Explain Anatomical and Physiological aspects of Puberty and Menopause. Explain neuroendocrinology with respect to puberty - hormon
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a thorough, well-structured answer. Here is the comprehensive response:
Puberty and Menopause: Anatomical, Physiological, and Neuroendocrine Aspects
Part 1 - PUBERTY
Definition and Overview
Puberty is the transitional period during which an individual becomes capable of reproduction - the final maturation of the reproductive system that was structurally in place since birth. Two distinct physiological processes operate in parallel:
- Gonadarche - physical and functional maturation of the gonads (production of gametes and sex steroids)
- Adrenarche - increased production of androgenic steroids (DHEA, DHEAS, androstenedione) by the adrenal cortex
Adrenarche is peculiar to humans and great apes. It occurs at ages 6-8 years in both sexes and precedes gonadarche. It induces pubarche (pubic hair growth) but is not required for reproductive competence - its exact function remains unclear.
- Medical Physiology (Boron & Boulpaep), p. 1587
Neuroendocrinology of Puberty - The Hormonal Cascade
This is the most complex and clinically important aspect. The entire sequence is orchestrated by a hierarchical neuroendocrine axis:
Hypothalamus → Anterior Pituitary → Gonads → Target Organs
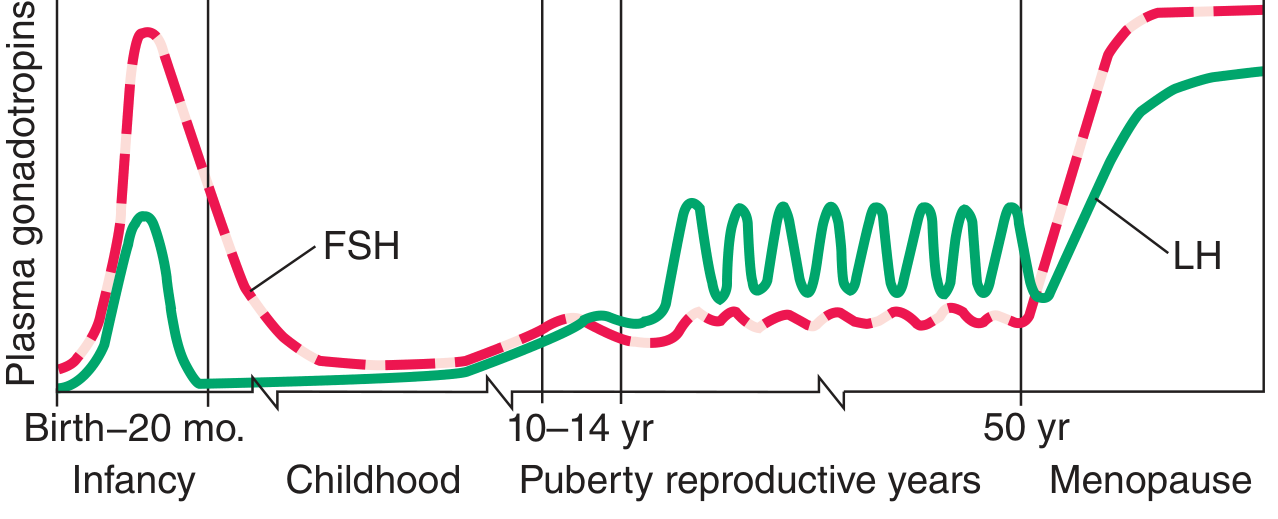
The diagram above shows how gonadotropin levels peak in infancy, remain quiescent throughout childhood, rise again at puberty, cycle during reproductive years, then surge dramatically at menopause.
Step 1: The GnRH Pulse Generator
The master switch for puberty is in the arcuate nucleus of the medial basal hypothalamus. A population of GnRH neurons here has an intrinsic pulsatile secretory rhythm of approximately one pulse per hour. During childhood, this pulse generator is actively suppressed.
Why is it suppressed before puberty?
During the prepubertal period, even tiny circulating levels of sex steroids are sufficient to exert negative feedback on the hypothalamic-pituitary system and block gonadotropin release. The gonadostat is exquisitely sensitive. At puberty, this sensitivity decreases - higher and higher steroid levels are needed to suppress the axis.
- Medical Physiology, p. 1588
Step 2: The Kisspeptin-NKB-Dynorphin (KNDy) System
The molecular "brake" and "accelerator" on the GnRH pulse generator have now been identified:
The KNDy Neuron System (Arcuate Nucleus):
| Molecule | Gene | Source | Action on GnRH |
|---|---|---|---|
| Kisspeptin | KISS1 | KNDy neurons, arcuate & preoptic | Potent STIMULATOR via GPR54/KISS1R |
| Neurokinin B (NKB) | TAC3 | KNDy neurons | Stimulates kisspeptin release |
| Dynorphin | PDYN | KNDy neurons | Inhibits kisspeptin (kappa opioid receptors) |
| GABA | - | Higher brain centers | Major INHIBITOR of GnRH neurons; represses kisspeptin |
| Glutamate (NMDA) | - | Higher centers | Excitatory; activates kisspeptin neurons |
At puberty onset: KISS1 and KISS1R transcripts are upregulated in the hypothalamus. Simultaneously, tonic GABA inhibition decreases, releasing the brake. Glutamatergic (NMDA) input to kisspeptin neurons strengthens. The net result: a surge in kisspeptin secretion that drives pulsatile GnRH release.
"At puberty, GnRH secretion and pulse frequency increase, mainly due to increased activity of kisspeptin neurons and reduction in tonic GABA inhibition." - Medical Physiology, p. 1624
The critical KISS1R/GPR54 evidence: Patients with loss-of-function mutations in GPR54 (the kisspeptin receptor) fail to enter puberty. This was the key experiment establishing kisspeptin as the essential gate-keeper of reproductive onset.
Epigenetic switch: Two imprinted genes, MKRN3 and DLK1, identified in families with central precocious puberty, are thought to maintain epigenetic repression of kisspeptin neurons during childhood. Their silencing (imprinting relaxation) may represent the molecular switch that initiates puberty.
- Harrison's Principles of Internal Medicine 22E, p. 544-554
Step 3: GnRH Pulsatility and the Pituitary Response
The earliest detectable sign of puberty - even before physical signs appear - is the onset of pulsatile LH and FSH secretion during REM sleep. These sleep-associated pulses eventually occur throughout the day as puberty advances.
GnRH is released in pulses into the hypothalamic-pituitary portal system and binds gonadotrophs in the anterior pituitary. The pulsatile nature is mandatory:
- Pulsatile GnRH → upregulates GnRH receptors → FSH and LH secretion
- Continuous (non-pulsatile) GnRH → downregulates GnRH receptors → suppresses FSH and LH (the principle behind GnRH agonist therapy for precocious puberty)
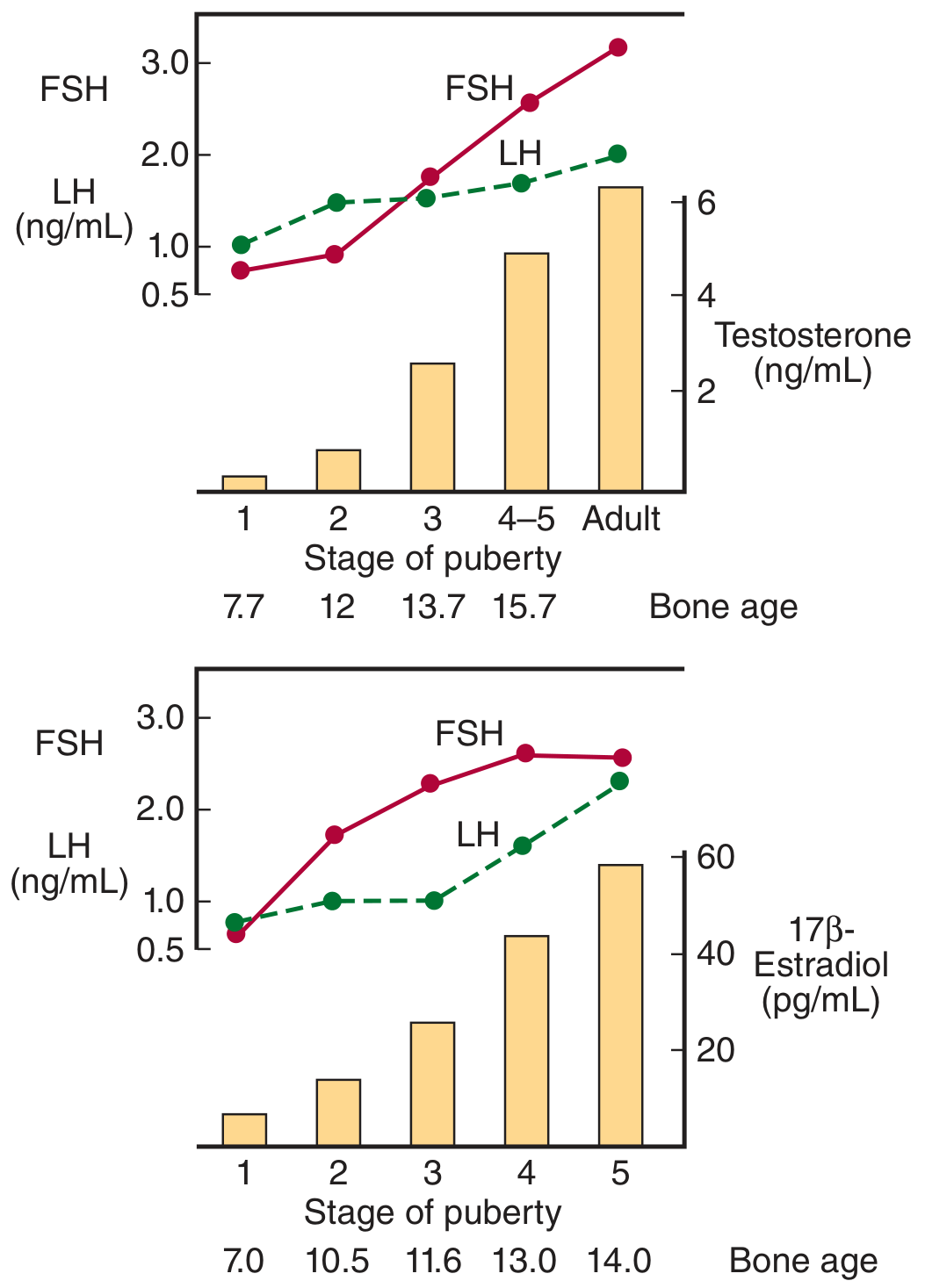
In boys (top panel), testosterone rises steeply from Tanner stage 2 onward. In girls (bottom panel), 17β-estradiol rises progressively, reaching peak levels at Tanner stage 5.
Step 4: Role of Leptin - Metabolic Gating of Puberty
Leptin (from adipocytes) plays a permissive but not sufficient role:
-
ob/ob mice lacking leptin are infertile; leptin injections restore fertility
-
Girls with anorexia nervosa or intensive athletic training lose body fat → leptin falls → GnRH suppressed → amenorrhea ("going back through puberty in reverse")
-
Leptin signals the hypothalamus that adequate energy stores exist to support reproduction
-
Ganong's Review of Medical Physiology, 26th Ed., p. 402
Anatomical Changes at Puberty
Tanner Staging System
Puberty is clinically staged using the Tanner (sexual maturity rating) stages 1-5, assessed separately for:
- Public hair (both sexes)
- Genital development (males)
- Breast development (females)
Stage 1 = prepubertal; Stage 5 = adult
Key hormones driving anatomical change:
| Change | Hormone Responsible |
|---|---|
| Testicular growth (primary sign in males) | FSH (Sertoli cells), LH (Leydig cells → testosterone) |
| Penile growth, scrotal pigmentation | Testosterone (via DHT) |
| Breast development (thelarche) | Estrogens |
| Pubic/axillary hair | Androgens (adrenal + gonadal) |
| Uterine/vaginal growth | Estrogens |
| Voice deepening (male) | Testosterone → laryngeal cartilage growth, vocal cord lengthening ~50% |
| Linear growth spurt | GH + IGF-1 + sex steroids |
| Epiphyseal fusion (stops growth) | Estrogens (even in males, via aromatization of testosterone) |
Male Puberty - Sequence and Anatomy
- First sign: Testicular enlargement >2.5 cm (Tanner 2), driven by FSH stimulating Sertoli cell proliferation. Testicular volume reaches ~3 mL.
- Testosterone secretion rises as LH stimulates Leydig cells.
- Spermarche (onset of sperm production) follows at ~13-14 years.
- Pubertal growth spurt occurs late in male puberty - average gain of 28 cm in height.
- Adult males have 150% the lean and skeletal mass of women, twice the muscle cell number.
- Body composition shifts: loss of fat, dramatic increase in muscle mass.
Female Puberty - Sequence and Anatomy
In girls, the sequence is:
- Thelarche (breast bud development, ~8-13 years) - first sign
- Pubarche (pubic and axillary hair)
- Growth spurt (occurs earlier in girls than boys - mid-puberty)
- Menarche (first menstrual period, ~12.5 years average in the USA)
- Initial cycles are typically anovulatory
- Regular ovulation appears approximately 1 year later
Estrogen causes:
- Uterine and vaginal growth; cornification of vaginal epithelium
- Growth and maturation of fallopian tubes
- Fat deposition (hips, buttocks, breasts)
- Women end up with 200% of men's body fat percentage
Androgens (adrenal): pubic and axillary hair, apocrine gland development, mild acne.
Factors Controlling Timing of Puberty
-
Genetic: Strong hereditary component - mother-daughter concordance in age of menarche
-
Nutrition/Body fat: Better nutrition → earlier puberty (secular trend: age of menarche has fallen 1-3 months per decade over 175 years in Europe and the USA)
-
Leptin: Permissive signal from fat tissue
-
Geography: Proximity to equator and lower altitude correlate with earlier puberty
-
Exercise/Stress: Heavy exercise and severe obesity both delay puberty
-
Light exposure: Seasonal and light-cycle effects via pineal/melatonin pathways
-
Medical Physiology, p. 1589; Ganong's, p. 402
Part 2 - MENOPAUSE
Definition
Menopause (also called the climacteric) is the permanent cessation of menstrual cycles and reproductive function in women, resulting from the depletion of ovarian follicular reserve. It is defined retrospectively as 12 consecutive months of amenorrhea without other cause. In the USA, mean age is ~51.5 years.
- Medical Physiology, p. 1643
Anatomical Basis - Follicular Depletion
The fundamental anatomical event is the progressive, irreversible loss of primordial follicles:
| Life Stage | Approximate Oocyte/Follicle Count |
|---|---|
| 20 weeks gestation | ~6-7 million oogonia |
| Birth | ~1-2 million |
| Puberty | ~300,000 |
| Age 37-38 | ~25,000 (accelerated loss begins) |
| Menopause | Virtually zero |
The massive loss of oocytes throughout reproductive life occurs through atresia - programmed apoptosis of follicles that do not ovulate. Of the ~300,000 follicles at puberty, only ~400 actually ovulate during a woman's lifetime.
By the late perimenopausal stage, the ovary contains only occasional secondary follicles and a few primary follicles in a prominent stroma. Post-menopausally, the ovary becomes a small, fibrotic, streak-like structure.
- Medical Physiology, p. 1643; Guyton & Hall, p. 1027
Neuroendocrinology and Hormonal Changes at Menopause
The hormonal sequence:
- FSH rises first - even as early as age 35, rising FSH is detected because of decreased folliculogenesis → decreased inhibin B and estradiol production → loss of negative feedback on FSH gonadotrophs
- Inhibin B falls - produced by granulosa cells; its fall removes a major pituitary brake on FSH specifically
- Estradiol and progesterone fall to very low levels:
- Estradiol: generally <30 pg/mL (vs. 200-400 pg/mL mid-cycle in reproductive years)
- Progesterone: often <1 ng/mL
- FSH and LH rise dramatically - higher than even the mid-cycle LH surge - representing the futile attempt of the hypothalamic-pituitary axis to stimulate the depleted ovary
- The anterior pituitary continues to respond to GnRH; gonadotrophs remain functional. The failure is ovarian, not pituitary or hypothalamic.
"Because the output of estrogens, progestins, and inhibins from the ovaries falls to very low levels during menopause, negative feedback on the hypothalamic-pituitary-ovarian axis becomes minimal. As a result, levels of FSH and LH may be higher than those seen during the mid-cycle surge in premenopausal women." - Medical Physiology, p. 1644
Androstenedione: Ovarian production becomes minimal at menopause, but adrenal androstenedione secretion remains relatively normal. Peripheral aromatization (in adipose tissue) of adrenal androstenedione to estrone becomes the main source of estrogen post-menopausally - explaining why obesity in post-menopausal women is associated with higher estrogen levels and endometrial cancer risk.
- Guyton & Hall, p. 1027-1028
Clinical Manifestations (Menopausal Syndrome)
The characteristic symptoms are primarily due to estrogen deficiency:
| Acute Symptoms (Menopausal Syndrome) | Long-Term Physical Changes |
|---|---|
| Vasomotor instability - hot flashes | Atrophy of vaginal epithelium |
| Night sweats | Changes in vaginal pH (less acidic → infection risk) |
| Mood changes, irritability | Decreased vaginal secretions and circulation |
| Sleep disturbances | Pelvic relaxation, loss of vaginal tone |
| Short-term memory difficulties | Cardiovascular disease (loss of estrogen's cardioprotective effects) |
| Headaches | Osteoporosis (estrogen normally inhibits osteoclast activity) |
| Loss of libido | Alzheimer disease risk increase |
| Psychic dyspnea | Urogenital atrophy |
- Medical Physiology, Table 55-3, p. 1643
Hot flashes are caused by estrogen withdrawal disrupting the hypothalamic thermoregulatory center - GnRH pulses synchronize with sudden peripheral vasodilation and sweating.
Perimenopause (Menopausal Transition)
The perimenopausal period begins several years before the final menstrual period:
- Cycles become irregular in frequency and length
- Anovulatory cycles become common
- FSH rises (detectable as early as age 35)
- Luteal phase defects (insufficient progesterone)
- Eventually, cycles cease entirely
Hormone Replacement Therapy (HRT)
Estrogen replacement effectively:
- Relieves vasomotor symptoms
- Prevents osteoporosis
- Potentially reduces Alzheimer and cardiovascular risk (if started early - "timing hypothesis")
Why progestins are added: Unopposed estrogen stimulates endometrial proliferation and risks endometrial hyperplasia/carcinoma. Progestins are omitted in women who have had hysterectomies.
Current guidance: If HRT is started before age 60, or within 10 years of menopause onset, benefits (symptom relief, bone protection) likely outweigh risks for women with low baseline cardiovascular and breast cancer risk.
SERMs (Selective Estrogen Receptor Modulators): Compounds like raloxifene and tamoxifen act as estrogen agonists in bone and cardiovascular tissue but as antagonists in breast and uterine tissue - potentially offering bone protection without carcinogenic risk.
- Medical Physiology, p. 1644; Guyton & Hall, p. 1028
Summary Comparison: Puberty vs. Menopause
| Feature | Puberty | Menopause |
|---|---|---|
| Trigger | Kisspeptin/KNDy disinhibition of GnRH pulse generator | Follicular exhaustion → loss of estrogen/inhibin negative feedback |
| FSH/LH | Rise progressively | Rise dramatically (very high) |
| Estrogens | Rise (estradiol from granulosa cells) | Fall to near zero |
| GnRH | Pulsatility activated | Pulsatility continues but ovary cannot respond |
| Kisspeptin | Upregulated - initiates axis | Still active but no follicles to stimulate |
| Anatomy | Growth of gonads and secondary sex organs | Atrophy of gonads and reproductive organs |
| Ovarian follicles | ~300,000 at onset | Virtually zero |
| Clinical outcome | Reproductive competence achieved | Reproductive competence lost |
Sources:
- Medical Physiology (Boron & Boulpaep), Chapters 53 and 55
- Guyton and Hall Textbook of Medical Physiology, Chapter 82
- Ganong's Review of Medical Physiology, 26th Edition, Chapter 22
- Harrison's Principles of Internal Medicine 22E, Chapter 404
This is a shared conversation. Sign in to Orris to start your own chat.