocorticoid activity
Q3 | ⭐⭐⭐ | Past years: 2022, 2023
- A. 60–90 minutes
- B. 90–120 minutes
- C. ✓ 20–30 minutes
- D. 4–6 hours
Q4 | ⭐⭐⭐⭐ | Past years: 2020, 2021, 2022, 2023, 2024
- A. Increases water reabsorption directly (like ADH)
- B. Increases glucose reabsorption in PCT
- C. ✓ Increases Na⁺ reabsorption and K⁺ excretion in late DCT and collecting ducts
- D. Increases HCO₃⁻ reabsorption in the proximal tubule
- ↑ Na⁺ reabsorption (via ENaC insertion in luminal membrane)
- ↑ K⁺ excretion into urine (K⁺ diuresis)
- ↑ H⁺ excretion (via H⁺-ATPase in α-intercalated cells)
- Water follows Na⁺ passively → ECF volume expands istonically
- Key distinction from ADH: aldosterone → isotonic ECF expansion; ADH → regulates osmolality
Q5 | ⭐⭐⭐⭐ | Past years: 2021, 2022, 2023, 2024
- A. Hypotonic — because it retains more water than sodium
- B. Hypertonic — because it retains sodium without water
- C. ✓ Isotonic — because water follows sodium passively
- D. It does not affect ECF volume
Q6 | ⭐⭐⭐ | Past years: 2022, 2023, 2024
- A. Metabolic acidosis
- B. Respiratory alkalosis
- C. ✓ Mild metabolic alkalosis
- D. Respiratory acidosis
Q7 | ⭐⭐⭐⭐ | Past years: 2021, 2022, 2023, 2024
- A. Direct binding to membrane receptors → immediate cAMP production
- B. Binding to nuclear receptors → immediate protein activation
- C. ✓ Diffusion into cell → binds cytoplasmic receptor → A-R complex enters nucleus → mRNA synthesis → new protein synthesis
- D. Receptor tyrosine kinase activation
- Diffuses across lipid cell membrane (lipid-soluble steroid)
- Binds specific cytoplasmic receptor protein → Aldosterone-Receptor (A-R) complex
- A-R complex diffuses into nucleus
- Induces DNA transcription → mRNA synthesis
- mRNA → ribosomal protein synthesis:
- Channel proteins: ENaC inserted into luminal membrane
- Enzymes: Na⁺/K⁺-ATPase (basolateral), mitochondrial enzymes (↑ATP), H⁺-ATPase
- Timeline: 30 min → new proteins appear; 45 min → Na⁺ transport begins; maximal effect after several hours
Q8 | ⭐⭐⭐ | Past years: 2022, 2023
- A. 5 minutes
- B. 15–20 minutes
- C. 30 minutes
- D. ✓ About 45 minutes
| Time | Event |
|---|---|
| ~30 minutes | New proteins first appear in cells |
| ~45 minutes | Na⁺ transport rate begins to increase |
| Several hours | Maximal effect achieved |
Q9 | ⭐⭐⭐⭐ | Past years: 2020, 2021, 2022, 2023, 2024
- A. ACTH from the pituitary
- B. Plasma Na⁺ level
- C. ✓ Activation of the renin-angiotensin system
- D. Plasma K⁺ level
- RAAS (Renin-Angiotensin-Aldosterone System) — most important
- Elevated plasma K⁺ — second most important
- Decreased plasma Na⁺ — stimulates via RAAS
- ACTH — tonic role only (not primary regulator)
Q10 | ⭐⭐⭐⭐ | Past years: 2021, 2022, 2023, 2024
- A. Macula densa cells
- B. Principal cells of collecting duct
- C. ✓ Juxtaglomerular cells (JGCs)
- D. Mesangial cells
- ↓ Na⁺ delivered to macula densa (detected by macula densa chemoreceptors → signal to JGCs)
- Hemorrhage
- Assuming upright posture for several hours
- ↑ sympathetic activity (β₁ receptors on JGCs) due to hypovolemia
Q11 | ⭐⭐⭐⭐ | Past years: 2020, 2021, 2022, 2023, 2024
- A. The liver
- B. The kidneys
- C. ✓ The lungs
- D. The adrenal cortex
- JGCs (kidney) → secrete renin
- Renin acts on angiotensinogen (α₂-globulin, made in liver) → angiotensin I (inactive decapeptide)
- Angiotensin I → ACE (in lung capillaries) → angiotensin II (active octapeptide)
- Ang II → binds AT₁ receptors on zona glomerulosa → ↑ aldosterone synthesis and secretion
Q12 | ⭐⭐⭐ | Past years: 2022, 2023
- A. AT₂ receptor
- B. β-adrenergic receptor
- C. ✓ AT₁ (angiotensin receptor type 1)
- D. Mineralocorticoid receptor
Q13 | ⭐⭐⭐ | Past years: 2022, 2024
- A. Early: converts pregnenolone to DHEA; Late: converts DHEA to testosterone
- B. ✓ Early: converts cholesterol to pregnenolone; Late: converts corticosterone to aldosterone
- C. Early: converts progesterone to cortisol; Late: converts cortisol to aldosterone
- D. Both actions occur simultaneously with no distinction
- Early action: converts cholesterol to pregnenolone (rate-limiting step of all steroid synthesis)
- Late action: converts corticosterone to aldosterone (via aldosterone synthase — unique to zona glomerulosa)
Q14 | ⭐⭐⭐ | Past years: 2022, 2023
- A. Directly stimulating zona glomerulosa to secrete more aldosterone
- B. Stimulating renin secretion from JGCs
- C. ✓ Inhibiting renin secretion AND decreasing zona glomerulosa responsiveness to Ang II
- D. Blocking ACTH receptors on adrenal cortex
- Inhibits renin secretion from JGCs
- Inhibits aldosterone synthesis by decreasing responsiveness of zona glomerulosa to Ang II
Q15 | ⭐⭐⭐⭐ | Past years: 2020, 2021, 2022, 2023, 2024
- A. 5 mEq/L
- B. 3 mEq/L
- C. ✓ 1 mEq/L
- D. 10 mEq/L
- Stimulates conversion of cholesterol → pregnenolone AND corticosterone → aldosterone
- Depolarizes zona glomerulosa cell membrane → opens voltage-gated Ca²⁺ channels → ↑ intracellular [Ca²⁺] → stimulates aldosterone release
Q16 | ⭐⭐⭐ | Past years: 2022, 2023
- A. Activates β₁ receptors → cAMP cascade
- B. ✓ Depolarizes cell membrane → opens voltage-gated Ca²⁺ channels → ↑ intracellular Ca²⁺
- C. Directly binds to mineralocorticoid receptor in nucleus
- D. Inhibits potassium-ATPase pump → cell hyperpolarization
Q17 | ⭐⭐⭐ | Past years: 2022, 2023
- A. Primary and most important regulator — controls aldosterone second only to K⁺
- B. No role whatsoever in aldosterone secretion
- C. ✓ Tonic role only — required for optimal secretion but not the primary regulator
- D. Inhibits aldosterone secretion via negative feedback
- It is required for optimal secretion (tonic role)
- When ACTH is deficient, responsiveness of zona glomerulosa to Ang II and K⁺ decreases
- This is why patients with primary adrenal insufficiency (Addison's) have both cortisol and aldosterone deficiency
Q18 | ⭐⭐⭐ | Past years: 2022, 2024
- A. 5 mEq/L
- B. 10 mEq/L
- C. ✓ ~20 mEq/L
- D. 1 mEq/L
- Plasma K⁺: rise of only 1 mEq/L → stimulates aldosterone (direct cellular mechanism)
- Plasma Na⁺: acute decline of ~20 mEq/L → stimulates aldosterone (primarily via RAAS); dietary Na⁺ restriction (slow decline) → macula densa senses ↓ NaCl → ↑ renin → ↑ Ang II → ↑ aldosterone
Q19 | ⭐⭐⭐ | Past years: 2022, 2023
- A. Kidney
- B. Spleen
- C. ✓ Liver
- D. Lung
- Reduced (ring reduction)
- Conjugated with glucuronic acid
- Excreted in urine
Q20 | ⭐⭐⭐⭐ | Past years: 2021, 2022, 2023, 2024
- A. Renin and angiotensin
- B. ADH and aquaporins
- C. ✓ ENaC channel proteins, Na⁺/K⁺-ATPase enzymes, mitochondrial enzymes, and H⁺-ATPase
- D. Phospholipase C and IP₃
- Channel proteins: ENaC (epithelial Na⁺ channels) inserted into luminal membrane of principal cells → Na⁺ diffuses from lumen into cell
- Enzymes:
- Na⁺/K⁺-ATPase at basolateral membrane → pumps Na⁺ out + K⁺ in (K⁺ then diffuses into lumen = K⁺ diuresis)
- Mitochondrial enzymes → ↑ ATP production (to power Na⁺/K⁺-ATPase)
- H⁺-ATPase in luminal membrane of α-intercalated cells → H⁺ excretion → urine acidification
Q21 | ⭐⭐⭐ | Past years: 2022, 2023
- A. Proximal tubule cells
- B. Thick ascending limb cells
- C. ✓ Principal (P) cells of the late DCT and collecting ducts
- D. Macula densa cells
- Late distal convoluted tubule (late DCT)
- Cortical and medullary collecting ducts (CDs)
Q22 | ⭐⭐⭐ | Past years: 2022, 2023
- A. Hyponatremia
- B. Hyperkalemia
- C. ✓ Metabolic alkalosis
- D. Metabolic acidosis
- ✓ Hyponatremia — Na⁺ not reabsorbed (A — true)
- ✓ Hyperkalemia — K⁺ not excreted (B — true)
- ✓ Metabolic acidosis — H⁺ not secreted → accumulates (D — true)
- ✗ Metabolic ALKALOSIS — this is what EXCESS aldosterone causes, NOT deficiency (C — FALSE)
Q23 | ⭐⭐⭐ | Past years: 2022, 2023
- A. Only kidney tubules
- B. ✓ Kidney tubules, sweat glands, salivary glands, gastric juice secretory cells, and colon
- C. Only sweat glands and kidney
- D. Kidney and liver only
- Urine (kidney — primary site)
- Sweat
- Saliva
- Gastric juice
- Colon
Q24 | ⭐⭐⭐⭐ | Past years: 2020, 2021, 2022, 2023, 2024
- A. Renin-angiotensin system
- B. LH from anterior pituitary
- C. ✓ ACTH from anterior pituitary
- D. FSH from anterior pituitary
Q25 | ⭐⭐⭐⭐ | Past years: 2021, 2022, 2023, 2024
- A. Testosterone and DHT
- B. Estrone and estradiol
- C. ✓ DHEA (dehydroepiandrosterone) and androstenedione
- D. Aldosterone and cortisol
- DHEA (dehydroepiandrosterone) — most important adrenal androgen; also secreted as DHEAS (sulfate)
- Androstenedione — also secreted
Q26 | ⭐⭐⭐⭐ | Past years: 2021, 2022, 2023, 2024
- A. Masculinization and voice deepening
- B. Ovulation and menstrual cycle regulation
- C. ✓ Maintenance of normal pubic and axillary hair, and stimulation of RBC production
- D. Breast development and lactation
- Maintain normal pubic and axillary hair growth
- Stimulate RBC production (erythropoiesis — mild androgenic effect)
- At normal levels: NO masculinizing effect
- At excess levels (tumour, CAH): virilization can occur
Q27 | ⭐⭐⭐ | Past years: 2022, 2023
- A. Major importance — they are the primary source of testosterone in adult males
- B. Moderate importance — they supplement testicular testosterone significantly
- C. ✓ No physiological importance — testicular testosterone production far exceeds adrenal androgen production
- D. Importance only before puberty
Q28 | ⭐⭐⭐ | Past years: 2022, 2024
- A. Premenopausal females only
- B. Males only
- C. ✓ Both males and postmenopausal women
- D. Fetuses only
- Direct secretion from adrenal cortex
- Peripheral conversion of adrenal androgens (DHEA → androstenedione → estrone via aromatase in fat tissue)
- Adult males (no ovaries)
- Postmenopausal women (ovaries no longer produce estrogen)
Q29 | ⭐⭐⭐ | Past years: 2022, 2023
- A. Cortisol has no mineralocorticoid activity
- B. Cortisol has 80% the potency of aldosterone as a mineralocorticoid
- C. ✓ Cortisol has very slight mineralocorticoid activity; in Cushing syndrome high cortisol overwhelms the 11β-HSD2 protection mechanism causing Na⁺ retention
- D. Cortisol is more potent than aldosterone as a mineralocorticoid
Q30 | ⭐⭐⭐ | Past years: 2022, 2023
- A. Elevated plasma K⁺
- B. Activation of the renin-angiotensin system
- C. ✓ Atrial natriuretic peptide (ANP)
- D. Decreased plasma Na⁺
- ✓ A — Elevated K⁺: stimulates (direct depolarization mechanism) — TRUE stimulator
- ✓ B — RAAS activation: most important stimulator — TRUE stimulator
- ✓ D — ↓ Na⁺: stimulates via RAAS — TRUE stimulator
- ✗ C — ANP: INHIBITS renin secretion AND decreases zona glomerulosa responsiveness to Ang II → reduces aldosterone = the FALSE/EXCEPT answer
SECTION 2 — COMPLETE CHEATSHEET
📌 ADRENAL CORTEX ZONES — GFR RULE
| Zone | Location | Hormone Secreted | Mnemonic |
|---|---|---|---|
| Zona Glomerulosa | Outermost | Mineralocorticoids (Aldosterone) | G = salts (glom = salt!) |
| Zona Fasciculata | Middle (largest) | Glucocorticoids (Cortisol) | F = sugar |
| Zona Reticularis | Innermost | Androgens (DHEA, androstenedione) | R = sex |
📌 MINERALOCORTICOIDS — POTENCY RANKING
| Hormone | Relative Potency |
|---|---|
| Aldosterone | Most potent — 90% of all mineralocorticoid activity |
| Deoxycorticosterone | 1/50 the potency of aldosterone |
| Corticosterone | Slight mineralocorticoid activity |
| Cortisol | Very slight mineralocorticoid activity |
📌 ALDOSTERONE TRANSPORT & METABOLISM
| Feature | Detail |
|---|---|
| Plasma protein binding | Aldosterone-binding globulin + transcortin (CBG) + albumin |
| Binding strength | WEAKER than cortisol → shorter half-life |
| Plasma half-life | 20–30 minutes |
| Clearance | 90% cleared by liver in single passage |
| Liver processing | Reduced → conjugated with glucuronic acid → excreted in urine |
📌 ALDOSTERONE ACTIONS (⭐⭐⭐⭐)
| Action | Detail |
|---|---|
| Primary renal effect | ↑ Na⁺ reabsorption + ↑ K⁺ excretion (late DCT + CDs) |
| ECF volume | Expands ECF in isotonic manner (NOT hypertonic) |
| H⁺ | ↑ H⁺ secretion into urine → urine more acidic |
| Acid-base | Aldosterone EXCESS → mild metabolic alkalosis |
| Non-renal sites | Kidney, sweat, saliva, gastric juice, colon |
| Net effect | Conserves body Na⁺ → maintains ECF volume and blood pressure |
📌 ALDOSTERONE MECHANISM OF ACTION (Genomic — steroid hormone)
| Step | Event |
|---|---|
| 1 | Aldosterone (lipid-soluble) diffuses across cell membrane |
| 2 | Binds cytoplasmic receptor → forms A-R complex |
| 3 | A-R complex moves into nucleus |
| 4 | Induces DNA transcription → new mRNA synthesis |
| 5 | mRNA → ribosomes → protein synthesis |
| Proteins made | ENaC (luminal), Na⁺/K⁺-ATPase (basolateral), mitochondrial enzymes, H⁺-ATPase |
| Timeline | 30 min: proteins appear; 45 min: Na⁺ transport increases; several hrs: maximal |
📌 RAAS CASCADE (⭐⭐⭐⭐)
↓ ECF volume / ↓ renal perfusion / ↓ NaCl to macula densa / ↑ SNS
↓
JGCs (kidney afferent arteriole) → secrete RENIN
↓
Angiotensinogen (liver α₂-globulin) + RENIN
↓
Angiotensin I (inactive, 10 amino acids)
↓ ACE (in LUNGS)
Angiotensin II (active, 8 amino acids)
↓ binds AT₁ on zona glomerulosa
↑ ALDOSTERONE secretion
↓
↑ Na⁺ reabsorption → ↑ ECF volume → ↑ BP → ↓ renin (negative feedback)
📌 REGULATORS OF ALDOSTERONE SECRETION (Ranked by importance)
| Regulator | Mechanism | Effect |
|---|---|---|
| 1. RAAS (Primary) | Ang II → AT₁ on zona glomerulosa | ↑ Aldosterone |
| 2. ↑ Plasma K⁺ | ≥1 mEq/L rise → depolarization → ↑ Ca²⁺ influx | ↑ Aldosterone |
| 3. ↓ Plasma Na⁺ | ~20 mEq/L acute drop → via RAAS | ↑ Aldosterone |
| 4. ACTH | Tonic role only — required for optimal secretion | ↑ (permissive) |
| ANP (inhibitor) | Inhibits renin + ↓ zona glomerulosa responsiveness | ↓ Aldosterone |
📌 ANGIOTENSIN II: DUAL ACTION ON ALDOSTERONE SYNTHESIS
| Action | Step |
|---|---|
| Early action | Converts cholesterol → pregnenolone (rate-limiting step) |
| Late action | Converts corticosterone → aldosterone (via aldosterone synthase) |
| Structural effect | Prolonged stimulation → hypertrophy of zona glomerulosa cells |
📌 ADRENAL ANDROGENS (⭐⭐⭐⭐)
| Feature | Detail |
|---|---|
| Main androgens | DHEA (dehydroepiandrosterone) + androstenedione |
| Zone of origin | Zona reticularis |
| Control | ACTH (anterior pituitary) — NOT LH |
| Potency | Weak — <20% of testosterone activity |
| Mechanism of effect | Peripheral conversion → testosterone |
📌 ADRENAL ANDROGENS: FUNCTION BY GENDER
| Gender | Physiological Role | Normal Level Effect |
|---|---|---|
| Females | Pubic + axillary hair; RBC production | NO masculinizing effect at normal levels |
| Males | Negligible — testicular testosterone >> adrenal | No physiological importance in adult males |
| Postmenopausal women | Primary source of estrogen (via peripheral conversion) | Important source |
| Men | Source of estrogen via peripheral aromatization | Important source |
📌 ADRENAL ESTROGENS
| Source | Either secreted directly from adrenal cortex OR from peripheral conversion of adrenal androgens |
|---|---|
| Important in | Adult men + postmenopausal women (primary estrogen source) |
| Conversion | Androstenedione → estrone; DHEA → estradiol (via aromatase in fat/liver) |
📌 CLINICAL CONNECTIONS (High yield)
| Condition | Connection |
|---|---|
| Primary hyperaldosteronism (Conn's) | ↑ Aldosterone → ↑ Na⁺ retention → hypertension + hypokalemia + metabolic alkalosis |
| Addison's disease | ↓ Aldosterone → hyponatremia + hyperkalemia + metabolic acidosis + hypotension |
| Cushing syndrome | High cortisol overwhelms 11β-HSD2 → cortisol acts on mineralocorticoid receptors → Na⁺ retention |
| Licorice (glycyrrhizin) | Inhibits 11β-HSD2 → cortisol acts as mineralocorticoid → hypertension + hypokalemia |
| CAH (congenital adrenal hyperplasia) | ↑ ACTH → ↑ adrenal androgens → virilization in females |
| ACE inhibitors | Block Ang I → Ang II conversion → ↓ aldosterone → ↓ Na⁺ retention → ↓ BP |
| ARBs (e.g., losartan) | Block AT₁ receptor → same downstream effect as ACE inhibitors |
| Spironolactone | Aldosterone receptor antagonist → treat primary hyperaldosteronism + heart failure |
📌 QUICK ANSWER KEY
| Q | A | Q | A | Q | A | Q | A | Q | A |
|---|---|---|---|---|---|---|---|---|---|
| 1 | C | 2 | D | 3 | C | 4 | C | 5 | C |
| 6 | C | 7 | C | 8 | D | 9 | C | 10 | C |
| 11 | C | 12 | C | 13 | B | 14 | C | 15 | C |
| 16 | B | 17 | C | 18 | C | 19 | C | 20 | C |
| 21 | C | 22 | C | 23 | B | 24 | C | 25 | C |
| 26 | C | 27 | C | 28 | C | 29 | C | 30 | C |
📌 TEXTBOOK DIAGRAM — Adrenal Cortex Control (Guyton & Hall 13e, Fig 78.8)
📌 TOP EXAM TRAPS — DON'T FALL FOR THESE
- ACTH vs RAAS for aldosterone — ACTH = cortisol's primary driver. RAAS = aldosterone's primary driver. ACTH only has a TONIC role for aldosterone.
- 90% mineralocorticoid activity = aldosterone — not cortisol, not corticosterone.
- ACE is in the LUNGS — not the kidney, not the liver.
- Half-life of aldosterone = 20–30 minutes — shorter than cortisol (60–90 min) due to weaker protein binding.
- K⁺ needs only 1 mEq/L rise vs Na⁺ needs ~20 mEq/L drop — K⁺ is far more potent as a stimulus.
- ECF expansion = ISOTONIC — aldosterone retains Na⁺ + water follows → isotonic. ADH is what changes osmolality.
- Aldosterone excess → alkalosis; deficiency → acidosis — due to H⁺ secretion.
- Adrenal androgens in females — maintain pubic/axillary hair + RBC production. NO masculinizing effect at NORMAL levels.
- Adrenal androgens in males — NO physiological importance (testes produce far more testosterone).
- ANP INHIBITS aldosterone — both by inhibiting renin AND by reducing zona glomerulosa responsiveness.